
Abstract
Introduction
Revision lumbar fusion is most commonly due to nonunion, adjacent segment disease (ASD), or recurrent stenosis, but it is unclear if diagnosis affects patient outcomes. The primary aim of this study was to assess whether patients achieved the patient acceptable symptom state (PASS) or minimal clinically important difference (MCID) after revision lumbar fusion and assess whether this was influenced by the indication for revision.
Methods
We retrospectively identified all 1–3 level revision lumbar fusions at a single institution. Oswestry Disability Index (ODI) was collected at preoperative, three-month postoperative, and one-year postoperative time points. The MCID was calculated using a distribution-based method at each postoperative time point. PASS was set at the threshold of ≤ 22.
Results
We identified 197 patients: 56% with ASD, 28% with recurrent stenosis, and 15% with pseudarthrosis. The MCID for ODI was 10.05 and 10.23 at three months and one year, respectively. In total, 61% of patients with ASD, 52% of patients with nonunion, and 65% of patients with recurrent stenosis achieved our cohort-specific MCID at one year postoperatively with ASD (p = 0.78). At one year postoperatively, 33.8% of ASD patients, 47.8% of nonunion patients, and 37% of patients with recurrent stenosis achieved PASS without any difference between indication (p = 0.47).
Conclusions
The majority of patients undergoing revision spine fusion experience significant postoperative improvements regardless of the indication for revision. However, a large proportion of these patients do not achieve the patient acceptable symptom state. While revision spine surgery may offer substantial benefits, these results underscore the need to manage patient expectations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The healthcare burden of lumbar fusion procedures has increased significantly over the past decade [1]. Currently, reported rates of revision after primary lumbar fusion range from 4.7 to 22% [2,3,4]. There is an urgent need to better understand the implications of revision lumbar fusion on patient outcomes. Several studies have evaluated outcomes after revision lumbar fusion, with a significant agreement that revision surgery portends poorer outcomes compared to primary fusion [5,6,7,8]. Defining clinically meaningful postoperative benchmarks and outcome measures may help manage patient expectations and set treatment targets.
Patient-reported outcome measures (PROMs) are increasingly emphasized to objectively assess postoperative outcomes and assign value to spinal care [9]. The patient acceptable symptom state (PASS) is derived from PROMs to assess the threshold at which patients are satisfied with postoperative outcomes and is the metric most closely aligned with patient satisfaction [10,11,12]. The PASS value has the potential to significantly improve patient care compared to using the minimal clinically important difference (MCID). While the MCID sets a floor for improvement after surgery, the PASS aligns with postoperative satisfaction. Collectively, these values provide a meaningful clinical context to the statistical significance of postoperative changes to PROMs offering greater clinical relevance.
To our knowledge, no studies have evaluated the number of patients reaching a patient acceptable symptom state after undergoing revision lumbar fusion. We believe this can help guide policy and shape patient expectations regarding the etiology of their symptoms. Therefore, the primary aim of this study was to assess whether patients achieved PASS after revision lumbar fusion and assess whether this was influenced by the indication for revision.
Methods
Study Design and setting
This was a retrospective study of prospectively collected data from a single academic center that was approved by our institutional review board. All adult patients who underwent revision 1–3 level lumbar spinal fusion between 2014 and 2021 were eligible for inclusion. Lumbar fusion patients were identified using a structured query language (SQL) search of current procedural terminal codes (CPT) 22533, 22558, 22612, 22630, and 22633. Subsequently, manual chart review was performed to collect patient demographics, comorbidities, levels fused, surgical approach, and confirm that surgery was a revision. Relevant demographic characteristics including age, sex, body mass index (BMI), medical comorbidities, preoperative diagnoses, smoking status, surgical characteristics, prior surgeries, American Society of Anesthesiologists (ASA) class, and Charlson Comorbidity Index (CCI) were recorded.
Indication for revision surgery was obtained by manual review of operative notes and preoperative clinic visits and included adjacent segment disease (ASD), non-union, and recurrent stenosis. Recurrent stenosis was defined as symptom recurrence at a previously operated level. Revision surgeries for ASD or recurrent stenosis are performed for a diagnosis of lumbar stenosis or radiculopathy at the level that causes either radicular pain/sensory changes or motor weakness. Patients with pseudarthrosis underwent surgery for persistent postoperative axial or radicular pain. In the event that a patient underwent surgery for multiple indications, the patient was categorized according to the primary surgical indication as determined by the surgeon in the preoperative clinic visit and/or operative report. Whether a patient demonstrated axial or radicular pain preoperatively was recorded. Motor examinations were screened for evidence of preoperative weakness, defined as ≤ 3/5 on the motor examination consistent with prior literature [13, 14]. Patients were excluded if they did not undergo a revision spine fusion, underwent fusion of more than three lumbar fusion levels, or underwent revision surgery for a diagnosis of trauma, infection, or malignancy.
Primary endpoints
Primary outcomes consisted of preoperative, three-month postoperative, and one-year postoperative PROMs. PROMs included were Oswestry Disability Index (ODI), collected from our institution’s prospectively collected PROM database (OBERD). The ODI is a ten-item scale in which each item is rated from 0 to 5. Based on these responses, ODI can be calculated by adding total responses and multiplying by two [15].
We evaluated the MCID for ODI using two separate methods. The distribution-based MCID for ODI was calculated by calculating half of the standard deviation (SD) of the mean ΔODI [16, 17]. This was calculated separately for the three-month and one-year timepoints. Utilizing our cohort-specific distribution-based method, the MCID was determined to be 10.05 and 10.23 at three months and one year, respectively. Additionally, we compared our study’s population statistical change to the acceptable MCID in the literature which was set at ≥ 6.8 in line with previous work [18]. This study by Parker et al. defined the MCID for revision spine fusion in the setting of pseudarthrosis using the Health Transition Index (HTI) of the 36-Item Short Form Survey (SF-36). Therefore, if the ΔODI was greater than half of the SD of the overall cohort mean ΔODI, the patient was deemed to have achieved MCID.
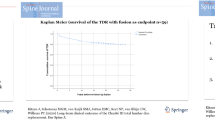
In order to assess if our revision cohort achieved PASS, patients with a three-month or one-year ODI score ≤ 22 were considered to meet the PASS at that given time point in line with a validated measure for primary and revision spinal surgery [19]. This value is considered independent of any preoperative disability and is not evaluated by the degree of postoperative improvement. This value of PASS was determined using the symptom-specific wellbeing item of the Core Outcome Measures Index (COMI) to determine whether satisfaction was achieved and then generating a receiver operating characteristic curve to identify which ODI value was associated with the greatest area under the curve. If the post-treatment score was below the acceptable threshold, the patient is deemed to have achieved a satisfactory level of improvement that meets the PASS threshold.
Statistical analysis
Standard descriptive statistics were reported. Bivariable comparisons were conducted using t-tests or Mann-Whitney U tests for continuous parametric and non-parametric data, respectively. Chi squared testing was performed for categorical data or Fisher’s exact tests in the case of cell counts less than 5. A delta ODI score calculated by subtracting the postoperative minus the preoperative values at three-month and one-year timepoints postoperatively. Patients were compared based on revision diagnosis for analysis of PROM outcome achievement. Patients were then grouped by whether or not PASS was attained postoperatively to assess factors associated with PASS failure. All statistical analysis was conducted using R Studio Version 4.0.2.
Results
We identified 197 patients: 56% (N = 111) with ASD, 28% (N = 56) with recurrent stenosis, and 15% (N = 30) with pseudarthrosis. Patients were predominately White (78%, N = 155) and non-smokers (60%, N = 120) with a mean age of 60.8 years and BMI of 30.9 (Table 1). Patients underwent an average of 2.13 levels fused and 1.87 levels decompressed. In total, 18% (N = 34) required a subsequent (third) revision. Of the patients assessed 37% (N = 74) underwent revision by the same surgeon as the index procedure and 76% (N = 151) within the same hospital system. Patients presented with a baseline preoperative ODI of 51.1 ± 16.9 and improved to an average 34.0 ± 19.0 at three months and 32.4 ± 19.3 at one year postoperatively.
In total, 61% of patients with ASD, 52% of patients with nonunion, and 65% of patients with recurrent stenosis achieved our cohort-specific MCID at one year postoperatively (p = 0.78). When compared to the prior value of MCID from the literature, 71% of ASD, 74% of non-union, and 78% of recurrent stenosis patients achieved MCID also without significant difference between groups (p = 0.65). Moreover, we observed no significant difference between surgical indication groups at the earlier three-month timepoint using either the cohort-specific MCID or the prior MCID reported in the literature (Table 2).
At three months, 24.5% of ASD patients, 25% of nonunion patients, and 31.7% of patients with recurrent stenosis achieved PASS. At one year, achievement of PASS rose to 33.8% of ASD patients, 47.8% of nonunion patients, and 37% of patients with recurrent stenosis. At both three-month and one-year timepoints, there was no difference between indication groups in likelihood of achieving PASS (p = 0.67 and p = 0.47, respectively) (Table 2). Patient characteristics associated with a failure to achieve PASS included increased BMI and a higher comorbidity burden. The location of pain symptoms whether concurrent axial and radicular pain (72.7% vs. 74.5%, p = 0.968), axial pain only (3.19% vs. 7.27%, p = 0.424), or radicular pain only (19.1% vs. 20.0%, p = 1.000) were similar between groups. There were no other patient or surgical characteristics associated with a failure to achieve PASS in our cohort (Table 3).
Discussion
Revision lumbar fusion represents a technically challenging procedure with high medical expenditures, increased risk of complications, and lower likelihood of improvement as compared to primary spine fusions [5, 6, 20,21,22]. Reoperation is most commonly due to complications associated with nonunion, ASD, or recurrent stenosis [23]. In the current analysis, we found that most patients undergoing revision spine fusion experience clinically noticeable improvements in their symptoms by one-year postoperatively regardless of indication. Despite the key finding that the majority of patients in our cohort achieved MCID at one year irrespective of indication, less than half of patients reached a patient acceptable symptom state.
A recent retrospective analysis of patients undergoing revision lumbar fusion found that revision fusion reduces disability in patients with ASD, pseudoarthrosis, and recurrent stenosis at two-year follow-up [6], which supports our study’s observation that the majority of patients achieve MCID at one year. In a separate cohort of patients, Suh et al. previously described poorer PROMs and higher reoperation rates among ASD patients compared to other revision indications [8]. However, these findings remain equivocal, as Lambrechts et al. recently found poorer outcomes across revision lumbar fusions broadly compared to primary lumbar fusion, but that revision lumbar fusion outcomes were similar across diagnostic indications [5]. Differences in patient diagnosis may also lead to differences in how ODI measures disease states. It is possible that ODI better captures low back pain disability rather than lower extremity symptoms common in patients undergoing surgery for ASD or recurrent stenosis. Rather, patients who underwent surgery for pseudarthrosis are typically indicated for unrelenting lower back pain and may experience improvement primarily captured by such a tool as the ODI. Ultimately, despite these differences in our cohort, 71–78% of our demonstrated clinical improvement in their self-reported disability suggesting good efficacy of these procedures in appropriately indicated patients.
Despite the high number of patients experiencing some degree of postoperative improvement, the majority did not reach an “acceptable symptom state” as defined in the literature. Yet, it is important to highlight that the average ΔODI improvement across our cohort at three months and one year post-revision was 13.36 and 18.66, respectively. In comparison, previous reports have documented mean ODI improvements of 6.58, and 5.0 at 6 months following revision lumbar fusion [24, 25]. Similarly, Djurasovic et al. highlighted a modest improvement in ODI by 11.4 points in comparison to significantly greater improvements in patients undergoing primary lumbar fusion [7]. However, this ultimately leads to concerns in the use of floor metrics of ODI improvement to determine whether an intervention is efficacious. An entire cohort could theoretically meet an MCID threshold set at 6.8. However, this minimal improvement from baseline symptoms would not be considered a good clinical outcome to a patient or a provider and highlights the need for better metrics to use in patient care. Despite a relatively low percentage of patients in our study failing to achieve PASS, it is evident that our patients experienced some noticeable improvement from their baseline within clinical expectations set by prior literature.
We suspect the reasons of this discrepancy are likely multifactorial. Unrealistic expectations about the symptomatic improvement after revision surgery may contribute to postoperative dissatisfaction. For instance, patients with inferior preoperative quality of life PROMs exhibit worse outcomes postoperatively, yet these same patients frequently have the highest expectations of postoperative recovery [26, 27], and these patients are less satisfied following surgery [26, 28]. In a cohort of patients undergoing minimally invasive transforaminal lumbar interbody fusion, patients with severe back and/or leg pain preoperatively demonstrated consistently poorer improvement in ODI and other PROMs [28]. Patients undergoing revision spine surgery may also define an acceptable symptom state at a higher level of disability compared to patients undergoing a primary spine fusion. Yet, no sensitivity analyses have been performed in PASS-determining literature to compare PASS between primary and revision spine fusion patients. With only one value of PASS for ODI available, which was validated in a population mainly undergoing primary elective lumbar fusion, it is unlikely that this can be used clinically for patients undergoing revision spinal fusion at this time. Future spine literature must at minimum begin to define these values in different patient populations undergoing various interventions. Psychological factors, comorbidity burden, and adherence to rehabilitation protocols all contribute to failure to achieve symptomatic improvement and must be optimized [29]. In our cohort, patients with more comorbidities were less likely to achieve PASS consistent with prior literature suggesting poorer outcomes. Preoperative depression and affective disorders have been particularly linked to inferior outcomes after primary and revision spine surgery with up to 8-fold poorer improvements in ODI if they were in the worst quartile of depression [30, 31]. Nonetheless, in two separate cost-effective analyses, Adogwa et al. demonstrated two year cost per quality associated life year gained of approximately $60,000 for spine fusion for either recurrent stenosis or ASD with improved return to work [32, 33]. Collectively, our results add to the literature by demonstrating the significant benefit and potential for robust outcomes following revision fusion.
Our study’s observed disparity between MCID and PASS metrics is consistent with the conclusions drawn from prior studies and inconsistencies in the applications of values of clinically important change derived from PROMs [34]. Both PASS and MCID metrics may be influenced by preoperative disability and patient efficacy. For example, it is possible that PASS may be significantly higher among patients with significant comorbidities and with more complex spinal disease, as is frequently the case at our high-volume tertiary care urban academic institution. Especially among patients undergoing revision spine surgery, the benefits of surgery are significant even if the absolute symptom state is not considered acceptable in some patient populations [34, 35]. Recently, Shahi et al. suggested postoperative improvement is best assessed by PASS in patients with minimal or moderate preoperative disability while MCID is an optimal metric for patients with severe preoperative disability [36]. In their population of 212 primary minimally invasive spine fusion patients, 19% achieved PASS but not MCID and 10% of achieved MCID but not PASS, with primary difference being a poorer preoperative ODI in the second group. Furthermore, these findings should be utilized to manage patient expectations after failed primary fusion and clinicians must counsel patients that appreciable clinical improvement may not be experienced until one year postoperatively. Despite the strong clinical rationale behind implementing PASS in value-based care, future groups must further develop PASS in the spinal literature using multi-institutional cohorts with a wide range of patient risk factors and surgical characteristics for these values to become universally adopted.
There are several limitations aside from those inherent to any retrospective study that warrant discussion. First, the value for PASS utilized was defined in a heterogenous population of spinal fusion patients to expand the applicability and generalizability of the value to all lumbar spine surge surgery for degenerative disease. However, it is likely that our revision fusion-only population may represent a skewed distribution of patients from that original study. At this point in time, this represents the best PASS threshold to utilize in this study based on a recent systematic review of all PASS thresholds in spine surgery [19]. Additionally, no studies have determined the PASS for other PROMs within lumbar spine surgery. Moreover, the ODI may not appropriately capture the benefits of revision laminectomy and fusion for patients undergoing surgery for adjacent segment disease or recurrent stenosis. In the current study, we also used a distribution-based calculation for MCID, which is well-validated but may be less clinically relevant than anchor-based calculations. However, anchor questions can only be assessed in prospective formats, which we believe should help guide future research.
Conclusion
The majority of patients undergoing revision lumbar fusion experience significant improvements from their baseline status regardless of diagnostic indication for surgery. However, many patients do not reach a patient acceptable symptom state despite this improvement. These results underscore the need for continued improvement in setting postoperative patient expectations and validating interpretation of PROMs across various patient populations including revision spine procedures.
References
Martin BI, Mirza SK, Spina N et al (2019) Trends in lumbar fusion procedure rates and associated hospital costs for degenerative spinal diseases in the United States, 2004 to 2015. Spine (Phila Pa 1976) 44:369–376. https://doi.org/10.1097/brs.0000000000002822
Försth P, Ólafsson G, Carlsson T et al (2016) A randomized, controlled trial of fusion surgery for lumbar spinal stenosis. N Engl J Med 374:1413–1423. https://doi.org/10.1056/nejmoa1513721
Kim CH, Chung CK, Park CS et al (2013) Reoperation rate after surgery for lumbar spinal stenosis without spondylolisthesis: a nationwide cohort study. Spine J 13:1230–1237. https://doi.org/10.1016/j.spinee.2013.06.069
Martin BI, Mirza SK, Comstock BA et al (2007) Reoperation rates following lumbar spine surgery and the influence of spinal fusion procedures. Spine (Phila Pa 1976) 32:382–387. https://doi.org/10.1097/01.brs.0000254104.55716.46
Lambrechts MJ, Toci GR, Siegel N et al (2023) Revision lumbar fusions have higher rates of reoperation and result in worse clinical outcomes compared to primary lumbar fusions. Spine J 23:105–115. https://doi.org/10.1016/j.spinee.2022.08.018
Adogwa O, Owens R, Karikari I et al (2013) Revision lumbar surgery in elderly patients with symptomatic pseudarthrosis, adjacent-segment disease, or same-level recurrent stenosis. Part 2. A cost-effectiveness analysis. J Neurosurg Spine 18:147–153. https://doi.org/10.3171/2012.11.spine12226
Djurasovic M, Glassman SD, Howard JM et al (2011) Health-related quality of life improvements in patients undergoing lumbar spinal fusion as a revision surgery. Spine (Phila Pa 1976) 36:269–276. https://doi.org/10.1097/BRS.0b013e3181cf1091
Suh S-P, Jo Y-H, Jeong HW et al (2017) Outcomes of revision surgery following instrumented Posterolateral Fusion in degenerative lumbar spinal stenosis: a comparative analysis between pseudarthrosis and adjacent segment disease. Asian Spine J 11:463–471. https://doi.org/10.4184/asj.2017.11.3.463
Reuben DB, Tinetti ME (2012) Goal-oriented patient care — an alternative health outcomes paradigm. N Engl J Med 366:777–779. https://doi.org/10.1056/nejmp1113631
Galea VP, Ingelsrud LH, Florissi I et al (2020) Patient-acceptable symptom state for the Oxford hip score and forgotten joint score at 3 months, 1 year, and 2 years following total hip arthroplasty: a registry-based study of 597 cases. Acta Orthop 91:372–377. https://doi.org/10.1080/17453674.2020.1750877
Connelly JW, Galea VP, Rojanasopondist P et al (2019) Patient acceptable symptom state at 1 and 3 years after total knee arthroplasty. J Bone Joint Surg Am 101:995–1003. https://doi.org/10.2106/jbjs.18.00233
Kvien TK, Heiberg T, Hagen KB (2007) Minimal clinically important improvement/difference (MCII/MCID) and patient acceptable symptom state (PASS): what do these concepts mean? Ann Rheum Dis 66:iii40–iii41. https://doi.org/10.1136/ard.2007.079798
Kreitz T, Huang R, Beck D et al (2018) Prolonged preoperative weakness affects recovery of motor function after Anterior Cervical Diskectomy and Fusion. JAAOS - J Am Acad Orthop Surg 26:67–73. https://doi.org/10.5435/JAAOS-D-16-00606
Pinter ZW, Sebastian AS, Wagner SC et al (2022) Indicators for substantial neurological recovery following elective Anterior Cervical Discectomy and Fusion. Clin Spine Surg 35:E698–E701. https://doi.org/10.1097/BSD.0000000000001340
Fairbank JCT, Pynsent PB (2000) The Oswestry disability index. Spine (Phila Pa 1976) 25:2940–2953. https://doi.org/10.1097/00007632-200011150-00017
Norman GR, Sloan JA, Wyrwich KW (2003) Interpretation of changes in health-related quality of life. Med Care 41:582–592. https://doi.org/10.1097/01.mlr.0000062554.74615.4c
Bendich I, Tarity TD, Alpaugh K et al (2023) Identifying aseptic revision total knee arthroplasty diagnoses that achieve minimal clinically important difference and patient acceptable symptom state. J Arthroplasty 38:1309–1312. https://doi.org/10.1016/j.arth.2023.01.020
Parker SL, Adogwa O, Mendenhall SK et al (2012) Determination of minimum clinically important difference (MCID) in pain, disability, and quality of life after revision fusion for symptomatic pseudoarthrosis. Spine J 12:1122–1128. https://doi.org/10.1016/j.spinee.2012.10.006
van Hooff ML, Mannion AF, Staub LP et al (2016) Determination of the Oswestry Disability Index score equivalent to a satisfactory symptom state in patients undergoing surgery for degenerative disorders of the lumbar spine—a spine Tango registry-based study. Spine J 16:1221–1230. https://doi.org/10.1016/j.spinee.2016.06.010
Elgafy H, Vaccaro AR, Chapman JR, Dvorak MF (2012) Rationale of revision lumbar spine surgery. Global Spine J 2:007–014. https://doi.org/10.1055/s-0032-1307254
Eichholz KM, Ryken TC (2003) Complications of revision spinal surgery. Neurosurg Focus 15:1–4. https://doi.org/10.3171/foc.2003.15.3.1
Kim WJ, Shin HM, Song DG et al (2021) Comparison of clinical outcomes and complications of primary and revision surgery using a combined anterior and posterior approach in patients with adult spinal deformity and sagittal imbalance. Clin Orthop Surg 13:196. https://doi.org/10.4055/cios20217
Gerling MC, Leven D, Passias PG et al (2016) Risk factors for reoperation in patients treated surgically for lumbar stenosis. Spine (Phila Pa 1976) 41:901–909. https://doi.org/10.1097/brs.0000000000001361
Montenegro TS, Gonzalez GA, Saiegh FA et al (2021) Clinical outcomes in revision lumbar spine fusions: an observational cohort study. J Neurosurg Spine 35:437–445. https://doi.org/10.3171/2020.12.spine201908
Montenegro TS, Singh A, Elia C et al (2021) Independent predictors of revision lumbar fusion outcomes and the impact of spine surgeon variability: does it matter whether the primary surgeon revises? Neurosurgery 89:836–843. https://doi.org/10.1093/neuros/nyab300
Mancuso CA, Duculan R, Stal M, Girardi FP (2015) Patients’ expectations of lumbar spine surgery. Eur Spine J 24:2362–2369. https://doi.org/10.1007/s00586-014-3597-z
McGirt MJ, Bydon M, Archer KR et al (2017) An analysis from the Quality outcomes Database, Part 1. Disability, quality of life, and pain outcomes following lumbar spine surgery: predicting likely individual patient outcomes for shared decision-making. J Neurosurg Spine 27:357–369. https://doi.org/10.3171/2016.11.spine16526
Jacob KC, Patel MR, Collins AP et al (2022) The effect of the severity of preoperative leg pain on patient-reported outcomes, minimum clinically important difference achievement, and patient satisfaction after minimally invasive transforaminal lumbar interbody fusion. World Neurosurg 167:e1196–e1207. https://doi.org/10.1016/j.wneu.2022.09.004
Maitra S, Mikhail C, Cho SK, Daubs MD (2020) Preoperative maximization to reduce complications in spinal surgery. Global Spine J 10:45S–52. https://doi.org/10.1177/2192568219882349. S
Adogwa O, Parker SL, Shau DN et al (2012) Preoperative Zung Depression Scale predicts outcome after revision lumbar surgery for adjacent segment disease, recurrent stenosis, and pseudarthrosis. Spine J 12:179–185. https://doi.org/10.1016/j.spinee.2011.08.014
Adogwa O, Parker SL, Shau DN et al (2013) Preoperative Zung depression scale predicts patient satisfaction independent of the extent of improvement after revision lumbar surgery. Spine J 13:501–506. https://doi.org/10.1016/j.spinee.2013.01.017
Adogwa O, Parker SL, Shau DN et al (2012) Cost per quality-adjusted life year gained of laminectomy and extension of instrumented fusion for adjacent-segment disease: defining the value of surgical intervention. J Neurosurg Spine 16:141–146. https://doi.org/10.3171/2011.9.SPINE11419
Adogwa O, Parker SL, Shau DN et al (2012) Cost per quality-adjusted life year gained of revision neural decompression and instrumented fusion for same-level recurrent lumbar stenosis: defining the value of surgical intervention. J Neurosurg Spine 16:135–140. https://doi.org/10.3171/2011.9.SPINE11308
Issa TZ, Lee Y, Henry TW et al (2023) Values derived from patient reported outcomes in spine surgery: a systematic review of the minimal clinically important difference, substantial clinical benefit, and patient acceptable symptom state. Eur Spine J. https://doi.org/10.1007/s00586-023-07896-x
Tanghe KK, Beiene ZA, McLawhorn AS et al (2023) Metrics of clinically important changes in total hip arthroplasty: a systematic review. J Arthroplast 38:383–388. https://doi.org/10.1016/j.arth.2022.09.007
Shahi P, Subramanian T, Maayan O et al (2023) Preoperative disability influences effectiveness of MCID and PASS in predicting patient improvement following lumbar spine surgery. Clin Spine Surg. https://doi.org/10.1097/bsd.0000000000001517
Funding
The authors, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity for the preparation of this article. Relevant disclosures related to the topic of the article are listed on disclosure forms.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
LEVEL OF EVIDENCE: III
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Issa, T.Z., Tarawneh, O.H., Ezeonu, T. et al. The attainment of a patient acceptable symptom state in patients undergoing revision spine fusion. Eur Spine J (2024). https://doi.org/10.1007/s00586-024-08358-8
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00586-024-08358-8