
Abstract
Purpose
The objective of this study is to characterize the occurrence of odontoid fractures within a Swedish population.
Methods
Prospective data of adults diagnosed with an odontoid fracture between 2015 and 2021 were retrieved from the Swedish Fracture Register (SFR). Epidemiologic data including age, sex, injury mechanism, injury type, fracture type (Anderson and D’Alonzo classification), neurological status and treatment type were requested from the SFR. Data pertinent to osteoporosis was retrieved from the Swedish National Patient Register.
Results
A total of 1,154 odontoid fractures were identified, of which 30 were type I fractures, 583 type II fractures, and 541 type III fractures. The mean (Standard Deviation [SD]) age was 77.2 (13.8) years. The prevalence of osteoporosis and neurological deficits did not differ between the fracture types. The majority of patients were treated non-surgically (81%). Male sex and patient age 18–30 years were commonly associated with a high-injury mechanism, especially motor vehicle accidents. In the type II fracture group, significantly more patients had fallen from standing height or less than in the type III group (66% vs. 58%, p = 0.01) while in contrast, motor vehicle accidents were more common in the type III fracture group (12% vs. type II: 8%, p = 0.04).
Conclusion
Based on the SFR, the typical odontoid fracture patient is older and suffers a type II fracture. Most injuries were caused by low-energy trauma although in younger patients and males, they were associated with motor vehicle accidents. Across the patient population, odontoid fractures were usually treated non-surgically.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Odontoid fractures are the most common cervical spine fractures in adults aged 65 years or above and show an increasing incidence with age [1, 2]. These fractures constitute 9–15% of all adult cervical spine fractures [3]. In recent years, several large-scale epidemiologic studies from countries such as the US and Norway have characterized the demographic patterns associated with odontoid fractures [2, 4, 5]. Despite this, nationwide studies containing data from fracture-specific registers are currently lacking. In light of this, the increasing incidence of odontoid fractures paralleling with an aging population poses a substantial economic and social burden on health care systems globally. Consequently, updated epidemiological investigations are necessary to improve the understanding of odontoid fracture epidemiology and management. The aim of this study was to perform an epidemiological survey of patients with odontoid fractures in terms of demographic, injury-related and surgical characteristics using the Swedish Fracture Register (SFR).
Methods
This study was reported according to STROBE guidelines for observational studies.
The Swedish Fracture Register (SFR)
This study is based on the SFR, a nationwide quality register collecting data pertinent to all fracture types of the extremities, pelvis and spine in Sweden. The SFR was established in 2011 and comprises data from over 900,000 patients [6]. Spinal fractures have been registered since 2015. From the inception of the SFR, coverage has grown to include all the 54 orthopeadic departments in Sweden, demonstrating nationwide coverage in 2020 [7]. Inclusion in the register is limited to fractures sustained within Sweden in patients with valid Swedish social security numbers and a fracture diagnosis confirmed with radiographic imaging. The physician records the date and mechanism of injury and classifies the fracture based on clinical and radiographic characteristics. Fractures in the SFR may be registered by the evaluating physician in the Orthopeadic emergency department or by the treating surgeon if the fracture is treated surgically.
Study population and eligibility criteria
Prospective register data was collected from the SFR between February 2015 and September 2021. Patients ≥ 18 years with a fracture of the odontoid process (Anderson and D’Alonzo classification [8]; Fig. 1) were eligible for inclusion. Demographics including age and sex as well as injury and treatment related data encompassing injury date, injury mechanism, injury type, fracture type (type I, II and III), neurological deficits, and treatment type were queried. Additionally, the diagnosis of osteoporosis (M80, M81, M82) was retrieved from the Swedish National Patient Register.

Reprint of this figure was permitted by the Swedish Fracture Register. Please note that ‘’traumatisk spondylolistes’’ corresponding to traumatic spondylolisthesis is not included in the analysis of the current manuscript
Classification of C2 fractures in the Swedish Fracture Register according to the web-based protocol at https://sfr.registercentrum.se/.
Statistical analysis
Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Continuous data are presented as mean (standard deviation [SD]) and median (min-max)). For categorical variables, count (n) and proportion (%) are reported. Differences between groups were assessed using one-way analysis of variance (ANOVA) for continuous variables and using chi-square test for non-ordered categorical variables. For pairwise comparisons between groups, the Fisher’s exact test (2-sided) was calculated for dichotomous variables and ANOVA for continuous variables. A two-tailed p-value < 0.05 was determined statistically significant.
Results
Demographic characteristics
Totally, 1,154 odontoid fractures were identified in the SFR (Table 1). The cohort comprised 30 patients with type I, 583 patients with type II and 541 patients with a type III fracture. Figure 2 displays the seasonal variation in injury incidence. The mean [SD] age was 77.2 (13.8) years, with type II fractures being oldest at 78.2 (13.1) years (p < 0.001, Fig. 3). Sex distribution was similar in the total study group, but significant differences were found between type II and type III fractures as more males suffered a type II fracture compared to type III fractures (56% vs. 45% p < 0.001, Table 1).

Seasonal variations of odontoid fractures. Vertical lines denote the confidence intervals

Age at injury by sex
The presence of neurological deficits as well as a diagnosis of osteoporosis did not differ between the three fracture types. Moreover, most patients underwent non-surgical treatment (81%). Surgical treatment was more prevalent with type II fractures (22%) compared with type III fractures (17%, p = 0.02).
Degree of trauma and injury mechanism
Only 135 (14%) patients were involved in a high-energy trauma, while 800 patients (86%) had a low impact trauma in the injury mechanism (Table 2). Significantly more patients in the type II fracture group (89%) were recorded to have a low-energy trauma compared with type III fractures (82%, p < 0.01). There was no difference between the prevalence of the three fracture types when all injury mechanisms were combined (fall from standing height or less, fall from height, motor vehicle accident, unspecified fall, or other causes). However, significantly more patients in the type II fracture group (66%) sustained a fall from standing height or less compared to patients with type III fractures (58%, p = 0.01). Conversely, a greater proportion of patients with type III fractures (12%) were involved in motor vehicle accidents than type II fractures (8.1%, p = 0.04).
Injury characteristics by age
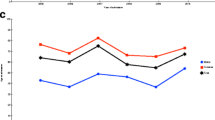
Most of the patients aged 18–30 years (75%) were involved in a high-energy trauma in comparison to the age groups 31–65 years (38%, p < 0.01) and > 65 years (9.6%, p < 0.001, Fig. 4, Supplementary Tables 1a-c). Additionally, significantly more patients aged > 65 years (67%) had fallen from standing height or less compared to those aged 18–30 years (23%, p < 0.001) and 31–65 years (37%, p < 0.001). Patients aged 31–65 years (20%) were more likely to fall from a height compared with the > 65 years group (13%, p = 0.04). In contrast, a greater proportion of patients within the age range 18–30 years (55%) were associated with motor vehicle accidents than those aged 31–65 years (30%, p < 0.05) and > 65 years (6.1%, p < 0.001). Similar findings were seen with the analysis of type II and type III fractures with regards to trauma type and injury mechanisms.

Degree of trauma by age groups 18–30 years; 31–65 years and 66 years or older
Injury patterns in males and females
A greater proportion of females (89%) sustained fractures in low-energy traumas compared to males (83%, p = 0.01, Supplementary Tables 2a-c). Subgroup comparisons within each type of injury mechanism did not show any sex differences, except for motor vehicle accidents being more prevalent in males (12% vs. females 8.1%, p = 0.04). In type II fractures, no differences were found between sexes in terms of the degree of trauma. Furthermore, an equal number of males and females were diagnosed with type II fractures in response to any of the registered injury mechanisms. Conversely, in type III fractures, males (23%) were more commonly recorded to be involved in a high-energy trauma than females (14%, p = 0.03). Consistent with the total study population, a greater proportion of males with type III fractures (16%) were involved in motor vehicle accidents than females (9.3%, p = 0.04). No other injury mechanism differed between sexes in the type III fracture group.
Discussion
The main findings of this study were that odontoid fractures usually occurred in older individuals, and type II fractures was the most frequent fracture type. Only 14% of the odontoid fractures were due to high-energy trauma. In younger individuals, motor vehicle accidents were usually reported as the injury mechanism. Conversely, in older patients, low-energy traumas were more frequent, and the fractures were predominantly caused by low-level falls. Males were commonly injured in high energy-related accidents. Lastly, non-surgical treatment was the preferred choice of management in 81% of cases.
Data from the SFR demonstrate that odontoid fractures were frequent in elders, with a mean age of 77.2 years and is consistent with previous studies [5, 9]. However, contrary to earlier reports, the present study found a clear unimodal age distribution, with a peak in the seventh to ninth decade of life. In a recent study from Illinois, USA, bimodal age distributions with peaks at 22 and 78 years of age were reported [10]. When comparing traffic accidents between Sweden and Illinois, USA, there were 4.6 times more fatal motor vehicle accidents per capita in Illinois in 2021 [11, 12]. In light of these findings, the peak in younger individuals may be the result of serious traffic accidents which was rather rare in the current study.
Approximately half of the patients with an odontoid fracture were male individuals, which is comparable with earlier studies [2, 4, 9, 13]. Similar to a previous cohort, the included male patients tended to be younger, while elders more commonly tended to be females [5]. Apart from being younger, males were less likely to be injured in low-energy traumas. While the exact mechanisms are not understood, young males are more likely to be risk-takers and show different travelling habits than females. In comparison, elderly females sustain fractures more easily, perhaps because of menopause and subsequently, an osteoporotic odontoid process [14]. Only 10% of the patients in this study had an osteoporosis diagnosis at the time of injury. Previous work has shown rates of osteoporosis in populations with odontoid fractures ranging between 58 and 77% which is considerably higher than this study [15, 16]. Likely explanations to this discrepancy could be that patients in this study possibly demonstrated signs of osteoporosis without having the diagnosis recorded (ICD codes), or that it was undiagnosed.
A large majority of patients had an intact neurological status (94%) whereas only 2.1% had some type of spinal cord injury. This is somewhat lower than previous reports with spinal cord injuries affecting 3–10% of patients [5, 17,18,19,20]. The relatively low rate in this study could be explained by several morphological attributes. For instance, the relatively large cross-sectional diameter of the spinal canal at the level of the odontoid process compared to the diameter of the spinal cord may result in fewer spinal cord injuries compared to other cervical spine fractures. Moreover, most odontoid fractures were associated with low-energy trauma and therefore did not contribute to large displacement causing neurological injuries.
The occurrence of odontoid fractures varied during the seasons with peaks in May and August. There is, to our knowledge, no previous research on the seasonal variation of odontoid fractures. However, other studies from the SFR have investigated seasonal variation of various fracture types. Talus fractures were usually sustained in warmer months (May through October) [21] while patella and ankle fractures in the colder months (October through March) [22, 23]. Speculatively, individuals are more physically active and spend more time outdoors during the summer months, therefore falling more often. Moreover, higher temperatures are associated with hypovolemia, syncope and other cardiac events in the elderly causing falls, and ultimately, odontoid fractures. In contrast, in the winter months, the streets are often slippery in Sweden which could be the cause of the increased number of patella and ankle fractures. One could only speculate as to why this increase was not seen in odontoid fractures. Perhaps those with odontoid fractures are generally older with more co-morbidities than those sustaining patella or ankle fractures. This could result in patients remaining inside when they know that the ground is unsafe to walk on.
Most of the included patients were treated non-surgically (81%) which is consistent with other publications [20, 24]. However, a previous study based on a Swedish population reported that 53% with a type II odontoid fracture underwent surgery with an annual increase between 2002 and 2014 [25]. This study included urban hospitals whereas the SFR receives data from hospitals all over Sweden. Moreover, the SFR has only collected data on spine fractures since 2015 which could provide another explanation to the different managements of type II fractures. Type II fractures are generally prone to pseudoarthrosis and non-union, and although guidelines on the management of odontoid fractures are absent, the risk of impaired fracture healing in type II fractures is an indication for surgical stabilization. This is consistent with our study since significantly more patients with type II fractures underwent surgery than the other fracture types. The overall aim of surgical treatment is to preserve the neurological function, relieve pain and establish a stable fusion. As only 3.5% of the included patients suffered neurological deficits, this could partly explain why most of the patients received non-surgical treatment. Other possible reasons may include high age and major co-morbidities.
Lastly, in this study, 87% of the fractures were caused by falls. For type II fractures, the corresponding number was 90% and for type III fractures 85%, respectively. This is similar to previous publications from Scandinavia [5, 17]. Consistent with earlier findings, older patients were more often injured after falls from a standing height or less, while younger patients were more often injured in a motor vehicle accident [10, 13]. Furthermore, older patients were more likely to sustain an odontoid fracture by a low-energy trauma than younger patients which could be explained by altered body composition, neurological dysfunction and the increasing number of co-morbidities that parallel with aging. For instance, physical inactivity, impaired balance, and neurological disabilities may result in unintended falls. In addition, polypharmacy is common in elders, further increasing the risk of falls [5]. Others have proposed that increasing age is associated with a stiffer cervical spine, and a reduced bone density, which can explain why elderly need less energy for a fracture to develop [25].
Strengths and limitations
The SFR contains data from patients within various geographic locations, representing a heterogenous population which enables a broad generalizability of the results from this study. Additionally, compared to traditional epidemiologic studies based on a sample of the population, the SFR is a population-based register minimizing the risk of selection bias. Moreover, the SFR contains one of the largest datasets on odontoid fractures, enabling the conduction of reliable subgroup analyses. The SFR also contains detailed records pertinent to injury patterns and the data are prospectively collected, which mitigates the risk of recall bias. On the other hand, the completeness of odontoid fracture coverage in the SFR is unknown. Fractures are registered by physicians with various levels of expertise, which may introduce bias due to incorrectly diagnosed or classified fractures. While the reliability of the Anderson and D’Alonzo classification [8] in the SFR has not been evaluated, classification of other fractures including thoracolumbar [26], ankle [27], and humerus [28] fractures have been shown to be highly reliable.
Conclusion
Based on the SFR, the typical patient with an odontoid fracture was older and suffered a type II fracture. Moreover, odontoid fractures typically occurred as a result of a low-energy trauma with a relatively low risk of neurological deficits. However, younger patients and males were more commonly involved in motor vehicle accidents. Most patients with an odontoid fracture were treated non-surgically although surgical treatment was more frequent in type II fractures.
Data availability
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
References
Ryan MD, Henderson JJ (1992) The epidemiology of fractures and fracture-dislocations of the cervical spine. Injury 23:38–40. https://doi.org/10.1016/0020-1383(92)90123-a
Salottolo K, Betancourt A, Banton KL, Acuna D, Panchal R, Bar-Or D, Palacio CH (2023) Epidemiology of C2 fractures and determinants of surgical management: analysis of a national registry. Trauma Surg Acute Care Open 8:e001094. https://doi.org/10.1136/tsaco-2023-001094
Butler JS, Dolan RT, Burbridge M, Hurson CJ, O’Byrne JM, McCormack D, Synnott K, Poynton AR (2010) The long-term functional outcome of type II odontoid fractures managed non-operatively. Eur Spine J 19:1635–1642. https://doi.org/10.1007/s00586-010-1391-0
Alluri R, Bouz G, Solaru S, Kang H, Wang J, Hah RJ (2021) A nationwide analysis of geriatric odontoid fracture incidence, complications, mortality, and cost. Spine (Phila Pa 1976) 46:131–137. https://doi.org/10.1097/brs.0000000000003734
Rizvi SAM, Helseth E, Rønning P, Mirzamohammadi J, Harr ME, Brommeland T, Aarhus M, Høstmælingen CT, Ølstørn H, Rydning PNF, Mejlænder-Evjensvold M, Utheim NC, Linnerud H (2020) Odontoid fractures: impact of age and comorbidities on surgical decision making. BMC Surg 20:236. https://doi.org/10.1186/s12893-020-00893-7
Svenska Frakturregistret https://sfr.registercentrum.se/
Möller M, Wolf O, Bergdahl C, Mukka S, Rydberg EM, Hailer NP, Ekelund J, Wennergren D (2022) The Swedish Fracture Register - ten years of experience and 600,000 fractures collected in a National Quality Register. BMC Musculoskelet Disord 23:141. https://doi.org/10.1186/s12891-022-05062-w
Anderson LD, D’Alonzo RT (1974) Fractures of the odontoid process of the axis. J Bone Joint Surg Am 56:1663–1674
Honda A, Michihata N, Iizuka Y, Mieda T, Takasawa E, Ishiwata S, Matsui H, Fushimi K, Yasunaga H, Chikuda H (2021) Clinical features and early post-operative complications of isolated C2 odontoid fractures: a retrospective analysis using a national inpatient database in Japan. Eur Spine J 30:3631–3638. https://doi.org/10.1007/s00586-021-06862-9
Cloney MB, Thirunavu V, Roumeliotis A, Texakalidis P, Swong K, El Tecle N, Dahdaleh NS (2023) Traumatic dens fracture patients comprise distinct subpopulations distinguished by differences in Age, Sex, Injury mechanism and severity, and Outcome. World Neurosurg 178:e128–e134. https://doi.org/10.1016/j.wneu.2023.07.007
Fredriksson RHP, Larsson P, Lindholm M, Rizzi M, Sternlund S (2022) Analys Av trafiksäkerhetsutvecklingen 2021: Målstyrning av trafiksäkerhetsarbetet mot etappmålen 2030. In: Trafikverkets publikationer. Borlänge
Watters C (2022) 2022 Illinois Highway Safety Plan Annual Report. In. Illinois Department of Transportation
Charles YP, Ntilikina Y, Blondel B, Fuentes S, Allia J, Bronsard N, Lleu M, Nicot B, Challier V, Godard J, Kouyoumdjian P, Lonjon N, Marinho P, Berthiller J, Freitas E, Barrey C (2019) Mortality, complication, and fusion rates of patients with odontoid fracture: the impact of age and comorbidities in 204 cases. Arch Orthop Trauma Surg 139:43–51. https://doi.org/10.1007/s00402-018-3050-6
Alswat KA (2017) Gender disparities in osteoporosis. J Clin Med Res 9:382–387. https://doi.org/10.14740/jocmr2970w
Watanabe M, Sakai D, Yamamoto Y, Nagai T, Sato M, Mochida J (2014) Analysis of predisposing factors in elderly people with type II odontoid fracture. Spine J 14:861–866. https://doi.org/10.1016/j.spinee.2013.07.434
Kaesmacher J, Schweizer C, Valentinitsch A, Baum T, Rienmüller A, Meyer B, Kirschke JS, Ryang YM (2017) Osteoporosis is the most important risk factor for Odontoid fractures in the Elderly. J Bone Min Res 32:1582–1588. https://doi.org/10.1002/jbmr.3120
Rizvi SAM, Helseth E, Harr ME, Mirzamohammadi J, Rønning P, Mejlænder-Evjensvold M, Linnerud H (2021) Management and long-term outcome of type II acute odontoid fractures: a population-based consecutive series of 282 patients. Spine J 21:627–637. https://doi.org/10.1016/j.spinee.2020.11.012
Patel A, Smith HE, Radcliff K, Yadlapalli N, Vaccaro AR (2012) Odontoid fractures with neurologic deficit have higher mortality and morbidity. Clin Orthop Relat Res 470:1614–1620. https://doi.org/10.1007/s11999-011-1994-8
Niemeier TE, Dyas AR, Manoharan SR, Theiss SM (2018) Type III odontoid fractures: a subgroup analysis of complex, high-energy fractures treated with external immobilization. J Craniovertebr Junction Spine 9:63–67. https://doi.org/10.4103/jcvjs.JCVJS_152_17
Greene KA, Dickman CA, Marciano FF, Drabier JB, Hadley MN, Sonntag VK (1997) Acute axis fractures. Analysis of management and outcome in 340 consecutive cases. Spine (Phila Pa 1976) 22:1843–1852. https://doi.org/10.1097/00007632-199708150-00009
Jermander E, Sundkvist J, Ekelund J, Möller M, Wolf O, Mukka S (2022) Epidemiology, classification, treatment and mortality of Talus fractures: an observational study of 1794 talus fractures from the Swedish fracture Register. Foot Ankle Surg 28:1444–1451. https://doi.org/10.1016/j.fas.2022.08.008
Rydberg EM, Wennergren D, Stigevall C, Ekelund J, Möller M (2023) Epidemiology of more than 50,000 ankle fractures in the Swedish Fracture Register during a period of 10 years. J Orthop Surg Res 18:79. https://doi.org/10.1186/s13018-023-03558-2
Kruse M, Wolf O, Mukka S, Brüggemann A (2022) Epidemiology, classification and treatment of patella fractures: an observational study of 3194 fractures from the Swedish fracture Register. Eur J Trauma Emerg Surg 48:4727–4734. https://doi.org/10.1007/s00068-022-01993-0
Vaccaro AR, Kepler CK, Kopjar B, Chapman J, Shaffrey C, Arnold P, Gokaslan Z, Brodke D, France J, Dekutoski M, Sasso R, Yoon ST, Bono C, Harrop J, Fehlings MG (2013) Functional and quality-of-life outcomes in geriatric patients with type-II dens fracture. J Bone Joint Surg Am 95:729–735. https://doi.org/10.2106/JBJS.K.01636
Robinson AL, Möller A, Robinson Y, Olerud C (2017) C2 fracture subtypes, incidence, and treatment allocation change with age: a retrospective cohort study of 233 consecutive cases. Biomed Res Int 2017:8321680. https://doi.org/10.1155/2017/8321680
Blixt S, Burmeister F, Mukka S, Bobinski L, Försth P, Westin O, Gerdhem P (2024) Reliability of thoracolumbar burst fracture classification in the Swedish fracture Register. BMC Musculoskelet Disord 25:281. https://doi.org/10.1186/s12891-024-07395-0
Juto H, Möller M, Wennergren D, Edin K, Apelqvist I, Morberg P (2016) Substantial accuracy of fracture classification in the Swedish fracture Register: evaluation of AO/OTA-classification in 152 ankle fractures. Injury 47:2579–2583. https://doi.org/10.1016/j.injury.2016.05.028
Wennergren D, Stjernström S, Möller M, Sundfeldt M, Ekholm C (2017) Validity of humerus fracture classification in the Swedish fracture register. BMC Musculoskelet Disord 18:251. https://doi.org/10.1186/s12891-017-1612-3
Acknowledgements
The authors are in gratitude to statisticians Henrik Albrektsson and Mattias Molin from the Statistska Konsultgruppen for help with the statistical analyses and interpretation of data.
Funding
This study was funded by the Swedish state under the agreement between the Swedish government and the county councils, ALF-agreement (ALFGBG-75120).
Open access funding provided by University of Gothenburg.
Author information
Authors and Affiliations
Contributions
Authors 1, 2 and 3 were responsible for study design, data acquisition, and completing the initial draft of the manuscript. Authors 4, 5, 6 and 7 contributed to the study design and assisted with the final version of the manuscript. All authors have read the final manuscript and given final approval of the manuscript to be published.
Corresponding author
Ethics declarations
Ethical approval
The current study was approved by the Swedish Ethical Review Authority (DNR 2022-02489-01). This study complies with the Declaration of Helsinki.
Competing interests
The authors have no conflicts of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Baranto, D., Steinke, J., Blixt, S. et al. The epidemiology of odontoid fractures: a study from the Swedish fracture register. Eur Spine J (2024). https://doi.org/10.1007/s00586-024-08406-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00586-024-08406-3