
Abstract
Purpose
Accurately classifying displaced intraarticular calcaneal fractures (DIACFs) is essential for orthopedic surgeons to choose optimal treatment methods and provide results evaluation and communication. Many authors studying used Sanders classification reported moderate intra- and interobserver reliability. Taking the software opportunity of 3D virtual exarticulation, Goldzak updated French tri-dimensional Utheza classification, providing an alternative framework for classifying DIACFs. The aim of this study was to compare the intra- and interobserver reliability of Sanders versus Goldzak classification systems.
Methods
The CT scans of 30 patients with displaced intraarticular calcaneal fractures, treated in the same trauma center between 2014–2018, were analyzed by 16 medical doctors (specialists and residents in orthopedic surgery, specialists and residents in radiology), and classified according to Sanders and Goldzak classifications. The same images were sent on two separate sessions, in a randomized order. Interobserver reliability and intraobserver reproducibility were assessed using Kappa statistics and Gwet’s AC1 coefficient.
Results
Interobserver reliability using Gwet reported a value of 0.36 for Goldzak classification and 0.30 for Sanders classification (corresponding to “fair assessment” in both cases). In absence of subclasses, “substantial assessment” was reported for Goldzak classification (Gwet of 0.61) and “moderate assessment” for Sanders classification (Gwet of 0.46). Goldzak system had a greater interobserver reliability in the group of radiology residents. Intraobserver reliability coefficient was 0.60 for Goldzak classification and 0.69 for Sanders classification, indicating a substantial agreement for both classifications.
Conclusion
Despite the better view of the fracture lines provided by 3D reconstructions, this study failed to prove the superiority of Goldzak classification compared to Sanders classification for DIACFs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fracture classifications are proposed to clarify fracture patterns and highlight treatment guidelines. CT scans have been in use since the 1990s to aid the analysis of complex fracture pathology. Although Sanders classification is the most used system for classifying displaced intraarticular calcaneal fractures (DIACFs) over the world, the assessment of this classification was fair in all published studies [1,2,3,4,5,6] and its usefulness (especially the subtypes: A, B, and C) has been questioned.
Moreover Sanders type 2 fractures are two-part fractures but the situation of the fundamental fracture line is crossing the articular surface medially, laterally or in its middle. In type 2a and 2c, the fracture line respect the articular surface which remains intact; on the opposite, in type 2b, there is a trans-articular fracture with the risk of residual step off after treatment. Indeed, the 3 subtypes of type 2 fractures are very quite different.
To address these limitations, Goldzak proposed a simplified version of the Utheza classification based on a 3D volume rendering (3D VR) analysis of the fracture [7, 8]. The Utheza classification was published in the early 90’s in the French literature and remained complicated and mainly used in France.
The simplified classification proposed by Goldzak, which is based on two main types depending on the situation of the fundamental fracture line on the 3D reconstructions, aims to be easier to use and of prognostic value.
To evaluate the accuracy of Goldzak classification, we decided to compare it to Sanders classification. We hypothetized that 3D volume rendering and extra-articulation used for Goldzak classification could provide better interobserver and intraobserver reliability than with Sanders classification.
Material and methods
Patients
The CT scans of 30 patients with DIACFs treated in one trauma center (Department of Traumatology and Orthopedic Surgery, Ostrow Wielkopolski, Poland) between 2014 and 2018 were collected and photographed by one of us (MF). The study was approved by our institutional review board. Signed consent was obtained from all participants for all aspects of this study.
Sixteen medical doctors (5 senior orthopedic surgeons, 4 orthopedic surgery residents, 4 trauma radiology specialists, 3 radiology residents) were recruited to analyze and classify the cases using Sanders and Goldzak classification systems. One senior orthopedic surgeon and 2 trauma radiology specialists were based outside of the trauma center. Head of the department who selected the patients and CT scans did not participate in the trials.
Each observer was provided with a package consisting of 2 CT slices (one coronal view including sustentaculum tali, and one axial view including the anterior facet) for classifying according to the Sanders scoring system and 3D VR calcaneal fracture reconstruction pictures (anterior, superior, medial and lateral views) for classifying according to the Goldzak scoring system. All digital images were anonymized and no data allowed to identify both patient and treating surgeon. The images were sent on two separate sessions 8 weeks apart. To minimize the chance of observers memorizing the data from the first session, the order of the cases was randomized for the second session, and the observers were asked not to discuss their cases and classifications. Figures describing Sanders and Goldzak classifications were provided to each participant during each session.
Sanders classification
This classification was the CT scan classification developed by Sanders et al.[9]. The grading of the intraarticular displacement of the posterior facet was based on a coronal CT scan slice and an axial cross section. The injury is classified into 4 major types depending on the number of fracture lines. Each major type is than further categorized into 3 subtypes depending on the situation of the primary fracture line.
Goldzak classification
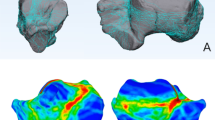
This classification is based on the same principles as the Utheza classification—a 3D reconstruction (Fig. 1). To improve the view of the joint surface, talar and cuboid are digitally removed. Utheza then evaluated the situation of the fundamental fracture line which may be medial with a vertical displacement of the whole posterior facet, lateral with an horizontal displacement of the posterior facet, or crossing the articular surface of the posterior facet creating a double displacement. The Utheza classification also takes into account the end of the fundamental fracture line (similarly as the Essex-Lopresti [10]), describing propagated and included fractures.

Utheza–Goldzak classification
Goldzak simplified and proposed to separate two types of fractures depending on the situation of the primary fracture line, related to the posterior facet. For type 1 fractures, the posterior facet is displaced but intact, in one piece, so that the reduction should be easy and the expected result good. There are 3 subtypes depending of the situation of the primary fracture line (A medial, B lateral, C lateral with an additional fracture line between the posterior facet and the sustentaculum tali). In type 2, the fracture line crosses the posterior facet near the middle, creating a double displacement There are 2 further subtypes, 2A if there is a single fracture line which crosses the posterior facet or 2B if there are 2 fracture lines which cross the articular surface (Fig. 2).

Goldzak classification
Statistical analysis
Intraobserver reproducibility and interobserver reliability were assessed using kappa statistics (SAS software, SAS Institute Inc, Cary, North Carolina, USA). A kappa value of 0.00 represents agreement by chance alone while a kappa value of 1.00 represents perfect agreement. Kappa statistics and Gwet’s AC1 coefficient were interpreted using the guidelines proposed by Landis and Koch [11]: 0.00 < k < 0.020 indicate slight agreement, 0.21 < k < 0.40 fair agreement, 0.41 < k < 0.60 moderate.
For similar studies, Furey used 30 fracture data analyzed by 4 observers while Lauder used 36 fracture data analyzed by 8 observers. As for us, we used 30 fracture data analyzed by 16 observers.
Results
Interrater reliability
The interrater reliability using Gwet coefficient of agreement was 0.36 (95% Cl; 0.228–0.498) for Goldzak classification and 0.30 (95% Cl; 0.200–0.393, p < 0.001) for Sanders classification (Table 1).
According to Landis and Koch, these results indicate fair assessment for both classifications [11].
When the subclasses were not used, a substantial assessment was found for Goldzak classification with a Gwet coefficient of 0.61, and a moderate assessment for Sanders classification with a Gwet coefficient of 0.46. When the ordinal range was taken into account, a substantial assessment was found for both classifications with, respectively, 0,61 and 0,68 for Gwet analysis.
For Goldzak classification, the Gwet coefficient was 0.29 for orthopedic residents, 0.37 for orthopedic surgeons, 0.37 for radiologists and 0.68 for radiology residents. For Sanders classification, the scores were 0.28 for orthopedic residents, 0.30 for orthopedic surgeons, 0.44 for radiologists and 0.26 for radiology residents (Table 2).
Intrarater reliability
Overall, the intrarater reliability kappa coefficient was 0.60 for Goldzak classification and 0.69 for Sanders classification, which indicates that both classification systems are characterized by substantial intraobserver agreement (Table 3).
Discussion
In the last five decades, 49 classification systems of calcaneal fractures have been proposed, and 19 of them are considered as current [12]. Such multitude of classifications can make the communication between radiologists and/or surgeons (or between different trauma departments) difficult.
Although the most commonly used system is the one proposed by Sanders[9], others are also frequently used worldwide [1]: Orthopaedic Trauma Association (OTA) classification [13], Essex-Lopresti [10], Crosby [14], Zwipp[15] and Regazzoni [16]. All current classification systems of calcaneal fracture are based on CT scans. However, none of these systems, including the Sanders classification, has reached the general acceptance as a result of low interrater [17]. For this reason searching a classification which would be not only descriptive but useful for surgical decisions, communication and predictive for outcome is always of value.
In this study, we compared the interobserver and intraobserver reliability of two classifications systems for intraarticular calcaneal fractures: the one of Sanders, based on 2D scans, and the Goldzak classification, based on 3D CT VR and virtual exarticulation. Both classifications considered the severity of the fracture: for Sanders, the main point is the number of fracture lines and thus the number of separated parts; for Goldzak, the main point is the preservation (or lack thereof) of the articular surface of the posterior facet. In both systems, type 1 is less severe, while type 2 for Goldzak classification and types 2, 3, 4 for Sanders classification are more severe.
In this study, interobserver rating showed fair agreement for both classifications. When the subclasses were not used (i.e., the letters were omitted), the Goldzak system showcased a substantial agreement with a 0.61 coefficient versus a moderate assessment only for Sanders classification with a 0.46 coefficient. It should be taken into consideration that the Sanders classification is well known and widely used in daily practice (especially by specialists in radiology and orthopedics), in contrast to the Goldzak classification, which was often first used by the observers during the presented study.
Among the group of radiology residents, who most likely classified less calcaneal fracture than more experienced radiology specialists, Goldzak interobserver reliability reached substantial agreement (coefficient of 0.68), while the Sanders system was characterized by only fair compatibility (coefficient of 0.26). This result suggests that the Goldzak system is more intuitive and easier to learn than Sanders. Repetitive training of observers on a classification system may further improve its reliability [1], which can result in a greater interobserver rating for Goldzak classification.
The interobserver reliability of Sanders classification in the available literature ranges from k = 0.22 [18] to k = 0.55 [5], which is classified as fair or moderate compatibility [1,2,3, 5, 6, 18, 19]. That observation is in line with our results, where the kappa value for those system was 0.30 (fair agreement). Brunner et al. noted, that the more complex and precisely the classification system is (i.a. Sanders), the more it may affect its reproducibility [1]. Hence, its usefulness (especially using the subtypes, A, B, and C) has come into question. Moreover, when using the Sanders system without subclasses, the interobserver agreement is greater, but still has remained stable on kappa value < 0.6 [5, 6]. Similar correlation was observed in the presented study. In the Sanders classification, the historic single CT cut, as originally described, represents the anterior portion of the posterior facet at the level of the sustentaculum tali. It is clear that it does not give a general overview at a glance of the anatomy [20] and a fracture may be identified as a Sanders type II anteriorly, as well as a Sanders type III posteriorly, depending on the chosen slice.
3D reconstruction of CT scans was proposed to improve accuracy and precision of the evaluation of fracture pathology [17]. Many authors have postulated that complex intraarticular fractures would be best classified with the use of advanced modalities 3D VR [4]. Obtained results displayed greater interobserver reliability, especially among inexperienced radiologists, when interpreting the scans using 3D CTs. Similar results were presented by Misselyn et al. Within the group of less experienced observers, they noted that the agreement with the reference standard (in Sanders system) was significantly higher when using 3D technique in comparison to 2D images [20]. Brunner et al. also found that 3D reconstruction was beneficial for less experienced doctors [1]. As there is no extra cost or radiation exposure, 3D CTs can be proposed as a valuable method with preoperative teaching and planning particularly for less experienced observers [21].
On the other hand, the interobserver reliability for both studied classification is fair. It seems that the analysis of the fractured calcaneus on 3D VR scans (i.a. Goldzak) is not always superior to 2D slices (i.a. Sanders), notably in the group of experienced radiologists, which was also highlighted in the study by Veltman et al.[18].
In the discussed study, radiology specialists gained a comparable interobserver reliability rate in the Goldzak system, and significantly higher rate in Sanders in comparison to orthopedic surgeons’ results. On the contrary, Schepers et al. observed a significantly greater coefficient value among surgeons in comparison to radiologists while classifying the calcaneal fractures according to Sanders (0.52 vs. 0.30) [12]. Thus, the modified Utheza system seems to be a more universal device for communication between radiologists and surgeons. More experienced observers achieved better single kappa values compared with less experienced observers (residents), which was reported previously [2].
The intraobserver reproducibility for Goldzak system (0.61), as well as Sanders system (0.70), was identified as substantial agreement. Similar results were presented by Lauder et al., where the Sanders system with subclasses reached moderate (0.57) agreement (substantial agreement in the 0.77 range when excluding subclasses) [5]. In the study by Veltman et al., the intraobserver rate for the Sanders classification was lower (0.46) than observed in the aforementioned results [18].
Our findings regarding 3D images are unexpected, as 3D images provide more details than CT scans and hence should make fracture classification easier. These results may be due to more common use of the Sanders classification and consequently, greater familiarity with this system. 3D CT scanning and VR with virtual exarticulation is also relatively new option, which very likely has a lot of benefits not revealed in available trials and may give useful information not captured by current classification systems [1]. Goldzak 3D VR reconstruction may enable better assessment of fragment size, displacement pattern, reliability to repair and exact fracture geometry compared with 2D; however, these issues were not the focus of this paper and require further investigation.
Conclusions
The interobserver reliability was fair for both classification systems, while the intraobserver reproducibility was identified as substantial. Despite the better view of the fracture lines provided by 3D reconstructions, the study failed to prove the superiority of Goldzak classification compared to Sanders classification.
References
Brunner A, Heeren N, Albrecht F et al (2012) Effect of three-dimensional computed tomography reconstructions on reliability. Foot Ankle Int 33:727–733. https://doi.org/10.3113/FAI.2012.0727
Howells NR, Hughes AW, Jackson M et al (2014) Interobserver and intraobserver reliability assessment of calcaneal fracture classification systems. J Foot Ankle Surg 53:47–51. https://doi.org/10.1053/j.jfas.2013.06.004
Sayed-Noor AS, Ågren P-H, Wretenberg P (2011) Interobserver reliability and intraobserver reproducibility of three radiological classification systems for intra-articular calcaneal fractures. Foot Ankle Int 32:861–866. https://doi.org/10.3113/FAI.2011.0861
Humphrey CA, Dirschl DR, Ellis TJ (2005) Interobserver reliability of a CT-based fracture classification system. J Orthop Trauma 19:616–622. https://doi.org/10.1097/01.bot.0000177107.30837.61
Lauder AJ, Inda DJ, Bott AM et al (2006) Interobserver and intraobserver reliability of two classification systems for intra-articular calcaneal fractures. Foot Ankle Int 27:251–255. https://doi.org/10.1177/107110070602700405
Bhattacharya R, Vassan UT, Finn P, Port A (2005) Sanders classification of fractures of the os calcis. An analysis of inter- and intra-observer variability. J Bone Joint Surg Br 87:205–208. https://doi.org/10.1302/0301-620x.87b2.15260
Utheza G, Goldzak M, Chaminade B et al (1998) 3-dimensional imaging of thalamic fractures of the calcaneum. Validation of classifying fractures into 3 forms. Rev Chir Orthop Reparatrice Appar Mot 84:440–450
Utheza G, Flurin PH, Colombier JA et al (1993) Intraarticular fractures of the calcaneus: pathological description. Contribution of x-ray computed tomography. Rev Chir Orthop Reparatrice Appar Mot 79:49–57
Sanders R, Fortin P, DiPasquale T, Walling A (1993) Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 290:87–95
Essex-Lopresti P (1952) The mechanism, reduction technique, and results in fractures of the os calcis. Br J Surg 39:395–419. https://doi.org/10.1002/bjs.18003915704
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Schepers T, van Lieshout EMM, Ginai AZ et al (2009) Calcaneal fracture classification: a comparative study. J Foot Ankle Surg 48:156–162. https://doi.org/10.1053/j.jfas.2008.11.006
Marsh JL, Slongo TF, Agel J et al (2007) Fracture and dislocation classification compendium-2007: orthopaedic trauma association classification, database and outcomes committee. J Orthop Trauma 21:S1-133. https://doi.org/10.1097/00005131-200711101-00001
Crosby LA, Fitzgibbons T (1990) Computerized tomography scanning of acute intra-articular fractures of the calcaneus. A new classification system. J Bone Joint Surg Am 72:852–859
Zwipp H, Tscherne H, Thermann H, Weber T (1993) Osteosynthesis of displaced intraarticular fractures of the calcaneus. Results in 123 cases. Clin Orthop Relat Res 290:76–86
Regazzoni P Behandlung von Kalkaneusfrakturen. Basler Beiträge Chir
Roll C, Schirmbeck J, Müller F et al (2016) Value of 3D reconstructions of CT scans for calcaneal fracture assessment. Foot Ankle Int 37:1211–1217. https://doi.org/10.1177/1071100716660824
Veltman ES, van den Bekerom MPJ, Doornberg JN et al (2014) Three-dimensional computed tomography is not indicated for the classification and characterization of calcaneal fractures. Injury 45:1117–1120. https://doi.org/10.1016/j.injury.2014.01.022
Piovesana LG, Lopes HC, Pacca DM et al (2016) Assessment of reproducibility of Sanders classification for calcaneal fractures. Acta Ortopédica Brasileira 24:90–93
Misselyn D, Nijs S, Fieuws S et al (2018) Improved interobserver reliability of the sanders classification in calcaneal fractures using segmented three-dimensional prints. J Foot Ankle Surg 57:440–444. https://doi.org/10.1053/j.jfas.2017.10.014
Halai M, Hester T, Buckley RE (2020) Does 3D CT reconstruction help the surgeon to preoperatively assess calcaneal fractures? Foot 43:101659. https://doi.org/10.1016/j.foot.2019.101659
Acknowledgements
The authors would like to deeply thank all the observers that participated to that study: the radiologists (Banasiak Magdalena, Bekalarek Kamil, Drzewiecka Dominika, Posadzy Magdalena, Romanowski Michal, Skowronska Agnieszka, Stawik Aleksandra) and orthopedic surgeons (Becki Marcin, Mikolajczyk Adrian, Palczewski Karol, Schenck Benoit, Szymczak Tomasz, Smiechura Lukasz, Smilowicz Rafal) and Maria Teresa Falis who collected the results. The authors would also like to deeply thank Chantal Simon, Ph.D., M.D. who assumed the statistical part of that study
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Falis, M., Bargiel, A., Pyszel, K. et al. Classification of intraarticular calcaneal fractures: comparison of two classification systems. Eur J Orthop Surg Traumatol 34, 1503–1508 (2024). https://doi.org/10.1007/s00590-023-03800-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-023-03800-x