
Abstract
Aim
Cardiovascular disease (CVD) is a leading cause of death in both men and women. Type 1 and 2 diabetes mellitus (DM1 and DM2) are well-known risk factors for CVD. In addition, gestational diabetes mellitus (GDM) is a female sex-specific risk factor for CVD. Here, we measure circulating concentrations of cardiac troponin T (cTNT), N-terminal pro-B-type natriuretic peptide (NT-proBNP) and growth differentiation factor 15 (GDF-15) during pregnancy—a window of time often referred to as a cardiovascular stress test for women.
Methods
This study utilized data from 384 pregnant women: 64 with DM1, 16 with DM2, 35 with GDM and 269 euglycemic controls. Blood was predominantly sampled within a week before delivery. Cardiovascular biomarker concentrations were measured in serum using electrochemiluminescence immunoassay.
Result
Circulating cTnT levels were higher in women with DM1, DM2 and GDM as compared to controls, whereas NT-proBNP and GDF-15 levels were only increased in women with DM1. Glucose dysregulation, assessed by third trimester HbA1c levels, positively correlated with all three CVD biomarker levels, whereas pregestational body mass index correlated negatively with GDF-15.
Conclusions
Our results support the presence of myocardial affection in women with diabetic disorders during pregnancy. Although pregestational DM1 in this study was associated with the most adverse CVD biomarker profile, women with GDM displayed an adverse cTnT profile similar to what we found in women with pregestational DM2. This supports that women with GDM should be offered long-term intensified cardiovascular follow-up and lifestyle advice following delivery, similarly to the well-established CV follow-up of women with pregestational DM.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cardiovascular disease (CVD) remains a leading cause of death in both men and women, but sex-specific mechanisms and risk factors have so far been underinvestigated [1]. A recent review summarizes that pathophysiologic mechanisms in diet-induced obesity and cardiometabolic disorders (i.e., heart failure, atrial fibrillation and ischemic heart disease) affect women and men’s hearts differently [2]. Diabetes mellitus (DM) is a cardiovascular disease (CVD) risk factor that affects both sexes [3], but is particularly worrisome for women [4,5,6]. Pregnancy represents a female sex-specific risk for developing diabetes, as women may develop gestational diabetes mellitus (GDM) during pregnancy. GDM resolves postpartum but confers a high risk for developing diabetes mellitus type 2 (DM2) later in life [7, 8]. In order to screen for DM2 development, current clinical guidelines therefore recommend a postpartum HbA1c test in women after GDM (e.g., 4 months after delivery) followed by annual HbA1c testing [9, 10]. Insulin resistance (i.e., DM2 and GDM) and CVD may be linked by several underlying factors, such as obesity, inflammation, endothelial dysfunction, hypertension and dyslipidemia. However, DM1 also confers increased cardiovascular risk [3], and DM1 and DM2 are associated with loss of cardiac innervation [11], as well as interstitial collagen deposits, resulting in cardiac wall stiffening and diastolic dysfunction [12]. In addition, heart disease generally manifests in different ways in diabetics and non-diabetics [13], further implicating a causal relationship between diabetes and cardiovascular disease.
In order to combat the high and increasing societal burden of CVD, it is necessary to develop ways of accurately identifying individuals at risk during the preclinical period. This includes developing less invasive methods to determine future or ongoing cardiac stress. We have previously shown that commonly used cardiovascular risk calculators are inadequate in assessing cardiovascular disease risk one-year postpartum following GDM [14]. In addition to blood pressure, blood lipids and exercise tests, molecular biomarkers such as circulating cardiac troponin T (cTnT) [15], N-terminal pro-B-type natriuretic peptide (NT-proBNP) [16] and growth-differentiation factor 15 (GDF-15) [17] are valuable tools in the diagnosis of preclinical heart disease. Sex-specific cut-off values for cTnT and NT-proBNP that may be used for simplified detection of preclinical cardiac disease are still lacking [2]. This despite well-known differences in levels between women and men [18] and an increased prognostic value of these markers in women [19, 20].
Soluble fms-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PlGF) are predominantly expressed by the placenta during pregnancy. The antiangiogenic sFlt-1 is a decoy receptor for the proangiogenic PlGF [21]. Thus, the relative circulating levels of sFlt-1 and PlGF reflects the pregnant woman’s angiogenic profile, and we argue that a high sFlt-1/PlGF ratio is a marker of syncytiotrophoblast stress and general placental dysfunction [22].
Pregnancy has been described as a cardiovascular stress test [23], and may thus serve as an opportunity to identify women at risk for diabetes and premature cardiovascular disease. Early identification of women at risk provides opportunities for more intensified follow-up and preventive measures, at a young age where initial vascular changes (i.e., early stages of atherosclerosis) may be more reversible. Here, we measure circulating concentrations of cTnT, NT-proBNP and GDF-15 in women with DM1, DM2 or GDM during pregnancy, and compare these to healthy control pregnant women. We hypothesized that the epidemiological excessive risk of premature CVD among women with diabetes—especially DM1—will be reflected by CVD risk biomarkers during pregnancy.
Methods
Study subjects
As previously described [24], women who had not yet gone into active labor were recruited to the Oslo Pregnancy biobank (OPB) [25], either upon admission for cesarean section or as outpatients followed up for pregnancy complications during the second half of pregnancy. Recruitment in pregnancy was mainly restricted by availability of study personnel, as almost none of the women approached declined participation. We included 384 women from the OPB prior to delivery: 64 with DM1, 16 with DM2, 35 with GDM and 269 euglycemic women (controls). Only women with singleton pregnancies, and no history of hypertension or other inflammatory diseases (e.g., autoimmunity or cancer) were included. Diabetes mellitus (DM) was defined according to the World Health Organization criteria at the time of inclusion [26], and diagnoses were retrieved from the individual medical charts. The patients with pregestational diabetes attended antenatal follow-up at the Oslo University Hospital according to routine, with assessment by endocrinologist, obstetrician and midwife.
The in-patient hospital blood pressure (BP) was based on repeated measurements with a validated device for pregnancy (Dinamap Pro, 100VE, GE Medical Systems Information Technology, Inc. Milwaukee, Wisconsin, USA), as previously described [14]. Offspring sex and gestational age specific birth weight percentiles were calculated according to Norwegian ultrasound-based percentiles [27].
Biomarker measurement
All maternal pregnancy blood samples were drawn predominantly within a week prior to delivery. Median gestational age at sampling was 37 + 0 for women with DM1, 37 + 1 for women with DM2, 38 + 5 for women with GDM and 39 + 0 for euglycemic controls (Table 1). Serum blood samples were thawed and analyzed for levels of cTnT, NT-proBNP and GDF-15 at the department for Multidisciplinary Laboratory Medicine and Medical Biochemistry at Akershus University Hospital, using electrochemiluminescence immunoassay Elecsys on the cobas e 801 platform (Roche Diagnostics, Rotkreuz, Switzerland). For cTnT, NT-proBNP and GDF-15 measuring ranges were 3–100,000 ng/L, 5–35,000 ng/L and 400–20,000 ng/L, respectively. Samples with GDF-15 levels > 20,000 ng/L were diluted 1:20 and reanalyzed. Biomarker values above or below measuring ranges were set to maximum or minimum possible measuring value, respectively. HbA1c vas available from the third trimester in 62 women with DM1, 15 with DM2, 33 with GDM and 3 controls.
The maternal PIGF and sFlt-1 serum concentrations from predelivery blood samples were quantified at the Department of Medical Biochemistry, Oslo University Hospital, on a cobas e 801 (Roche Diagnostics, Rotkreuz, Switzerland), using the fully automated Elecsys PlGF and sFlt-1 system, according to the manufacturer´s instructions.Footnote 1 Alternatively, the PlGF and sFlt-1 proteins were measured by the same Roche reagents, using an Elecsys 2010 Modular Analytics E170 or a cobas e 601 (Roche Diagnostics, Rotkreuz, Switzerland). All concentrations were within the measuring ranges of the PlGF and sFlt-1 assays (3–10,000 pg/mL and 10–85,000 pg/mL, respectively). The coefficients of variation were ≤ 2.1% for PlGF and ≤ 1.8% for sFlt-1.
Statistical analysis
Continuous variables are presented as medians and interquartile ranges and categorical variables as counts (percent). Comparisons between groups were conducted using the nonparametric Mann–Whitney U test for continuous variables and the Fisher’s exact test for categorical variables. Spearman’s rank correlation was used to assess the relationships between HbA1c and cardiovascular biomarkers. Statistical analyses were performed using SPSS version 22.0 (IBM). The level of significance was set at p < 0.05.
Results
Pregnancy phenotypes and placenta-cardiovascular biomarkers
Descriptive statistics as well as biomarker levels during pregnancy are shown in Table 1. The groups of women with DM1, DM2 and GDM had higher prepregnancy BMI as well as higher BMI at delivery, when compared to controls. The group with GDM also had a higher proportion of obese women (BMI ≥ 30 kg/m2). Median birthweight percentiles were higher in the DM1 and GDM groups as compared to controls. At delivery, women with DM1 or DM2 had higher median systolic and diastolic blood pressures as compared to controls, as well as significantly higher prevalences of hypertension (systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg).
When compared to controls, cTnT was higher in DM1, DM2 and GDM, while NT-proBNP and GDF-15 were only significantly higher in DM1. Women with DM1 also had significantly higher levels of cTnT (p < 0.001) and NT-proBNP (p < 0.001) than women with GDM.
As expected, women with hypertension at inclusion (systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg) had significantly higher levels of cTnT (p < 0.001), NT-proBNP (p < 0.001) and GDF-15 (p = 0.012, Supplemental Fig. 1). Elevated cTnT and NT-proBNP, but not GDF-15, levels were associated with hypertension when women with diabetes and controls were analyzed separately as well (results not shown).
Among women with diabetes, BMI before pregnancy was negatively correlated with NT-proBNP (rs = − 0.261, p = 0.005) and GDF-15 (rs = − 0.241, p = 0.010). Among controls, BMI before pregnancy was only negatively correlated with GDF-15 (rs = − 0.167, p = 0.006). Moreover, pregestational obesity (BMI ≥ 30 kg/m2 before pregnancy) was associated with significantly lower levels of GDF-15 among diabetics (p = 0.009, Supplemental Fig. 2) and controls (p = 0.006, Supplemental Fig. 3).
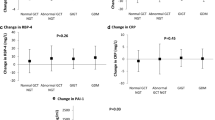
Norwegian guidelines for glucose control during pregnancy recommend a third trimester HbA1c level below 6% (42 mmol/mol) for women with pregestational diabetes [28]. In our cohort, most of the women had HbA1c levels above this goal; 46 of 62 with DM1, 13 of 15 with DM2 and 11 of 33 with GDM. The 3 controls with available HbA1c measurements had as expected values below 6% (42 mmol/mol). In the total cohort, HbA1c correlated positively with cTnT (rs = 0.284, p = 0.002), NT-proBNP (rs = 0.214, p = 0.023) and GDF-15 (rs = 0.271, p = 0.004). Moreover, women with HbA1c values at or above the recommended 6% (42 mmol/mol) had significantly higher levels of cTnT (p = 0.008), NT-proBNP (p = 0.019) and GDF-15 (p = 0.013) as compared to women below this threshold (Fig. 1).

Boxplots of circulating A cardiac troponin T (cTnT), B N-terminal pro-Brain Natriuretic Peptide (NT-proBNP) and C growth differentiation factor 15 (GDF-15) levels, all in ng/L. Pregnant women with available third trimester HbA1c measurements were categorized into groups based on Norwegian guidelines for glucose control during pregnancy: HbA1c < 42 mmol/mol versus ≥ 42 mmol/mol. Biomarker concentrations are shown in boxplots as 10th percentile (lower whisker), 25th percentile, median (horizontal box line), 75th percentile, 90th percentile (upper whisker), as well as outliers. Groups were compared using the Mann–Whitney U test, *p < 0.050, **p < 0.010
Median sFlt-1 was increased in both DM1 and DM2, but only women with DM1 had decreased median PlGF and a significantly dysregulated sFlt-1/PlGF ratio relative to controls (Table 1). We recently demonstrated a correlation between sFlt-1/PlGF and the CVD markers cTnT and NT-proBNP in women with hypertensive disorders during pregnancy and healthy controls (article in review). Among diabetics (DM1, DM2 and GDM), we again observe a correlation between sFlt-1/PlGF and cTnT (rs = 0.459, p = 0.000) and between sFlt-1/PlGF and NT-proBNP (rs = 0.504, p = 0.000). The association between sFlt-1/PlGF and GDF-15 was not significant (rs = 0.114, p = 0.225).
Discussion
This study shows that DM1 is associated with the highest levels of markers of cardiovascular injury and dysfunction during pregnancy, among diabetic disorders. This is in line with previous observations of increased cardiovascular disease risk and all-cause mortality in people with DM1 as compared to both non-diabetics and people with DM2 [29]. Our results also add to previous reports of elevated cardiovascular biomarkers in women with DM2 and GDM during pregnancy, and underscore the importance of glucose control during pregnancy.
Elevated circulating levels of cardiac troponins in women with DM1, DM2 and GDM, indicating myocardial injury, have been well documented previously [30, 31]. Even prediabetic patients may have higher levels of cTnT in the circulation [32]. Moreover, in both men and women with DM2, cTnT is correlated with advanced glycation end-products (AGE), markers of oxidative stress, and arterial pulse wave reflection [33], and may serve as a biomarker for increased risk of coronary artery disease in patients with diabetes [34, 35]. Our previous report of elevated circulating AGE in pregnancies affected by diabetes [36] combined with our present findings of elevated cTnT in the same groups underscore the presence of cardiovascular dysfunction in diabetes, also during pregnancy. This adds further support to the Obstetrics Guidelines 2020 of the Norwegian Society of Gynecology and Obstetrics (NGF), which recommend supplementing the traditional 4 month postpartum (and later annual) HbA1c testing for DM2 development with a general assessment of cardiovascular health [10]. The NGF guideline suggests similar cardiovascular follow-up by a general practitioner in line with what the Society also suggests after a pregnancy complicated by preeclampsia [37]. The clinical impression is that these recommendations are not followed up, possibly due to limited knowledge of the long-term effects of GDM on other risk factors for cardiovascular disease than glucose control.
Outside of pregnancy, DM1 [38, 39] and DM2 [40] are associated with elevated NT-proBNP levels. Moreover, NT-proBNP may act as an independent risk factor for CVD in patients with DM1 [41] and DM2 [42]. This upregulation may be due to the structural and functional cardiac changes associated with diabetes mellitus mentioned above. Here, we report elevated maternal levels of NT-proBNP in pregnancies with DM1, but no difference in NT-proBNP levels between pregnant women with DM2 and healthy controls. This may be due to the low number (16) of women with DM2 in our study. The regulation of NT-proBNP in GDM is a disputed topic. While Mert and colleagues show clear increases in NT-proBNP levels in GDM [31], two other studies failed to show the same association [43, 44]. Our findings are in line with these latter reports, suggesting that NT-proBNP levels in women with GDM do not reflect the epidemiologically increased risk for future CVD in this group [45].
Unlike cTnT and NT-proBNP, GDF-15 is highly expressed in the placenta [46]. In fact, maternal circulating GDF-15 correlates with placental GDF-15 mRNA levels [25]. In a partly overlapping cohort (84 subjects in common: 27 DM1, 8 DM2, 12 GDM and 37 controls), we have previously shown increased levels of GDF-15 during pregnancy in diabetic pregnancies collectively [25]. In addition, other studies have shown elevated GDF-15 levels in DM2 [47] and GDM separately [48]. GDF-15 is also elevated before onset of DM2, but is not an independent predictor of the disease [49]. Rather, researchers argue that confounding factors underlie elevated GDF-15 levels as well as increased risk of DM2. In the present study, only the group of women with DM1 had significantly higher median level of GDF-15 as compared to the control group. Although the levels of circulating GDF-15 were elevated in women with DM2 and GDM as well, these were not significantly different from controls. This may be partly due to the low number of participants in these groups.
GDF-15 suppresses appetite in animal models [50, 51] and is inversely correlated with BMI in humans outside pregnancy [52]. In pregnancy, a state during which GDF-15 levels increase 200-fold, there is still a negative correlation between GDF-15 and BMI [53]. Here, we report a negative association between GDF-15 prior to delivery and pregestational BMI. In addition, we report no correlation between pregestational obesity and cTnT or NT-proBNP, suggesting that the observed associations between elevated CVD risk markers and diabetes are not confounded by BMI.
Hyperglycemia is known to cause substantial damage to the glycocalyx [54]. Destruction of this protective proteoglycan layer may promote atherosclerosis in larger arteries [55], as well as microvascular disease in arterioles and capillaries [56]. In addition, hyperglycemia reduces NO synthesis [57], reduced endothelial progenitor cell numbers and function [58] and causes hypercoagulability [59]. Accordingly, we here demonstrate an association between the severity of glucose mismanagement during pregnancy and circulating CVD risk markers. This is in line with previous studies also showing a positive correlation between HbA1c levels and circulating troponins, NT-proBNP and GDF-15 [60,61,62]. These observations underscore the importance of glucose control during pregnancy and support strict HbA1c guidelines and follow-up of pregnant women with diabetes. In the present study cohort, the majority of women with DM1 and DM2, as well as a third of women with GDM presented with third trimester HbA1c measurements exceeding the Norwegian guidelines for glucose control during pregnancy for pregestational diabetes mellitus. Norway follows strict guidelines for antenatal follow-up of women with pregestational diabetes [28] and GDM [10]. These guidelines are in line with international guidelines, such as the UK NICE guidelines [9].
In line with our recent report from hypertensive pregnancies (article in review), we observe correlations across all diabetic groups in pregnancy between the sFlt-1/PlGF ratio and cTnT and NT-proBNP, adding support to our concept of crosstalk between placental function and cardiovascular health. As expected, women with DM1 had a median birthweight percentile that was significantly higher than healthy control pregnancies, which is known to associate with larger placentas. The group also displayed a significantly elevated antiangiogenic sFlt-1/PlGF ratio compared to controls. These two findings support our concept of excessive placental growth leading to microvillus overcrowding and placental syncytiotrophoblast stress, which we have postulated underlies the development of placental dysfunction and thus late-onset preeclampsia [63]. The increased risk of preeclampsia development in women with pregestational diabetes is well documented [64], and in accordance with the particularly elevated CVD risk biomarker profile in women with DM1 in the present study.
The cross-sectional nature of our study design and the lack of hard endpoints limit the interpretation of biomarker profiles to assumed CVD risk. Longitudinal studies are required to further elucidate the relationship between diabetes during pregnancy and CVD. Furthermore, many women with GDM do not develop glucose intolerance postpartum [65]. Follow-up characterization and circulating biomarker measurements in women with previous GDM is of great importance, but beyond the scope of the present study. Still, our well-characterized study cohort and the high general health status of the Norwegian population provide unique insights into the association between metabolic dysfunction, placental function and CVD biomarker levels during pregnancy.
Our results indicate the presence of myocardial injury and stress in women with diabetic disorders during pregnancy. Furthermore, we show that women with DM1 are the most affected by the cardiovascular burden of pregnancy. Still, our results suggest that women with GDM should receive targeted cardiovascular follow-up postpartum and receive lifestyle advice, not limited to annual measurement of HbA1c.
Notes
COBAS E and ELECSYS are trademarks of Roche.
References
Vogel B et al (2021) The Lancet women and cardiovascular disease commission: reducing the global burden by 2030. Lancet 397(10292):2385–2438
Gerdts E, Regitz-Zagrosek V (2019) Sex differences in cardiometabolic disorders. Nat Med 25(11):1657–1666
Morrish NJ et al (1991) Incidence of macrovascular disease in diabetes mellitus: the London cohort of the WHO multinational study of vascular disease in diabetics. Diabetologia 34(8):584–589
Kautzky-Willer A, Harreiter J, Pacini G (2016) Sex and gender differences in risk, pathophysiology and complications of type 2 diabetes mellitus. Endocr Rev 37(3):278–316
Peters SA, Huxley RR, Woodward M (2014) Diabetes as a risk factor for stroke in women compared with men: a systematic review and meta-analysis of 64 cohorts, including 775,385 individuals and 12,539 strokes. Lancet 383(9933):1973–1980
Peters SA, Huxley RR, Woodward M (2014) Diabetes as risk factor for incident coronary heart disease in women compared with men: a systematic review and meta-analysis of 64 cohorts including 858,507 individuals and 28,203 coronary events. Diabetologia 57(8):1542–1551
Bellamy L et al (2009) Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet 373(9677):1773–1779
Ratner RE et al (2008) Prevention of diabetes in women with a history of gestational diabetes: effects of metformin and lifestyle interventions. J Clin Endocrinol Metab 93(12):4774–4779
Diabetes in pregnancy: management from preconception to the postnatal period. NICE guideline NG3. 2015, updated 2020; Available from: https://www.nice.org.uk/guidance/qs109/chapter/quality-statement-7-annual-hba1c-testing-after-gestational-diabetes
Friis CMS-R, Holm HO, Toft JH, Roland MCP, Thordarson HB (2020) Svangerskapsdiabetes. In Norsk gynekologisk forening Veileder i fødselshjelp (2020). ePub.
Niakan E et al (1986) Silent myocardial infarction and diabetic cardiovascular autonomic neuropathy. Arch Intern Med 146(11):2229–2230
Shehadeh A, Regan TJ (1995) Cardiac consequences of diabetes mellitus. Clin Cardiol 18(6):301–305
Dortimer AC et al (1978) Diffuse coronary artery disease in diabetic patients: fact or fiction? Circulation 57(1):133–136
Moe K et al (2020) Risk prediction of maternal cardiovascular disease one year after hypertensive pregnancy complications or gestational diabetes mellitus. Eur J Prev Cardiol 27(12):1273–1283
Thygesen K et al (2018) fourth universal definition of myocardial infarction (2018). Circulation 138(20):e618–e651
Herr F, Baal N, Zygmunt M (2009) Studies of placental vasculogenesis: a way to understand pregnancy pathology? Z Geburtshilfe Neonatol 213(3):96–100
Kempf T et al (2007) Prognostic utility of growth differentiation factor-15 in patients with chronic heart failure. J Am Coll Cardiol 50(11):1054–1060
Lew J et al (2017) Sex-based differences in cardiometabolic biomarkers. Circulation 135(6):544–555
Omland T et al (2015) Impact of sex on the prognostic value of high-sensitivity cardiac troponin I in the general population: the HUNT study. Clin Chem 61(4):646–656
Taki M et al (2018) Sex differences in the prognostic power of brain natriuretic peptide and N-terminal pro-brain natriuretic peptide for cardiovascular events—the japan morning surge—home blood pressure study. Circ J 82(8):2096–2102
Ahmad S, Ahmed A (2004) Elevated placental soluble vascular endothelial growth factor receptor-1 inhibits angiogenesis in preeclampsia. Circ Res 95(9):884–891
Redman CWG, Staff AC, Roberts JM (2022) Syncytiotrophoblast stress in preeclampsia: the convergence point for multiple pathways. Am J Obstet Gynecol 226(2S):S907–S927
Sattar N, Greer IA (2002) Pregnancy complications and maternal cardiovascular risk: Opportunities for intervention and screening? BMJ 325(7356):157–160
Jacobsen DP et al (2021) Pregnancy and postpartum levels of circulating maternal sHLA-G in preeclampsia. J Reprod Immunol 143:103249
Sugulle M et al (2009) Circulating and placental growth-differentiation factor 15 in preeclampsia and in pregnancy complicated by diabetes mellitus. Hypertension 54(1):106–112
Alberti KG, Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 15(7):539–553
Johnsen SL et al (2006) Longitudinal reference ranges for estimated fetal weight. Acta Obstet Gynecol Scand 85(3):286–297
Roland MCPHT, Thordarson HB, Strøm-Roum E, Friis CM, Magnussen E (2020) Pregestasjonell diabetes (type1 og type 2). In Norsk gynekologisk forening Veileder i fødselshjelp (2020). ePub.
Lee YB et al (2019) Risk of early mortality and cardiovascular disease in type 1 diabetes: a comparison with type 2 diabetes, a nationwide study. Cardiovasc Diabetol 18(1):157
Everett BM et al (2011) Sensitive cardiac troponin T assay and the risk of incident cardiovascular disease in women with and without diabetes mellitus: the women’s Health Study. Circulation 123(24):2811–2818
Mert MK et al (2016) Troponin T and NT ProBNP levels in gestational, type 1 and type 2 diabetic mothers and macrosomic infants. Pediatr Cardiol 37(1):76–83
Whelton SP et al (2017) High-sensitivity cardiac troponin T (hs-cTnT) as a predictor of incident diabetes in the atherosclerosis risk in communities study. Diabetes Care 40(2):261–269
Hitsumoto T (2015) Factors associated with high-sensitivity cardiac troponin T in patients with type 2 diabetes mellitus. J Nippon Med Sch 82(6):274–280
Hayashi T et al (2017) Cardiac troponin T elevation at dialysis initiation is associated with all-cause and cardiovascular mortality on dialysis in patients without diabetic nephropathy. Clin Exp Nephrol 21(2):333–341
Segre CA et al (2015) Troponin in diabetic patients with and without chronic coronary artery disease. BMC Cardiovasc Disord 15:72
Harsem NK et al (2008) Advanced glycation end products in pregnancies complicated with diabetes mellitus or preeclampsia. Hypertens Pregnancy 27(4):374–386
Staff ACKA, Langesæter E, Michelsen TM et al. (2020) Hypertensive svangerskapskomplikasjoner og eklampsi. In Norsk gynekologisk forening Veileder i fødselshjelp (2020). ePub.
Salem M et al (2009) Early predictors of myocardial disease in children and adolescents with type 1 diabetes mellitus. Pediatr Diabetes 10(8):513–521
McKenna K et al (2005) Elevated plasma concentrations of atrial and brain natriuretic peptide in type 1 diabetic subjects. Ir J Med Sci 174(3):53–57
Magnusson M et al (2004) Elevated plasma levels of Nt-proBNP in patients with type 2 diabetes without overt cardiovascular disease. Diabetes Care 27(8):1929–1935
Tarnow L et al (2005) Plasma N-terminal pro-brain natriuretic peptide as an independent predictor of mortality in diabetic nephropathy. Diabetologia 48(1):149–155
Gaede P et al (2005) Plasma N-terminal pro-brain natriuretic peptide as a major risk marker for cardiovascular disease in patients with type 2 diabetes and microalbuminuria. Diabetologia 48(1):156–163
Sadlecki P, Grabiec M, Walentowicz-Sadlecka M (2016) Prenatal clinical assessment of NT-proBNP as a diagnostic tool for preeclampsia, gestational hypertension and gestational diabetes mellitus. PLoS ONE 11(9):e0162957
Andreas M et al (2011) N-terminal-pro-brain natriuretic peptide is decreased in insulin dependent gestational diabetes mellitus: a prospective cohort trial. Cardiovasc Diabetol 10:28
Staff AC et al (2016) Pregnancy and long-term maternal cardiovascular health: progress through harmonization of research cohorts and biobanks. Hypertension 67(2):251–260
Lawton LN et al (1997) Identification of a novel member of the TGF-beta superfamily highly expressed in human placenta. Gene 203(1):17–26
Dostalova I et al (2009) Increased serum concentrations of macrophage inhibitory cytokine-1 in patients with obesity and type 2 diabetes mellitus: the influence of very low calorie diet. Eur J Endocrinol 161(3):397–404
Yakut K et al (2021) Is GDF-15 level associated with gestational diabetes mellitus and adverse perinatal outcomes? Taiwan J Obstet Gynecol 60(2):221–224
Carstensen M et al (2010) Macrophage inhibitory cytokine-1 is increased in individuals before type 2 diabetes diagnosis but is not an independent predictor of type 2 diabetes: the Whitehall II study. Eur J Endocrinol 162(5):913–917
Mullican SE et al (2017) GFRAL is the receptor for GDF15 and the ligand promotes weight loss in mice and nonhuman primates. Nat Med 23(10):1150–1157
Johnen H et al (2007) Tumor-induced anorexia and weight loss are mediated by the TGF-beta superfamily cytokine MIC-1. Nat Med 13(11):1333–1340
Tsai VW et al (2015) Serum levels of human MIC-1/GDF15 vary in a diurnal pattern, do not display a profile suggestive of a satiety factor and are related to BMI. PLoS ONE 10(7):e0133362
Andersson-Hall U et al (2021) Growth-differentiation-factor 15 levels in obese and healthy pregnancies: relation to insulin resistance and insulin secretory function. Clin Endocrinol (Oxf) 95(1):92–100
Nieuwdorp M et al (2006) Loss of endothelial glycocalyx during acute hyperglycemia coincides with endothelial dysfunction and coagulation activation in vivo. Diabetes 55(2):480–486
Nagy N et al (2010) Inhibition of hyaluronan synthesis accelerates murine atherosclerosis: novel insights into the role of hyaluronan synthesis. Circulation 122(22):2313–2322
Nieuwdorp M et al (2006) Endothelial glycocalyx damage coincides with microalbuminuria in type 1 diabetes. Diabetes 55(4):1127–1132
Noyman I et al (2002) Hyperglycemia reduces nitric oxide synthase and glycogen synthase activity in endothelial cells. Nitric Oxide 7(3):187–193
Ingram DA et al (2008) In vitro hyperglycemia or a diabetic intrauterine environment reduces neonatal endothelial colony-forming cell numbers and function. Diabetes 57(3):724–731
Stegenga ME et al (2008) Hyperglycemia enhances coagulation and reduces neutrophil degranulation, whereas hyperinsulinemia inhibits fibrinolysis during human endotoxemia. Blood 112(1):82–89
Simic S et al (2019) Relationship between hemoglobin A1c and serum troponin in patients with diabetes and cardiovascular events. J Diabetes Metab Disord 18(2):693–704
Siebenhofer A et al (2003) Plasma N-terminal pro-brain natriuretic peptide in type 1 diabetic patients with and without diabetic nephropathy. Diabet Med 20(7):535–539
Tang M et al (2020) Corrigendum to “serum growth differentiation factor 15 is associated with glucose metabolism in the third trimester in Chinese pregnant women” [Diabetes Res. Clin. Pract. 156(2019): 107823]. Diabetes Res Clin Pract 166:108218
Redman CW, Sargent IL, Staff AC (2014) IFPA senior award lecture: making sense of pre-eclampsia–two placental causes of preeclampsia? Placenta 35(Suppl):S20–S25
Weissgerber TL, Mudd LM (2015) Preeclampsia and diabetes. Curr Diab Rep 15(3):9
Noctor E, Dunne FP (2015) Type 2 diabetes after gestational diabetes: The influence of changing diagnostic criteria. World J Diabetes 6(2):234–244
Acknowledgements
We thank Lise Øhra Levy and previous PhD students for patient recruitment and for essential biobanking help at Oslo University Hospital.
Funding
Open access funding provided by University of Oslo (incl Oslo University Hospital). This work was funded by a post doc grant (DPJ) from The South-Eastern Norway Regional Health Authority (The MATCH study: Microchimerism and maternal cardiovascular health, grant number ref 2019012).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Roche Diagnostics donated biomarker reagents in-kind (cTnT, NT-proBNP and GDF-15). Anne Cathrine Staff has received recompensation from Roche Diagnostics for Advisory board service in 2018 regarding preeclampsia screening. Roche Diagnostics had no further involvement in study planning, collection or interpretation of data, writing of the manuscript, or the decision to submit the article for publication.
Ethical Standard Statement
The study was approved by the Regional committee for Medical and Health Research Ethics in South-Eastern Norway, and conducted in accordance with the principles of the Helsinki Declaration.
Informed consent
All women included provided informed written consent.
Additional information
This article belongs to the topical collection Pregnancy and Diabetes, managed by Antonio Secchi and Marina Scavini.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jacobsen, D.P., Røysland, R., Strand, H. et al. Cardiovascular biomarkers in pregnancy with diabetes and associations to glucose control. Acta Diabetol 59, 1229–1236 (2022). https://doi.org/10.1007/s00592-022-01916-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-022-01916-w