
Abstract
Purpose
To systematically investigate all published literature on spinal gout regarding location demographics, patient characteristics, treatment, and outcomes.
Methods
We performed a systematic literature search of Medline and EMBASE from inception until April 15, 2023. Two investigators performed data extraction and quality assessment of location demographics and patient characteristics and outcomes of all article types describing spinal gout.
Results
A total of 214 articles (204 case reports and 10 case series) were included, encompassing 315 subjects with spinal gout (81% male, mean age 58.1 years; range: 16–92). Most cases (36%) were between the age of 60–69 years. We observed an increase in publications and cases from 1950 to the present. Most patients were from institutions in Asia (n = 119, 37.8%) and North America (n = 96, 30.5%). Reported symptoms frequently included back pain (75%), radiating pain to extremities (27.3%), and weakness in the extremities (26.3%). The lumbar spine was most often affected. Pharmacological treatment was described for 108 (34.2%) patients. Surgery was performed for 146 (46.3%) of patients, of which 4.8% had postoperative complications. Three patients (2%) required secondary surgery for recurrence.
Conclusion
Published cases of spinal gout have increased over the last decades. Patient characteristics of spinal gout were similar to findings in systemic gout. Trends identified in patient characteristics and treatment outcomes may help guide patient management and improve our understanding of spinal gout.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gout is a common metabolic disorder affecting the joint and soft tissues, as a result of increased uric acid causing depositions of monosodium urate crystals [1]. In patients with gout, long term tophus formation and joint flares may progress to joint damage [2]. The etiology of gout has been well established. Increased cardiovascular and inflammatory comorbidities are usually observed, including obesity, diabetes, hypertension, chronic kidney disease, and dyslipidemia [3].
The first presentation is usually a gout flare, presenting as an inflammatory arthritis in the lower extremities [4]. Frequent gouty depositions include the feet, ankles, and wrists, but nonarticular sites such as olecranon bursae, ears, and tendons of hands and feet may also be affected [5].
Gouty presentation at the level of the spine, however, is a relatively uncommon location site.
According to the 2020 American College of Rheumatology guideline for gout, treatment includes urate lowering therapy for tophus gout, radiographic damage or frequent flares in gout, with concurrent anti-inflammatory prophylaxis therapy [6]. However, when gout presents at the spine, surgical treatment may be required in some cases [7, 8]. The first case of spinal gout was reported in 1950 by Kersley and colleagues [9]. Since then, various cases and series have been reported in the literature [7, 8, 10], including literature reviews [11,12,13]. Hence, in this systematic review, we aimed to assess the location demographics and epidemiological knowledge of patient characteristics, treatment and outcomes of spinal gout. In addition, we performed analyses not reported previously, including aggregating data on location and patient characteristics including comorbidities and symptoms. Thirdly, we aimed to analyze study specific quality assessment with regards to selection, ascertainment, causality, and reporting of each study.
Materials and methods
Data sources and literature search
We conducted this systematic review using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [14]. The databases of Medline and EMBASE were systematically searched on April 15, 2023 for articles reporting gout at the spine. A search syntax was constructed with the terms “Spine” AND “Gout” including relevant synonyms and descriptions. The full search syntax can be accessed in Supplementary Appendix A. Title and abstract screening was performed by two authors independently, discussing discrepancies by consensus. We considered all article types, did not place any restrictions on language, and performed cross-referencing to identify additional articles not included in the electronic search.
Data extraction and quality assessment
Data extraction and quality assessment were performed independently by each investigator, with differences discussed until consensus was reached. Case reports were defined as articles describing one or two patients with spinal gout, and case series were defined as three or more patients with spinal gout [15]. Quality assessment was performed using the methodological quality and synthesis of case series and case reports tool from Murad et al. [16]. The study domains selection, ascertainment, causality, and reporting of each study were assessed. Data were extracted on country, patient characteristics including age, sex, symptoms, comorbidities, duration of symptoms, imaging modalities used, biochemical results, treatment, follow-up, complications and outcomes after conservative and surgical treatment.
Statistical analysis
A p-value less than 0.05 was considered as statistical significance. Data were presented using mean and standard deviation (SD) for normal data, and non-normal data using median ± interquartile range (IQR). Differences between groups were compared using t-tests. Data on cases for each country were visualized using the r package “rworldmap”. Statistical analysis was performed using R, version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study selection and location demographics
A total of 1438 articles were assessed for full-text eligibility after discarding duplicates. After full-text screening, 69 articles were excluded with reason based on our inclusion criteria, ultimately resulting in 214 articles in the systematic review (Fig. 1). A total of 204 case reports and 10 case series were included, describing 315 patients with gout at the spine.

Study selection flowchart
Between 1950 and 2023, a steady increase of published studies was observed, as well as an increase in the number of cases with spinal gout (Fig. 2).

The number of cases and publication between 1950 and the present
Location demographics of published cases by country is shown in Fig. 3. Most patients were from institutions in Asia (N patients = 119, N studies = 71), followed by North America (N patients = 96, N studies = 71) Europe (N patients = 63, N studies = 49), South America (N patients = 22, N studies = 11), Australia (N patients = 10, N studies = 9), and Africa (N patients = 5, N studies = 5).

The worldwide distribution of spinal gout cases
Patient characteristics
Sex was reported for 299 cases, including 242 males and 57 females, ratio M/F = 4.2 to 1. The mean age of all cases (reported for 290 cases) was 58.1 years (SD = 16 years, range: 16–92 years). Females were on average older than males (65 vs. 56 years, p < 0.001). When stratified by age-group, 26 (9%) subjects were younger than 30 years, 24 subjects (9%) were between 30 and 39 years, 25 subjects (9%) between 40 and 49 years, 46 subjects (16%) between 50 and 59 years, 104 subjects (36%) between 60 and 69 years, 50 subjects (17%) between 70 and 79 years, and 15 subjects (5%) over the age of 80. Erythrocyte sedimentation rate (ESR) was reported for 61 subjects, mean ESR 70 mm/h (SD: 40 mm/h), normal for 12 subjects and elevated for 49 subjects. C-reactive protein was reported for 76 subjects, median 67.4 mg/L (IQR: 11—127.5 mg/L), which was normal for 19 subjects and elevated in 57 subjects. White blood cells were reported for 69 subjects, median 10.35 × 109/L (IQR:7.8–13.5 × 109/L). Serum uric acid was reported for 161 subjects and was elevated in 133 subjects and normal for 28 subjects, median value 10.1 mg/dl; IQR: 8.5–11.9 mg/dl.
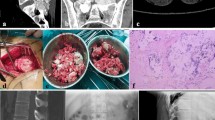
Imaging modalities used included computed tomography (CT) (n = 205, 65%), including dual energy CT (n = 27, 9%), magnetic resonance imaging (n = 168, 53%), spinal radiographs (n = 104, 33%), myelography (n = 13, 4%), bone scintigraphy (n = 13, 4%), and positron emission tomography CT (n = 7, 2%). The most common affected spine level was the lumbar spine (n = 184), followed by the cervical spine (n = 73), thoracic spine (n = 57), and the sacroiliac joint (n = 55). Multiple level spine involvement was observed for 86 patients (27.3%). A total of 171 subjects had a history of previous gout, of which 86 had the duration of gout specified (median: 10 years; IQR: 7–15 years). At presentation, 119 patients had concurrent peripheral tophi and 38 patients had no evidence of tophi, which was not described for the remaining cases. Comorbidities were reported for 133 subjects and most frequently included hypertension, diabetes mellitus, chronic kidney disease, obesity, and dyslipidemia (Table 1).
Symptoms, diagnosis, and treatment
Symptoms were reported in 267 patients and most frequently included back pain (n = 200), radiating pain to extremities (n = 73), weakness in the legs (n = 58) and arms (n = 12), fever (32), and sensory dysfunction (n = 31). Other severe symptoms included incontinence (n = 12), paraplegia (n = 9), and quadriplegia (n = 5) (Table 2). Symptom duration was reported for 117 subjects and was a median of 35 days; IQR: 7–152 days.
Final diagnosis of gout was established by surgery (n = 150), clinical presentation and imaging (n = 74), biopsy (n = 34), aspiration (n = 13), dual energy CT (n = 19), and not reported in the remaining cases. Nonoperative treatment was specified for 108 subjects and included (in various combinations) treatment with allopurinol (n = 65), colchicine (n = 55), glucosteroids (n = 34), nonsteroidal anti-inflammatory drugs (n = 22), febuxostat (n = 14), benzbromarone (n = 7), and anakinra (n = 2). Improvement following conservative therapy was reported for 96 subjects (88.9%), as well as partial improvement of motor function but not sensibility (n = 1), no improvement (n = 4), and death (n = 3).
Surgical treatment was refused by three patients. A total of 146 (46%) subjects were treated with surgery, which most frequently consisted of a decompressive laminectomy. Symptom resolution after surgery was reported for 124 subjects, including improvement (n = 114, 92%), no improvement (n = 4), sensibility improvement but no motor function (n = 2), remaining paraplegia (n = 1), and death (n = 3).
Follow-up, complications, and outcomes
Three patients died before surgery due to pneumonia (n = 2), with the other reason not specified. Following surgery, complications were reported for seven patients (4.8%): Three patients died after surgery due to sepsis (n = 2) and a chest infection (n = 1). Other complications following surgery included wound infection (n = 1), bed sores and urinary tract infection (n = 1), hemorrhage (n = 1), and superficial wound dehiscence (n = 1).
Follow-up was described for 78 patients, with a median follow-up of 6 months (IQR: 46–365 days). Three patients required a secondary laminectomy due to recurrent stenosis (n = 2) and new onset weakness after the first surgery (n = 1). No other cases of recurrence were reported.
Discussion
In this systematic review we identified 315 cases with gout at the axial skeleton from inception till 2023. Since the first case published in 1950, we observed a gradual increase of cases and publications on spinal gout over time. This may be due to the increased awareness of clinicians that patients with preexisting gout can also present with gout at the spine, as well as the general increase in publications in published literature over time.
Most patients were reported from institutions in Asia and North America, though it was also evident that authors from multiple continents reported on cases of spinal gout.
Furthermore, the majority of spinal gout cases were predominantly male between 60 and 69 years of age, and the mean age of males presenting with spinal gout was much lower compared to females. These findings and characteristics are in line with observations seen in patients systemic gout [1].
The estimated prevalence of axial gout ranged from 14 to 35% in patients with gout, which is based on small studies with varying methodology and demographics [17,18,19,20]. The pathophysiology of spinal gout remains to be elucidated, though the lumbar spine is most commonly affected in line with previous results [12].
The presence of gout did not always correlate with back pain in some series [17, 18], though it was the most reported symptom in our study population. Furthermore, compared to patients with no axial gout, disease duration [17, 18, 20], patients age [17, 18, 20], serum uric acid [18, 20], or urate lower therapy [17, 18, 20], hypertension [18, 20] were not associated with the presence of axial gout. The presence of diabetes was associated with spinal gout [18, 20]. The presence of peripheral tophi however, was not conclusive as it was associated with gout in the prospective series of de Mello et al. [17] but not in the retrospective series of Konatapali et al. [18]. A portion of patients presenting with spinal gout in our series did not have evidence of peripheral tophi. The previous review by Zhang et al. [12] highlighted the important distinction between gout at the spine without and with peripheral involvement of tophi, the latter being an important discriminating feature in the recently updated gout classification criteria [4].
Conservative treatment with urate lower therapy and anti-inflammatory medication is usually the first treatment of choice in patients with spinal gout [6]. In the presence of progressive neurological deficits, or new onset of neurological symptoms, surgical resection and decompression is usually initiated. In our review, the complication rate following spine surgery was low, which was also observed for reoperation rates.
Earlier diagnosis is important to prevent progression with neurological symptoms, including spinal stenosis or spinal cord injury. In the last decade, dual energy CT has become a promising diagnostic modality for patients with gout. It is a noninvasive method to quantify urate crystal deposits, which may aid clinicians for establishing the diagnosis of gout in complex and atypical patients [21]. Clinical findings, urate levels, and imaging features should be considered when evaluating patients for spinal gout or tophi. Nonetheless, histological confirmation of gout remains the gold standard for diagnosis to date.
The published literature may be an underestimation of the real reported cases with spinal gout. Indeed, spinal tophi depositions in gout may also be present without evoking clinical symptoms, for which diagnosis can be difficult. Given that the burden of obesity and other attributable factors are projected to increase the coming decades [22], an increase in cases of spinal gout may also be expected. It is important to increase awareness of spinal gout, so that clinicians are aware of the (atypical) presentation, and patient factors, in order to optimize treatment and outcomes for this patient population.
Strengths and limitations
The limitations should be mentioned. Selective reporting bias could not be fully ascertained as a subset of included studies had missing population and outcome data (Supplementary Appendix B). Furthermore, systematic reviews based on case reports and case series are inherently limited by incomplete validity assessments, and the inability to appraise publication bias. Nevertheless, in the current study we have reviewed and summarized the largest collection of patients with gout at the spine, using our extensive and expert literature search without language restriction. We also assessed study-specific level quality, and attempted to exclude bias with our selection process.
Conclusion
Published cases of spinal gout have increased over the last decades, yet, the prevalence of spinal gout remains underestimated. Patient characteristics of spinal gout were similar to findings in systemic gout, most commonly affecting men, at an earlier stage compared to women. Surgical treatment has low complication rates, and good clinical outcome, which may be suitable for patients with a progression of symptoms or after conservative management has become inadequate. Trends identified in patient characteristics and treatment outcomes may help guide patient management and improve our understanding of spinal gout.
Data availability
Available upon reasonable request from the corresponding author.
References
Dehlin M, Jacobsson L, Roddy E (2020) Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol 16:380–390. https://doi.org/10.1038/s41584-020-0441-1
Chhana A, Dalbeth N (2014) Structural joint damage in gout. Rheum Dis Clin North Am 40:291–309. https://doi.org/10.1016/j.rdc.2014.01.006
Choi HK, McCormick N, Yokose C (2022) Excess comorbidities in gout: the causal paradigm and pleiotropic approaches to care. Nat Rev Rheumatol 18:97–111. https://doi.org/10.1038/s41584-021-00725-9
Taylor WJ, Fransen J, Jansen TL, Dalbeth N, Schumacher HR, Brown M et al (2015) Study for updated gout classification criteria: identification of features to classify gout. Arthritis Care Res (Hoboken) 67:1304–1315. https://doi.org/10.1002/acr.22585
Grassi W, De Angelis R (2012) Clinical features of gout. Reumatismo 63:238–245. https://doi.org/10.4081/reumatismo.2011.238
FitzGerald JD, Dalbeth N, Mikuls T, Brignardello-Petersen R, Guyatt G, Abeles AM et al (2020) 2020 American college of rheumatology guideline for the management of gout. Arthritis Care Res (Hoboken) 72:744–760. https://doi.org/10.1002/acr.24180
Zhou MMX, Wu MMM, Sang MML, Wu MMJ (2023) Clinical observation of posterior decompression, fusion and fixation in the treatment of spinal gout: a case series. J Orthop Surg Res 18:303. https://doi.org/10.1186/s13018-023-03791-9
Xie L, Zhang X, Xi Z, Li J (2019) Percutaneous endoscopic treatment for cervical ligamentum flavum gouty tophus: a case report. Medicine (Baltimore) 98:e15665. https://doi.org/10.1097/MD.0000000000015665
Kersley GD, Mandel L, Jeffrey MR (1950) Gout; an unusual case with softening and subluxation of the first cervical vertebra and splenomegaly. Ann Rheum Dis 9:282–304. https://doi.org/10.1136/ard.9.4.282
Kao Y, Wang Z, Leng J, Qu Z, Zhuang X, Ma H et al (2020) Thoracic gout tophus with abdominal wall protrusion: a case report. Medicine (Baltimore) 99:e19348. https://doi.org/10.1097/MD.0000000000019348
Hou LC, Hsu AR, Veeravagu A, Boakye M (2007) Spinal gout in a renal transplant patient: a case report and literature review. Surg Neurol 67:65–73
Zhang T, Yang F, Li J, Pan Z (2019) Gout of the axial joint-A patient level systemic review. Semin Arthritis Rheum 48:649–657. https://doi.org/10.1016/j.semarthrit.2018.04.006
Thornton FJ, Torreggiani WC, Brennan P (2000) Tophaceous gout of the lumbar spine in a renal transplant patient: a case report and literature review. Eur J Radiol 36:123–125. https://doi.org/10.1016/s0720-048x(00)00214-x
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700
Harlianto NI, Kuperus JS, Mohamed Hoesein FAA, de Jong PA, de Ru JA, Öner FC et al (2022) Diffuse idiopathic skeletal hyperostosis of the cervical spine causing dysphagia and airway obstruction: an updated systematic review. Spine J 22:1490–1503. https://doi.org/10.1016/j.spinee.2022.03.002
Murad MH, Sultan S, Haffar S, Bazerbachi F (2018) Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med 23:60–63. https://doi.org/10.1136/bmjebm-2017-110853
de Mello FM, Helito PV, Bordalo-Rodrigues M, Fuller R, Halpern AS (2014) Axial gout is frequently associated with the presence of current tophi, although not with spinal symptoms. Spine (Phila Pa 1976). https://doi.org/10.1097/BRS.0000000000000633
Konatalapalli RM, Lumezanu E, Jelinek JS, Murphey MD, Wang H, Weinstein A (2012) Correlates of axial gout: a cross-sectional study. J Rheumatol 39:1445–1449. https://doi.org/10.3899/jrheum.111517
Konatalapalli RM, Demarco PJ, Jelinek JS, Murphey M, Gibson M, Jennings B et al (2009) Gout in the axial skeleton. J Rheumatol 36:609–613. https://doi.org/10.3899/jrheum.080374
Jin HJ, Son ES, Kim DH (2020) The frequency of axial deposition in korean patients with gout at a tertiary spine center. Front Med (Lausanne) 7:339. https://doi.org/10.3389/fmed.2020.00339
Bongartz T, Glazebrook KN, Kavros SJ, Murthy NS, Merry SP, Franz WB 3rd et al (2015) Dual-energy CT for the diagnosis of gout: an accuracy and diagnostic yield study. Ann Rheum Dis 74:1072–1077. https://doi.org/10.1136/annrheumdis-2013-205095
Chong B, Jayabaskaran J, Kong G, Chan YH, Chin YH, Goh R et al (2023) Trends and predictions of malnutrition and obesity in 204 countries and territories: an analysis of the Global Burden of Disease Study 2019. EClinicalMedicine 16(57):101850. https://doi.org/10.1016/j.eclinm.2023.101850
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Informed consent
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Harlianto, N.I., Harlianto, Z.N. Patient characteristics, surgical treatment, and outcomes in spinal gout: a systematic review of 315 cases. Eur Spine J 32, 3697–3703 (2023). https://doi.org/10.1007/s00586-023-07942-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07942-8