
Abstract
Background
Both bone forearm fractures (BBFFs) are a common injury amongst the pediatric population. The main indications of surgical fixation are open, irreducible, or unstable fractures. The two most commonly used surgical techniques are closed or open reduction with intramedullary fixation (IMF) and open reduction with plate fixation (PF). The aim of this systematic review and meta-analysis was to determine which fixation method is superior for BBFFs.
Methods
PubMed, Scopus, Web of Science, and CENTRAL were searched to identify studies comparing IMF and PF. We extracted data on union rates, complications, early hardware removal rates, reoperation rates, and radiographic, clinical, and perioperative outcomes.
Results
Sixteen studies were included in the analysis, with a total of 922 patients (539 IMF and 383 PF). Similar union rates were achieved by both fixation technique. IMF was associated with a higher incidence of symptomatic hardware, and early hardware removal. Better restoration of the radial bow was observed with the PF group, especially in older children and adolescents. The rate of excellent function was comparable between groups, whereas better cosmesis was reported with the IMF group. Despite shorter fluoroscopy time and immobilization time, PF demonstrated longer tourniquet time, operating time, and hospital stay compared to IMF.
Conclusions
We found no significant difference between IMF and PF in terms of union rates and functional outcomes taking in consideration the merits and demerits of each technique. High-quality randomized controlled trials are, therefore, necessary to determine the superiority of one fixation technique over the other.
Level of evidence
III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Both bone forearm fractures (BBFFs) are a common injury amongst the pediatric population accounting for approximately 3–5% of all fractures and 30% of upper extremity fractures [1]. Management of BBFFs is controversial as regards time to operate, acceptable reduction, and age-related remodeling capacity. Most pediatric BBFFs are amenable to nonoperative treatment with closed reduction and cast application. Only 10% of pediatric BBFFS necessitate surgical fixation [2]. The main indications of surgical fixation are open, irreducible or unstable BBFFs. Despite the favourable results of conservative management, surgical fixation of these fractures has become increasingly more common. For instance, Cruz et al. have shown that the percentage of children treated with surgery increased from 59.3% in 2000 to 70.0% in 2012 [3]. The rising trend of operative management may be attributed to technological advancements, socioeconomic changes, liability concerns, and family and surgeon intolerance of residual deformity [4].
The two most commonly used surgical techniques are closed or open reduction with intramedullary fixation (IMF) and open reduction with plate fixation (PF). Several advantages of IMF have been reported, including better cosmesis, minimal soft tissue dissection, decreased operating time, reliable restoration of length and alignment, high union rates, ease of implant removal, and early functional recovery [5,6,7,8]. On the other hand, PF also offers several advantages such as immediate fracture stabilization, anatomic reduction, and restoration of normal radial bow location, and magnitude, considered crucial to forearm rotation [9].
Based on the existing literature [10,11,12], there is no consensus on which fixation modality would provide superior outcomes in terms of safety and efficacy. Therefore, we carried out a systematic review and meta-analysis of studies comparing union rates, complication rates, and radiographic, clinical, and perioperative outcomes of IMF and PF for management of unstable pediatric BBFFs.
Materials and methods
Search protocol and information sources
We conducted a systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [13]. The protocol was registered at PROSPERO (CRD42023494905). PubMed, Scopus, Web of Science and CENTRAL databases were searched from 2000 until 2023 using the following search terms: forearm fracture, both bone, radius and ulna, pediatric, child, adolescent, skeletally immature, intramedullary, plate.
Eligibility criteria, study selection, and data items
Retrieved results were imported into Endnote X9 software (Thomson Reuters, New York, NY, USA), where a check for duplicates was conducted. The titles and abstracts of the remaining articles were then screened with the following exclusion criteria:
-
Articles published in languages other than English.
-
Reviews, guidelines, or classifications.
-
Letters to the editor or case reports, small case series or conference papers
-
In vitro and animal experiment studies
-
Irrelevant studies.
Subsequently, full-text articles of potentially relevant studies were obtained and assessed for eligibility. We included studies that met the following inclusion criteria:
-
Randomized or non-randomized, prospective or retrospective studies comparing IMF and PF for management of BBFF in skeletally immature individuals.
-
The ability to extract data related to the outcomes used for comparison.
-
A minimum sample size of 20 patients.
We extracted the following data from studies that met the inclusion criteria: the name of the first author, year of publication, country of origin, study design, study period, number of participants in each group, participants’ age and gender, fracture characteristics, implants used for surgical fixation, and length of follow-up time.
Primary outcomes:
-
Union
-
Complication, early hardware removal, and reoperation rates.
Secondary outcomes:
-
Radiographic outcomes, including radial bow magnitude, and radial bow location.
-
Clinical outcomes, including function, and cosmesis.
-
Perioperative outcomes, including tourniquet time, fluoroscopy time, operating time, estimated blood loss, length of hospital stay, and immobilization time.
Data collection process, and risk of bias in individual studies
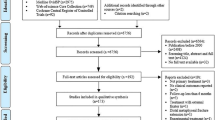
Two independent reviewers performed the review of the list of potential references and the extraction of data, and a third reviewer was consulted, when necessary, to decide any uncertainties regarding eligibility. The flow diagram for the study selection process is shown in Fig. 1.

Flow diagram of the study selection process
The methodological quality of the enrolled studies was evaluated using the Methodological Index for Non-Randomized Studies (MINORS) which consists of eight criteria for non-comparative studies and 12 criteria for comparative studies [14]. Each study scored 0–2 points for each of these items. The methodological quality was determined as follows: a score of 0–12 was considered low quality, 13–18 was considered moderate quality, and 19–24 was considered high quality.
Summary measures, synthesis of results, and risk of bias across studies
We performed all data analyses using Review Manager version 5.4.1. (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). We calculated the odds ratio (OR) with 95% confidence intervals (CIs) for binary outcomes. We calculated the mean difference (MD) with 95% CIs for continuous outcomes. To calculate the overall effect estimate with a 95% CI, we used a fixed-effect model with the method of Mantel–Haenszel when there is no evidence of heterogeneity between studies. Otherwise, a random-effect model with the method of DerSiomonian and Laird was chosen. Heterogeneity between studies was evaluated using the Q statistic and I2 test, which describes the percentage of variability in the effect estimates. Missing values were calculated according to different methods described in the literature [15]. A subgroup analysis was also performed which primarily concerned older children and adolescents. A P value of less than 0.05 was used to declare statistical significance. Publication bias was assessed using funnel plots for outcomes reported by at least 10 studies.
Results
Study selection
The electronic search yielded 922 references from the four databases. After excluding duplicates and title/abstract screening, we had 20 relevant articles for full-text screening. Fourteen fulfilled the inclusion criteria, and six were excluded; two were review articles, one reported inseparable data, and three looked at either IMF, PF, or hybrid fixation exclusively. The manual search of references imported two additional articles.
Study characteristics
Sixteen studies [2, 4, 16,17,18,19,20,21,22,23,24,25,26,27,28,29] were included in the analysis, with a total of 922 patients: 539 patients received IMF, and 383 patients received PF. Baseline characteristics of included studies are demonstrated in Table 1. All included studies were retrospective except for one prospective study by Barua et al. [28] Across studies, the mean age ranged from 9.3 to 14.4 years. Eight studies [19, 20, 22,23,24,25,26, 29] were concerned with older children and adolescents aged 10 years or more. The percentage of male patients ranged from 42 to 100%. The follow-up period ranged from 3.4 to 37 months.
In the IMF group, surgical fixation was performed using TENs in 10 studies [2, 4, 16, 17, 22, 24,25,26,27,28], K-wires in six studies [2, 4, 18, 20, 24, 29], rush pins in four studies [2, 17, 18, 24], and Steinman pins in one study [17]. In the PF group, surgical fixation was performed using small DCP in four studies [2, 16, 17, 22], one-third tubular plates in two studies [18, 22], and LCP and LC-DCP in one study [29]. Three studies did not specify the type of IMF implants [19, 21, 23], whereas PF implants were not specified in 10 studies [4, 19,20,21, 23,24,25,26,27,28]. In the IMF group, fracture reduction via a mini-open approach was reported by 13 studies in 161 (35.5%) patients [2, 4, 16,17,18,19,20,21,22, 24,25,26, 29].
Risk of bias within studies
All included studies reported clearly stated aims, endpoints appropriate to these aims, loss to follow-up less than 5%, adequate control groups, contemporary equivalent groups, and adequate statistical analysis. Ten studies [16,17,18,19,20,21, 23, 25, 26, 29] reported a follow-up period appropriate to the aim of the study, two studies [4, 17] reported consecutive inclusion of patients, and one study [28] reported prospective data collection. None reported unbiased assessment of the study endpoints, or prospective calculation of sample size. As shown in Table 1, the mean MINORS score of the included studies was 16.8 ± 1, ranging from 15 to 19. Accordingly, all included studies had moderate-to-high quality.
Synthesis of results
Union
Union time
Ten studies [4, 17, 18, 20, 22,23,24,25, 27, 28] reported differences in union time with 377 patients in the IMF group, and 276 patients in the PF group (Fig. 2). The majority of studies defined union radiographically by the presence of bridging callus across at least three cortices of bone on standard anteroposterior and lateral radiographs and nontender fracture sites, whereas Ishihara et al. used the modified radiographic union scale in tibial (mRUST) fracture score. The combined MD and 95% CIs was 0.06 (− 0.55 to 0.67). This demonstrates no statistically significant difference between IMF and PF in terms of union time (Z = 0.20, P = 0.84). Subgroup analysis revealed faster union in older children and adolescents using PF compared to IMF. However, the difference was not statistically significant either.

Forest plot of time to union demonstrating no significant difference between IMF and PF
Non-union
Nine studies [2, 16,17,18,19, 21,22,23,24] reported differences in the rate of non-union, defined as inadequate consolidation at 6 months, with 271 patients in the IMF group and 215 patient in the PF groups (Fig. 3). The combined OR and 95% CIs was 1.20 (0.40 to 3.56) with no statistically significant difference between IMF and PF in terms of non-union (Z = 0.33, P = 0.74). By running a subgroup analysis for older children and adolescents, no statistically significant difference was observed between groups either.

Forest plot of non-union demonstrating no significant difference between IMF and PF
Delayed union
Eleven studies [2, 4, 16,17,18,19,20, 22, 25, 27, 28] reported differences in the rate of delayed union, defined as inadequate consolidation at 3 to 4 months, with 344 patients in the IMF group and 246 patient in the PF groups (Fig. 4). The combined OR and 95% CIs was 1.83 (0.80 to 4.16) with no statistically significant difference between IMF and PF in terms of delayed union (Z = 1.44, P = 0.15). By running a subgroup analysis for older children and adolescents, no statistically significant difference was observed between groups either.

Forest plot of delayed union demonstrating no significant difference between IMF and PF
Complications
In all, eleven complications were selected for analysis, including non-union, delayed union, malunion, refracture, infection, compartment syndrome, neuropathy, limited forearm rotation, limited thumb and finger extension, symptomatic hardware, and hardware failure and migration. The pooled results of these complications are summarized in Table 2. No statistically significant difference could be found between groups in terms of complications except for the higher rate of symptomatic hardware associated with IMF.
Early hardware removal
Twelve studies [2, 4, 16,17,18,19, 21,22,23,24,25, 27] reported differences in the early removal rate with 438 patients in the IMF group and 308 patients in the PF group (Fig. 5). The combined OR and 95% CIs was 3.91 (1.84 to 8.33). This demonstrates a significantly higher early removal rates in the IMF group compared to the PF group (Z = 3.54, P < 0.001). Subgroup analysis revealed similar results in older children and adolescents. Causes of early hardware removal are summarized in Table 3.

Forest plot of early hardware removal rate demonstrating a significant difference in favor for PF
Reoperation
Eleven studies [2, 4, 16,17,18,19, 22,23,24,25, 27] reported differences in the reoperation rate with 421 patients in the IMF group and 291 patients in the PF group (Fig. 6). The combined OR and 95% CIs was 0.59 (0.27 to 1.35) with no statistically significant difference between IMF and PF in terms of reoperation rate (Z = 1.38, P = 0.17). By running a subgroup analysis for older children and adolescents, no statistically significant difference was observed between groups either. Causes of reoperation are summarized in Table 4.

Forest plot of reoperation rate demonstrating no significant difference between IMF and PF
Radiographic outcomes
Six studies [19, 21, 22, 24, 25, 28] reported differences in the magnitude and location of radial bow with 187 patients in the IMF group, and 157 patients in the PF group (Fig. 7). The location and maximum radial bow were measured using the method described by Firl and Wunsch both as a percentage of radial length [30]. The combined MD and 95% CIs of radial bow magnitude was − 0.10 (− 0.29 to 0.09) with no statistically significant difference between IMF and PF (Z = 1.04, P = 0.30). Subgroup analysis revealed larger bow magnitude in older children and adolescents using PF compared to IMF. However, the difference was not statistically significant either. For radial bow location, the combined MD and 95% CIs was 3.74 (1.19 to 6.29). This demonstrates a significantly more distal location of radial bow in the IMF group compared to the PF group (Z = 2.87, P = 0.004). Subgroup analysis revealed similar results in older children and adolescents.

a Forest plot of radial bow magnitude demonstrating no significant difference between IMF and PF b forest plot of radial bow location demonstrating a significant difference in favor for PF
Clinical outcomes
Functional outcome
Twelve studies [4, 16,17,18, 20, 21, 23, 25,26,27,28,29] reported differences in functional outcome. Nine studies [17, 18, 20, 23, 25,26,27,28,29] used the Price et al. criteria, Flynn et al. [4] used the Children’s Hospital of Philadelphia (CHOP) Forearm Fracture Fixation Outcome Classification, Teoh et al. [21] used the POSNA Outcome Questionnaire, and Fernandez et al. [16] used a subjective evaluation. However, only 10 studies [4, 16,17,18, 20, 23, 26,27,28,29] were suitable for analysis with 347 patients in the IMF group and 231 patient in the PF groups (Fig. 8). The combined OR and 95% CIs of excellent function was 1.33 (0.88 to 2.03). This demonstrates no statistically significant difference between IMF and PF in terms of functional outcome (Z = 1.35, P = 0.18). By running a subgroup analysis for older children and adolescents, no statistically significant difference was observed between groups either.

Forest plot of excellent function demonstrating no significant difference between IMF and PF
Cosmesis
Three studies [16, 20, 21] reported differences in cosmetic outcome postoperatively. However, only two studies [16, 20] were suitable for analysis with 62 patients in the IMF group and 30 patient in the PF groups (Fig. 9). The combined OR and 95% CIs of excellent cosmesis was 21.58 (6.30 to 73.86). This demonstrates significantly better cosmetic results in the IMF group (Z = 4.89, P < 0.001). Teoh et al. [21] also found that patients who underwent IMF had a better Manchester scar score. Table 5 compares the mean scar length between IMF and PF groups.

Forest plot of excellent cosmesis demonstrating a significant difference in favor for IMF
Perioperative outcomes
Tourniquet, fluoroscopy, and operating time
Two studies [19, 24] reported differences in tourniquet time with 89 patients in the IMF group and 44 patient in the PF groups (Fig. 10). The combined MD and 95% CIs was − 45.79 (− 55.09 to − 36.49). This demonstrates a significantly longer tourniquet time in the PF group (Z = 9.65, P < 0.001).

Forest plot of tourniquet time demonstrating a significant difference in favor for IMF
Three studies [16, 23, 26] reported differences in fluoroscopy time. However, only two studies [23, 26] were suitable for analysis with 82 patients in the IMF group, and 62 patients in the PF group (Fig. 11). The combined MD and 95% CI was 12.75 (2.56 to 22.94). This demonstrates a significantly longer fluoroscopy time in the IMF group (Z = 2.45, P = 0.01).

Forest plot of fluoroscopy time demonstrating a significant difference in favor for PF
Eight studies [16, 19, 20, 23, 26,27,28,29] reported differences in total operating time with 231 patients in the IMF group, and 169 patients in the PF group (Fig. 12). The combined MD and 95% CIs was − 30.96 (− 39.59 to − 22.34). This demonstrates a significantly longer operating time in the PF group (Z = 7.04, P < 0.001).

Forest plot of operating time demonstrating a significant difference in favor for IMF
Estimated blood loss
Three studies [19, 23, 24] reported differences in amount of intraoperative blood loss with 137 patients in the IMF group, and 88 patients in the PF group (Fig. 13). The combined MD and 95% CIs of blood loss was − 28.05 (− 77.90 to 21.81) with no statistically significant difference between groups (Z = 1.10, P = 0.27).

Forest plot of estimated blood loss demonstrating no significant difference between IMF and PF
Length of hospital stay
Four studies [16, 22, 26, 28] reported differences in length of hospitalization with 114 patients in the IMF group, and 103 patients in the PF group (Fig. 14). The combined MD and 95% CIs was − 2.33 (− 3.95 to − 0.71). This demonstrates a significantly longer hospital stay in the PF group (Z = 2.81, P = 0.005).

Forest plot of hospital stay demonstrating a significant difference in favor for IMF
Immobilization time
Seven studies [18, 20,21,22,23, 27, 29] reported differences in immobilization time, ranging from 2 to 6.7 weeks in the IMF group, and from 1.2 to 6.3 weeks in the PF group. However, only three studies [22, 23, 29] were suitable for analysis with 89 patients in the IMF group, and 116 patients in the PF group (Fig. 15). The combined MD and 95% CIs was 2.38 (0.46 to 4.31). This demonstrates a significantly longer immobilization time in the IMF group (Z = 2.42, P = 0.02).

Forest plot of immobilization time demonstrating a significant difference in favor for PF
Risk of bias across studies
Funnels plots were used to check for publication bias for outcomes reported by at least 10 studies. On visual inspection of the funnel plots, there was a possibility of publication bias found in the published studies measuring symptomatic hardware, early hardware removal rate, and union time. No other variables showed obvious asymmetry.
Discussion
BBFFs are amongst the most commonly encountered fractures in the pediatric population [31]. Nevertheless, to date, there is no universal agreement on the optimal treatment strategy, especially in unstable fractures where surgical fixation is mandatory [32]. The purpose of this systematic review and meta-analysis was to determine which fixation technique, IMF, or PF, would provide superior outcomes for the management of unstable BBFFs in children and adolescents.
The most important finding of our study was that IMF and PF had similar union rates, and functional outcomes. Better cosmetic results were reported with IMF. Although both techniques had similar complication and reoperation rates, IMF was associated with a higher incidence of symptomatic hardware, and early hardware removal. Despite shorter fluoroscopy time and immobilization time, PF demonstrated longer tourniquet time, operating time, and hospital stay compared to IMF. The advantages of each surgical technique are summarized in Table 6.
Healing complications in pediatric BBFFs have been shown to be rare by several previous studies [33, 34]. In our study, the mean union time ranged from 6.5 to 10.3 weeks in the IMF group, and from 7.2 to 9.3 weeks in the PF group with no statistically significant difference between fixation techniques [MD (95% CI) = 0.06 (− 0.55, 0.67), P = 0.84]. As age is a major determinant of union rates, a subgroup analysis based on patients’ age was performed [35]. Subgroup analysis of patients aged between 10 and 18 years old showed faster union rates with PF. However, the difference did not reach a statistical significance. On the one hand, both IMF and PF demonstrated low non-union rates of 2.2% and 1.4%, respectively. On the other hand, the overall delayed union rate was 6.1% in the IMF group and 2.4% in the PF group. Although not statistically significant, these results suggest that IMF may result in a higher rate of delayed union. Subgroup analysis of older children and adolescents did not reveal additional data as regards non-union and delayed union rates. A mini-open approach was required in 161 of 453 (35.5%) patients undergoing IMF mostly due to soft tissue interposition or inadequate reduction. Although one might postulate that this may interfere with the healing process, our data showed that opening the fracture site did not alter the outcome.
Regarding complications other than non-union and delayed union, the meta-analysis did not favor either technique in terms of malunion, refracture, infection, compartment syndrome, neuropathy, limited thumb and finger extension, hardware failure and migration or reoperation rate. The IMF group demonstrated higher incidence of symptomatic hardware and early hardware removal compared to the PF group. However, unlike plate removal, minimal activity restrictions are necessary after nail removal because of the absence of stress shielding, cortical continuity, and low risk of refracture [36, 37].
It is worth noting that the incidence of limited forearm rotation (more than 10 degrees) was higher in the PF group (16%) compared to the IMF group (10%), and the difference almost reached statistical significance [OR (95% CI) = 0.55 (0.31, 0.99), P = 0.05]. It is widely known that anatomical restoration of the radial bow in terms of magnitude and location is critical to normal range of forearm rotation. The average values of radial bow magnitude and location in healthy children are approximately 7.21%, and 60.39%, respectively [30]. In our study, the mean radial bow magnitude ranged from 5.1 to 6.8% in the IMF group, and from 5.8 to 6.7% in the PF group. The mean radial bow location ranged from 63 to 69.3% in the IMF group, and from 60.1 to 64.6% in the PF group. Accordingly, better restoration of radial bow location as well as magnitude was observed with PF group, especially in older children and adolescents. This finding can be explained by the fact that as children approach skeletal maturity, remodelling power declines. However, a statistically significant difference was only observed when comparing radial bow location. An association between residual bow deformity and functional deficit in forearm rotation was suggested by Schemitsch and Richards [9]. However, this was not supported by our findings. Despite better anatomical correction of the radial bow location, PF demonstrated greater percentage of patients with limited forearm rotation, as mentioned above. It should be noted that lack of comparison to the contralateral uninjured arm may have skewed the results.
An important factor in the decision-making process is the functional outcome. The majority of included studies defined excellent outcome according to Price et al. criteria as absence of complaint in strenuous activity and loss of forearm rotation less than 15 degrees [38]. Flynn et al. [4] defined excellent outcome according to the CHOP Forearm Fracture Fixation Outcome Classification as full range of forearm movement and absence of postoperative complications. Fernandez et al. [16] defined excellent outcome as patients being very content. Only one study [21] used a validated scoring system, the POSNA questionnaire, for functional evaluation. The overall rate of excellent function was 80% in the IMF group, and 75% in the PF group with no statistically significant difference. Therefore, we may conclude that the difference in forearm rotation between IMF and PF groups, despite being statistically significant, was clinically insignificant. Furthermore, cosmesis is another important factor to many patients. IMF was clearly the most cosmetic choice in the studies that examined this parameter.
Regarding perioperative outcomes, signifcanlty shorter tourniquet time, and operating time were reported with IMF. However, the estimated blood loss during surgery was similar for the two fixation techniques. Fluoroscopy was used intraoperatively for significantly less time in the PF group due to direct visualization of the fracture site. According to Lu et al., intraoperative parameters may also be affected by the type of orthopaedic surgeon where non-pediatric orthopedists needed significantly longer operating time and fluoroscopy time compared to pediatric orthopedists for intramedullary fixation of pediatric forearm fractures [39]. Although the length of hospital stay was longer in the PF group compared to the IMF group, this parameter can be largely affected by conditions unrelated to the forearm fracture especially in polytraumatized patients. Postoperative cast immobilization time was significantly shorter in the PF group versus the IMF group which may have allowed for earlier functional recovery. A significant heterogeneity was found among studies reporting perioperative data. Therefore, these findings should be viewed with caution as perioperative parameters are surgeon dependent and may vary case by case.
Limitations
To our best knowledge, this is the most comprehensive systematic review and meta-analysis of the recent literature to determine to what extent the implant type would impact the radiological and functional outcomes of pediatric BBFFs undergoing surgical fixation. Nonetheless, our study had several inherent limitations. First of all, despite our comprehensive search of the literature, we were only able to include observational studies, mostly retrospective in nature, with no mention of blinding or randomization increasing the likelihood of selection bias. Secondly, most included studies had a relatively small sample size with no prospective power calculation to determine the probability of type II error. Thirdly, different studies had different definitions of an excellent outcome, and only one study used a validated functional scoring system. The lack of standardized definitions of outcome measurements may impact the reported overall estimates. Finally, the specific type of intramedullary devices and plates varied across the studies, and it was not possible to assess if specific types may outweigh the others as the number of studies for each type was too small or the type was not specified. Therefore, high-quality standardized randomized controlled trials with larger sample sizes are necessary to determine the superiority of one fixation technique over the other.
Conclusion
Based on our systematic review and meta-analysis, both IMF and PF are equally effective treatment modalities for BBFFs in skeletally immature patients. While IMF has the advantages of shorter surgical time, and better cosmesis, we may recommend PF for older children and adolescents for earlier union, and better restoration of the radial bow. The merits and demerits of each technique should be discussed thoroughly with a child’s family to reach the best decision possible.
References
Sinikumpu JJ, Lautamo A, Pokka T, Serlo W (2012) The increasing incidence of paediatric diaphyseal both-bone forearm fractures and their internal fixation during the last decade. Injury 43:362–366. https://doi.org/10.1016/j.injury.2011.11.006
Smith VA, Goodman HJ, Strongwater A, Smith B (2005) Treatment of pediatric both-bone forearm fractures: a comparison of operative techniques. J Pediatr Orthop 25:309–313. https://doi.org/10.1097/01.bpo.0000153943.45396.22
Cruz AI Jr, Kleiner JE, DeFroda SF, Gil JA, Daniels AH, Eberson CP (2017) Increasing rates of surgical treatment for paediatric diaphyseal forearm fractures: a National Database Study from 2000 to 2012. J Child Orthop 11:201–209. https://doi.org/10.1302/1863-2548.11.170017
Flynn JM, Jones KJ, Garner MR, Goebel J (2010) Eleven years experience in the operative management of pediatric forearm fractures. J Pediatr Orthop 30:313–319. https://doi.org/10.1097/BPO.0b013e3181d98f2c
Van der Reis WL, Otsuka NY, Moroz P, Mah J (1998) Intramedullary nailing versus plate fixation for unstable forearm fractures in children. J Pediatr Orthop 18:9–13
Qidwai SA (2001) Treatment of diaphyseal forearm fractures in children by intramedullary Kirschner wires. J Trauma 50:303–307. https://doi.org/10.1097/00005373-200102000-00017
Richter D, Ostermann PA, Ekkernkamp A, Muhr G, Hahn MP (1998) Elastic intramedullary nailing: a minimally invasive concept in the treatment of unstable forearm fractures in children. J Pediatr Orthop 18:457–461
Pogorelić Z, Kadić S, Milunović KP, Pintarić I, Jukić M, Furlan D (2017) Flexible intramedullary nailing for treatment of proximal humeral and humeral shaft fractures in children: a retrospective series of 118 cases. Orthop Traumatol Surg Res 103:765–770. https://doi.org/10.1016/j.otsr.2017.02.007
Schemitsch EH, Richards RR (1992) The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 74:1068–1078
Baldwin K, Morrison MJ 3rd, Tomlinson LA, Ramirez R, Flynn JM (2014) Both bone forearm fractures in children and adolescents, which fixation strategy is superior—plates or nails? A systematic review and meta-analysis of observational studies. J Orthop Trauma 28:e8–e14. https://doi.org/10.1097/BOT.0b013e31829203ea
Mmerem K, Beeharry MW (2023) Clinical and radiological outcomes of paediatric forearm fractures of the radius and ulna following fixation by intramedullary nailing or plating: a systematic review. Cureus 15:e43557. https://doi.org/10.7759/cureus.43557
Patel A, Li L, Anand A (2014) Systematic review: functional outcomes and complications of intramedullary nailing versus plate fixation for both-bone diaphyseal forearm fractures in children. Injury 45:1135–1143. https://doi.org/10.1016/j.injury.2014.04.020
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73:712–716. https://doi.org/10.1046/j.1445-2197.2003.02748.x
Weir CJ, Butcher I, Assi V, Lewis SC, Murray GD, Langhorne P et al (2018) Dealing with missing standard deviation and mean values in meta-analysis of continuous outcomes: a systematic review. BMC Med Res Methodol 18:25. https://doi.org/10.1186/s12874-018-0483-0
Fernandez FF, Egenolf M, Carsten C, Holz F, Schneider S, Wentzensen A (2005) Unstable diaphyseal fractures of both bones of the forearm in children: plate fixation versus intramedullary nailing. Injury 36:1210–1216. https://doi.org/10.1016/j.injury.2005.03.004
Carmichael KD, English C (2007) Outcomes assessment of pediatric both-bone forearm fractures treated operatively. Orthopedics 30:379–383. https://doi.org/10.3928/01477447-20070501-08
Ozkaya U, Parmaksizoğlu AS, Kabukçuoğlu Y, Yeniocak S, Sökücü S (2008) Surgical management of unstable both-bone forearm fractures in children. Acta Orthop Traumatol Turc 42:188–192. https://doi.org/10.3944/aott.2008.188
Reinhardt KR, Feldman DS, Green DW, Sala DA, Widmann RF, Scher DM (2008) Comparison of intramedullary nailing to plating for both-bone forearm fractures in older children. J Pediatr Orthop 28:403–409. https://doi.org/10.1097/BPO.0b013e31816d71f2
Kose O, Deniz G, Yanik S, Gungor M, Islam NC (2008) Open intramedullary Kirschner wire versus screw and plate fixation for unstable forearm fractures in children. J Orthop Surg 16:165–169. https://doi.org/10.1177/230949900801600207
Teoh KH, Chee YH, Shortt N, Wilkinson G, Porter DE (2009) An age- and sex-matched comparative study on both-bone diaphyseal paediatric forearm fracture. J Child Orthop 3:367–373. https://doi.org/10.1007/s11832-009-0197-2
Shah AS, Lesniak BP, Wolter TD, Caird MS, Farley FA, Vander Have KL (2010) Stabilization of adolescent both-bone forearm fractures: a comparison of intramedullary nailing versus open reduction and internal fixation. J Orthop Trauma 24:440–447. https://doi.org/10.1097/BOT.0b013e3181ca343b
Zheng W, Tao Z, Chen C, Zhang C, Zhang H, Feng Z et al (2018) Comparison of three surgical fixation methods for dual-bone forearm fractures in older children: a retrospective cohort study. Int J Surg 51:10–16. https://doi.org/10.1016/j.ijsu.2018.01.005
Freese KP, Faulk LW, Palmer C, Baschal RM, Sibbel SE (2018) A comparison of fixation methods in adolescent patients with diaphyseal forearm fractures. Injury 49:2053–2057. https://doi.org/10.1016/j.injury.2018.08.023
Thapa UJ, Wahegaonkar K, Ranjeet N, Sapkota K, Onta PR, Thapa P (2018) Comparative study in the outcome of intramedullary nailing to plating for both-bone forearm fracture in early and mid-adolescent age group. Med J Dr. DY Patil Univ 11:499–505. https://doi.org/10.4103/mjdrdypu.mjdrdypu_84_18
Topak D, Doğar F, Yıldız M, Bilal Ö, Şakı Ö, Ekici E (2020) Comparison of two different surgical treatments of forearm double diaphysis fractures in adolescents. Ann Clin Anal Med 11:457–461
Zeybek H, Akti S (2021) Comparison of three different surgical fixation techniques in pediatric forearm double fractures. Cureus 13:e16931. https://doi.org/10.7759/cureus.16931
Barua DS, Joon A, Vaisakh A, Shirdinayak TS, Hari KNG, Abhijit D (2021) Comparing titanium elastic nailing and plate osteosynthesis in treating both bone diaphyseal fractures of forearm in children. Int J Res Orthopaed 7:1117–1121
Ishihara N, Tokutake K, Takegami Y, Asami Y, Kumagai H, Ota H et al (2023) An age-matched comparative study on intramedullary nailing and plate fixation of both-bone diaphyseal forearm fracture in adolescents. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-023-03679-8
Firl M, Wünsch L (2004) Measurement of bowing of the radius. J Bone Joint Surg Br 86:1047–1049. https://doi.org/10.1302/0301-620x.86b7.14294
Naranje SM, Erali RA, Warner WC Jr, Sawyer JR, Kelly DM (2016) Epidemiology of pediatric fractures presenting to emergency departments in the United States. J Pediatr Orthop 36:e45–e48. https://doi.org/10.1097/bpo.0000000000000595
Caruso G, Caldari E, Sturla FD, Caldaria A, Re DL, Pagetti P et al (2021) Management of pediatric forearm fractures: what is the best therapeutic choice? A narrative review of the literature. Musculoskelet Surg 105:225–234. https://doi.org/10.1007/s12306-020-00684-6
Wyrsch B, Mencio GA, Green NE (1996) Open reduction and internal fixation of pediatric forearm fractures. J Pediatr Orthop 16:644–650. https://doi.org/10.1097/00004694-199609000-00018
Ortega R, Loder RT, Louis DS (1996) Open reduction and internal fixation of forearm fractures in children. J Pediatr Orthop 16:651–654. https://doi.org/10.1097/00004694-199609000-00019
Mills LA, Simpson AH (2013) The risk of non-union per fracture in children. J Child Orthop 7:317–322. https://doi.org/10.1007/s11832-013-0521-8
Beaupre GS, Csongradi JJ (1996) Refracture risk after plate removal in the forearm. J Orthop Trauma 10:87–92. https://doi.org/10.1097/00005131-199602000-00003
Yao CK, Lin KC, Tarng YW, Chang WN, Renn JH (2014) Removal of forearm plate leads to a high risk of refracture: decision regarding implant removal after fixation of the forearm and analysis of risk factors of refracture. Arch Orthop Trauma Surg 134:1691–1697. https://doi.org/10.1007/s00402-014-2079-4
Price CT, Scott DS, Kurzner ME, Flynn JC (1990) Malunited forearm fractures in children. J Pediatr Orthop 10:705–712. https://doi.org/10.1097/01241398-199011000-00001
Lu D, Lin Z, Zhang JD, Chen H, Sun LJ (2017) Treatment of pediatric forearm midshaft fractures: Is there a difference between types of orthopedic surgeon? Orthop Traumatol Surg Res 103:119–122. https://doi.org/10.1016/j.otsr.2016.11.008
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Consent to publish
All participants gave their written informed consent to publish the obtained data of the current study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ahmed, A.M., Said, E., Addosooki, A. et al. Intramedullary versus plate fixation of both bone forearm fractures in skeletally immature patients: a systematic review and meta-analysis. Eur J Orthop Surg Traumatol (2024). https://doi.org/10.1007/s00590-024-03925-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00590-024-03925-7