
Abstract
Purpose
Clinical guidelines recommend epidural steroid injection (ESI) as a treatment option for severe disc-related sciatica, but there is considerable uncertainty about its effectiveness. Currently, we know very little about factors that might be associated with good or poor outcomes from ESI. The aim of this systematic review was to synthesise and appraise the evidence investigating prognostic factors associated with outcomes following ESI for patients with imaging confirmed disc-related sciatica.
Methods
The search strategy involved the electronic databases Medline, Embase, CINAHL Plus, PsycINFO and reference lists of eligible studies. Selected papers were quality appraised independently by two reviewers using the Quality in Prognosis Studies tool. Between-study heterogeneity precluded statistical pooling of results.
Results
3094 citations were identified; 15 studies were eligible. Overall study quality was low with all judged to have moderate or high risk of bias. Forty-two prognostic factors were identified but were measured inconsistently. The most commonly assessed prognostic factors were related to pain and function (n = 10 studies), imaging features (n = 8 studies), patient socio-demographics (n = 7 studies), health and lifestyle (n = 6 studies), clinical assessment findings (n = 4 studies) and injection level (n = 4 studies). No prognostic factor was found to be consistently associated with outcomes following ESI. Most studies found no association or results that conflicted with other studies.
Conclusions
There is little, and low quality, evidence to guide practice in terms of factors that predict outcomes in patients following ESI for disc-related sciatica. The results can help inform some of the decisions about potential prognostic factors that should be assessed in future well-designed prospective cohort studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Sciatica is a common variation of low back pain, presenting as sharp, shooting pain in the leg, often with numbness and muscle weakness [1]. In most cases (90%) [1] sciatica is caused by a lumbar disc herniation compressing the lumbar spinal nerve root(s), with associated inflammation [2]. Many patients improve but around 30% continue to suffer from pain and related disability after one year [3]. Guidelines recommend epidural steroid injections (ESI) for treating severe disc-related sciatica pain based on trial data that shows modest benefits in terms of pain reduction and avoidance of surgery [4, 5]. ESIs can be performed in a number of ways (caudal, interlaminar and transforaminal approaches), and with or without imaging to verify delivery of the injectile substance to the target level in the spine [6]. The term epidural steroid injection (ESI) is used throughout this paper to describe any type of spinal injection (including local anaesthetic and corticosteroid), used for disc-related sciatica for reducing leg pain.
There is considerable uncertainty about the effectiveness of ESI for sciatica. A recent Cochrane review update showing small, average, treatment effects raised questions about the value of ESIs [7], with similar findings in other reviews where very few studies detected clinically relevant effects, and the certainty of evidence was judged to be low [8, 9]. However, another recent review argued that these conclusions are flawed and their review which did not include active placebo (e.g. anaesthetic), showed strong evidence for the effectiveness of ESI for managing sciatica [10]. Clinical guidelines provide different recommendations; ESIs are recommended for those with severe sciatica in the UK [4] and Belgium [11], whereas they are not recommended in the Netherlands [12], ESIs are one of the most common interventional pain procedures in the USA [13]. In the UK National Health Service (NHS), the average cost for an ESI under image guidance is £711 [14] and on average 5.2% of patients receive three or more injections in a 12-month period (April 2015–March 2018). Around 9500 injections are repeated in under six months, with a total annual cost to the NHS of £6.7 m [15].
There appears to be wide variation in response to ESIs, with some patients improving to such a degree that spinal surgery is avoided whilst others do not improve [4, 7,8,9,10]. Little is known about which factors are associated with outcome from ESIs; patient characteristics, clinical assessment findings, imaging findings or other test results. Only one systematic review of prognostic factors associated with treatment outcomes for sciatica, limited to imaging and laboratory markers, concluded that nerve root compression grading on MRI (magnetic resonance imaging) scan and elevated inflammatory markers were promising predictors of outcome [16].
With the need to reduce low value healthcare [17] it would be helpful to be able to better identify patients who have a reasonable chance of benefiting from ESI. This would prevent unnecessary burden on healthcare services and unnecessary healthcare costs. The objectives of this systematic review were to identify what factors, from those that are routinely collected in clinical practice, are potentially associated with good or poor outcome after an ESI for sciatica.
Methods
This review followed the PRISMA statement for reporting systematic reviews [18]. The protocol was registered on PROSPERO (CRD42020225777).
Eligibility criteria
Study eligibility criteria were guided by the PICOTS framework [19], covering population, index prognostic factor, comparator prognostic factors, outcomes, timing and setting/study design (Table 1). Included studies reported results for adults with a diagnosis of disc-related sciatica confirmed with MRI scan (or CT (Computerised Tomography) myelogram) of any duration who received an ESI for their sciatica symptoms. Studies were excluded if they did not present any information, statistical or narrative, on the strength of association between prognostic factors and outcome(s). We did not include laboratory markers as prognostic factors as they are not routinely collected as part of usual healthcare for sciatica patients.
Search strategy and Study selection
Four electronic databases were searched (MEDLINE, EMBASE, CINAHL Plus, PsycINFO) from inception to November 2020. An updated search was carried out in February 2022. Reference lists of included full text studies were searched. The search strategy used subject headings and free text searching, combining terms for prognosis, epidural steroid injection and sciatica. The Medline search strategy is presented in Table 2.
The results of all searches were downloaded into EndNote X9 (available at https://endnote.com/) to remove duplicates. The remaining studies were transferred to an excel spreadsheet for initial title and abstract screening, aided by an eligibility criteria checklist (Table 3).
All titles and abstracts were screened independently by two authors (AN & SS). Any disagreement was resolved through discussion. Full texts were independently screened by two authors (AN and SS) with a third reviewer (KS or KK) being consulted in the case of disagreements.
Data extraction
One reviewer extracted data for all the studies (AN) which was thoroughly checked by a second reviewer (SS). Data extraction was guided by CHARMS-PF, a modification of the checklist for critical appraisal and data extraction for systematic reviews of prediction modelling studies that can be used for prognostic factors [19]. Prognostic factors identified were grouped into domains of patient socio-demographics, health and lifestyle, medication, work, onset of sciatica, pain and function (disability), psychological measures, clinical assessment findings, MRI scan findings, EMG (Electromyography) study findings, QST (Quantitative Sensory Testing) and level and number of injections.
Risk of bias
The Quality in Prognostic Studies (QUIPS) tool [20] was used by two authors independently (AN and SS) to assess the risk of bias for each study. It consists of six potential bias domains: study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, statistical analysis and reporting. Domains were rated as low, moderate or high [20]. If there was uncertainly or in the event a domain was considered not appropriate it was rated as unsure. Overall risk of bias classification was rated low, moderate or high risk. To achieve low overall risk of bias, each domain must score low in all the 6 domains.
Synthesis of results
Results extracted from studies, included unadjusted (or crude) and adjusted estimates of the association of the prognostic factor with the outcome and corresponding standard errors or confidence intervals (e.g. odds ratio) for each prognostic factor of interest [19]. Where possible, reporting of adjusted prognostic associations (from multivariable analyses), including odds ratios, and 95% confidence intervals and p values were stated. Study heterogeneity precluded statistical pooling of results. Therefore a narrative synthesis was developed to provide an overview of the evidence for each prognostic factor.
A guide to systematic review and meta-analysis of prognostic factor studies [19] was used as a guide to conduct the review and REMARK (reporting recommendations for tumour marker prognostic studies) [21] was used to guide the review reporting.
Results
Study selection
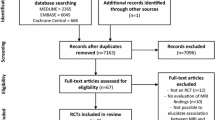
The search yielded 2726 citations after duplicates were removed. Following screening of titles and abstracts, the full texts of 130 studies were retrieved that satisfied the eligibility criteria outlined in Table 3. Studies unrelated to the topic of interest or not meeting the eligibility criteria were excluded. If after reading title and abstract the eligibility was unclear, full texts were retrieved and assessed. The updated search on 3rd February 2022 identified 368 additional titles and abstracts for screening. Four studies fulfilled the inclusion criteria therefore a total of 15 studies were included in the review (see the flowchart in Fig. 1).

PRISMA flow diagram showing identification and selection of included studies
Included studies
Fifteen studies, published between 1998 and 2021 (1606 participants) provided information about potential prognostic factors for patients with disc-related sciatica who had an ESI for their symptoms [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] (see Table 4 for summary of included studies). Study designs included prospective (n = 6 studies) and retrospective (n = 6) longitudinal cohorts, RCTs (n = 1), retrospective review of data from a previously published RCT (n = 1) and data from an unpublished prospective cohort study (n = 1). The sample size of included studies ranged from 17 to 390 with a median of 73 participants.
Study characteristics
Three studies included mixed populations of sciatica attributed to disc herniation or stenosis [22, 24, 27] but were included because they analysed results of diagnostic subgroups. All studies indicated concordance between clinical findings of nerve root pain/ radicular pain and imaging (MRI or CT) findings. It was less clear from most of the studies whether the clinically identified nerve root was the same as that reported on imaging.
Participants’ age ranged from 17 to 88 years and female participants within studies ranged from 30 to 74%. The ESI routes of delivery were transforaminal (n = 7), interlaminar (n = 2) and caudal (n = 2). One study included all three approaches [22]. Another two studies [26, 31] performed a selective nerve root block (SNRB), which is technically similar to a transforaminal ESI. The remaining study [25] did not clearly report the route of delivery. Fluoroscopic guidance (with contrast dye) was used in 11 studies (including all transforaminal ESI and SNRB studies and one interlaminar ESI study), ultrasound guidance was used for the caudal ESI [33, 35] and two studies did not use image guidance [24, 25]. Injectate solutions varied among the included studies, with differing use of corticosteroids (methylprednisolone acetate (n = 7), triamcinolone acetonide (n = 7) and dexamethasone (n = 1)) and different local anaesthetic (bupivacaine (n = 8), lidocaine (n = 5), ropivacaine (n = 1). One study, which did not report the ESI route of delivery, did not use anaesthetic and reported a total volume used of 7 ml [25]. The total injectate volumes varied between ESI routes of delivery. Transforaminal ESI and SNRB ranged from 1.5 to 4 ml, interlaminar ESI ranged from 3 to 9 ml and caudal ESI from 8 to 30 ml. One study did not report total volume used [26].
Characteristics of the individual studies are summarised in Table 4. Studies are grouped consistently in all tables according to the domains of the prognostic factor.
Prognostic factors
A total of 42 different prognostic factors were identified across the 15 studies (Table 5). The most assessed prognostic factors were related to pain and function (n = 10 studies each), imaging features (n = 8 studies), patient socio-demographics (n = 7 studies), health and lifestyle (n = 6 studies), clinical assessment findings (n = 4 studies) and injection level (n = 4 studies). Six of the 15 studies [23, 24, 26, 33, 34, 36] provided univariate/unadjusted analyses only.
Risk of bias
Nine of the 15 studies were judged as overall high risk of bias (RoB) and six studies were judged moderate RoB (Table 6 and Fig. 2). All high RoB studies had at least one domain judged as high RoB and the remaining domains were predominately moderate RoB. No study achieved low overall RoB, which required low risk ratings in all six domains [20]. In the individual domains of the QUIPS tool, low risk was most prevalent in the domain “outcome measurement”.

QUIPS Risk of Bias summary: Review authors’ judgement about each risk of bias domain presented as percentages across all included studies (n − 15)
Patient factors: demographics, health and lifestyle, medication, work and psychosocial factors
Seven studies investigated age [22, 24, 29, 31,32,33, 35] and six investigated gender [24, 29, 31,32,33, 35] but none found a statistically significant association with pain or disability outcomes following ESI. None of the health and lifestyle factors including body mass index (BMI) [29, 31, 35], smoking status [22, 31], type of previous surgery [24, 28] or comorbidities [31] showed a statistically significant association with pain or medication use outcomes. Three studies considered work-related characteristics [22, 28, 31]. White-collared office work [31] and increased physical demands of the job [28] were associated with poor outcomes in univariable analyses but neither remained significant in multivariable analyses. Secondary gain [22, 28] and history of an inciting event (e.g. lifting) [22, 31] were not found to be associated with outcome. Two studies using unadjusted analyses found higher levels of baseline depression to be associated with poorer outcomes of pain and the need for subsequent surgery [23, 26]. Medication use was investigated in two studies, neither found any association with pain reduction or changes in medication use after ESI [22, 28].
Sciatica related factors: onset of sciatica, pain and function
Of the two studies that investigated factors related to the onset of sciatica, no statistically significant association with pain outcomes were found for an inciting event [22, 31] or a previous sciatica episode versus a first episode [31]. For pain related factors, eight studies investigated pain duration [22, 24, 29,30,31,32,33, 35] and only one showed that pain duration less than 6 months was associated with better pain outcomes [35]. Only one [22] of seven studies [22, 24, 27,28,29, 31, 35] showed an association between higher baseline leg pain and a poorer pain outcome. Co-existing back pain [31], location of pain (calf, entire leg, thigh, gluteal) [31], bilateral sciatica [22] and side of sciatica (right or left) [31] showed no association with pain outcomes.
In unadjusted analysis, a study with 36 participants showed that pain not increased by walking was associated with poorer outcomes and pain that increased during coughing was associated with better outcomes (reduced pain) [24]. One [31] of the three studies [28, 31, 35] that investigated baseline disability scores, found higher baseline Oswestry Disability Index score was associated with minimal or no pain relief after ESI, but no multivariable analysis was carried out.
Clinical assessment findings
Four studies considered findings from the clinical assessment [24, 30, 31, 35]; lumbar flexion [35], straight leg raise test [24, 31, 35], and sensory, motor or reflex deficit [30, 31]. The only statistically significant association with poor pain outcomes, found in one study, was sensory deficit with pain relief (study did not report how pain was measured) in univariable analysis but it did not remain significant in multivariable analysis [31].
Investigation findings: MRI scans, EMG and QST
Eight studies considered various MRI scan findings as prognostic factors [29,30,31,32,33,34,35,36]. Following multivariable analysis, low-grade nerve root compression was associated with better pain outcomes in two studies [30, 32], the presence of a lumbosacral transitional segment was associated with poorer outcomes [31] and the location of disc herniation either centrally [32] or non-foraminal [35], was associated with better pain outcomes.
EMG findings were considered in two studies [27, 28]. In univariable analysis both showed an association between EMG evidence of sciatica and improved outcomes which remained significant in one of the two studies when adjusted for other baseline variables [27]. One small study considered QST, a test to measure mechanical and thermal sensations [25]. In adjusted analysis, greater dysfunction of Aδ-fibres (cold sensation) was associated with better pain outcomes and dysfunction of Aβ-fibres (vibration/touch) was associated with poorer outcomes (Table 7).
Injection factors
Of the three studies that considered the level the ESI was delivered (e.g. L5/S1) [29, 32, 35], one found that a target level other than between L2 and L4 was associated with better pain outcomes [35]. One study comparing multilevel injections (two or more) with single-level injections found a 7.5-fold increase in the odds of a better pain outcome favouring multilevel injections [22].
Discussion
This is the first systematic review to synthesise the literature investigating factors that can be routinely collected in clinical practice, as prognostic factors associated with outcomes following ESI for patients with disc-related sciatica. The review found 15 eligible studies, which explored 42 potential prognostic factors assessed before the ESI. Our review showed that no prognostic factor is consistently associated with patient outcomes, most studies found no association or conflicting results. Overall study quality was low with all judged to have moderate or high risk of bias and between-study heterogeneity precluded statistical pooling of results. Considering the frequent use of ESIs in clinical practice, the search results are surprising. It was anticipated that there would be more high-quality prognosis studies of this nature.
The most commonly assessed prognostic factors were patient demographics, health and lifestyle factors, leg pain related factors and MRI scan findings but even these were only included in, at most, six to eight of the studies. All but one of the studies used a measure of pain as a primary outcome but a variety of methods of measuring and defining a good or poor outcome was evident across studies.
Comparison of results to similar studies
To our knowledge, one systematic review has been published on prognostic factors associated with treatment outcomes for sciatica [16] but it only focused on imaging factors and laboratory inflammatory biomarkers. That review searched only one database and identified eight eligible studies with mixed populations (disc herniation and spinal stenosis) and ESIs for lumbar and cervical spine which makes it difficult to compare our results. For MRI imaging, the review concluded that nerve root compression grading, based on two studies, can predict short-term pain reduction after ESI. Our review, which included these two studies and four additional studies showed inconsistent results for grades of nerve root compression and their association with outcome. The review suggested elevated inflammatory biomarkers (obtained from simple blood tests or material harvested during the injection) seemed promising to predict outcomes. The evidence of the role of biomarkers in sciatica is not convincing [40]. Biomarkers were not included in this review as potential prognostic factors to inform a future prospective cohort study data collection as those specific to ESI are costly to perform and analyse and not routinely collected in clinical practice.
In the absence of similar reviews of ESIs for disc-related sciatica, we compared findings to reviews of prognostic factors in sciatica treatment outcomes. A review of factors associated with recovery following lumbar discectomy surgery for sciatica reported higher severity of pre-operative leg pain predicted better outcomes (reduced leg pain) at 2 and 7 years [41]. The review showed very low-level evidence that a lower pre-operative measure of health-related quality of life (measured by the EQ-5D) predicted better health-related quality of life at 2 years. There was low-level evidence to support duration of leg pain pre-operatively not being associated with outcome, and very low-quality evidence that supported other factors of pre-operative disability, duration and severity of back pain, ipsilateral SLR and forward bend not being associated with outcome. For non-surgically treated sciatica patients, there was positive association with strong evidence for leg pain intensity at baseline as a prognostic factor for subsequent surgery [42]. Overall, there is a lack of clear and consistent factors predicting outcomes in patients with sciatica [42,40,44] that has made it challenging to design prognostic models to guide treatment decision-making. A stratified care model developed for sciatica patients based on prognosis and factors associated with referral to spinal specialists was not superior to non-stratified usual care [45]. The authors of that trial recommended further research to identify factors associated with outcomes to help develop better predictive models for use in clinical decision-making.
Strengths and limitations of the review
The inclusion of a broad range of potential prognostic factors, treatment outcomes and study designs, consisting of RCTs, retrospective and prospective cohorts, strengthens the completeness of this review. But it could be argued that a more robust streamlined review was possible if only prospective study designs has been included, which are considered optimum for prognostic factor research [19, 46] and if we limited our eligibility criteria to a minimum sample of 100 participants as other prognostic factor systematic reviews have done [47]. Only four studies in the review used a prospective design and 10 of the 15 studies had a sample size with outcome follow-up data of less than 100 participants. It was anticipated that more high-quality prognosis studies would have been identified considering the popular use of ESIs. This raises the potential of publication bias and selective reporting which is common in prognosis research [19].
Limitations of the review include the moderate to high risk of bias across the available studies. Therefore the conclusion of the review showing that no prognostic factor was consistently associated with patient outcome, may be in part due to the overall poor quality of the studies. Non-English studies were not included in the search strategy therefore potentially relevant studies may have been missed. The definition and diagnosis of sciatica was ambiguous in two of the included studies. It is possible therefore that not all subjects had disc-related sciatica. The diverse measured time-points and outcome measures used, ranging from pain outcomes (with differing definitions of what resulted in treatment success and failure), inconsistent disability outcomes and complex composite measures of pain severity and medication use, may also contribute to conflicting results. The review identified only four papers that focused on injection related factors as potential prognostic factors, three looked at the level of injection and one on multilevel injections versus single level. Other factors such as the injection approach, the type and dose of medication used were not considered in any of the papers we reviewed. This reflects current clinical practice where multiple types of ESI are performed, delivered through transforaminal, interlaminar or caudal approaches with varying steroid and anaesthetic types and dosages.
To consider injection related factors as potential prognostic factors would require a large cohort study, likely multicentre in nature to capture different practices and have enough numbers with different types of injections that could be used in the prognostic factor analysis. Alternatively, an individual participant data analysis would be needed, combining data and outcomes from existing trials and cohort studies to test injection factors as potential prognostic factors.
Conclusions and next steps
This systematic review highlights the continued uncertainty about prognostic factors in patients having ESI for sciatica. There is a clear need for a suitably powered, low risk of bias, prospective cohort to more carefully investigate factors that predict outcome following ESI. The results of this systematic review can help to inform at least some of the decisions about the predictors assessed in such a future cohort study. The variations in outcomes used across studies also highlights that there should be international agreement on the definition of treatment success that can be used consistently in future cohort studies and trials of ESIs.
References
Jensen RK, Kongsted A, Kjaer P, Koes B (2019) Diagnosis and treatment of sciatica. BMJ 367:l6273. https://doi.org/10.1136/bmj.l6273
Stafford MA, Peng P, Hill DA (2007) Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. Br J Anaesth 99(4):461–473. https://doi.org/10.1093/bja/aem238
Lequin MB, Verbaan D, Jacobs WC, Brand R, Bouma GJ, Vandertop WP, Peul WC et al (2013) Surgery versus prolonged conservative treatment for sciatica: 5-year results of a randomised controlled trial. BMJ Open 3(5):e002534. https://doi.org/10.1136/bmjopen-2012-002534
National Institute for Health and Care Excellence (2016) Low back pain and sciatica in over 16s: assessment and management. Manchester: National Institute for Health and Care Excellence. (NG59). Available: https://www.nice.org.uk/guidance/ng59/chapter/Recommendations
National Institute for Health and Care Excellence (2017) National Low Back and Radicular Pain Pathway. Including Implementation of NICE Guidance NG59
Lee J, Gupta S, Price C, Baranowski AP, British Pain Society (2013) Low back and radicular pain: a pathway for care developed by the British Pain Society. Br J Anaesth 111(1):112–20. https://doi.org/10.1093/bja/aet172
Oliveira CB, Maher CG, Ferreira ML, Hancock MJ, Oliveira VC, McLachlan AJ, Koes BW, Ferreira PH, Cohen SP, Pinto RZ (2020) Epidural corticosteroid injections for sciatica: an abridged Cochrane systematic review and meta-analysis. Spine (Phila Pa 1976) 45(21):E1405–E1415. https://doi.org/10.1097/BRS.0000000000003651
de Bruijn TM, de Groot IB, Miedema HS, Haumann J, Ostelo RWJG (2021) Clinical relevance of epidural steroid injections on lumbosacral radicular syndrome-related synptoms: systematic review and meta-analysis. Clin J Pain 37(7):524–537. https://doi.org/10.1097/AJP.0000000000000943
Verheijen EJA, Bonke CA, Amorij EMJ, Vleggeert-Lankamp CLA (2021) Epidural steroid compared to placebo injection in sciatica: a systematic review and meta-analysis. Eur Spine J 30(11):3255–3264. https://doi.org/10.1007/s00586-021-06854-9
Manchikanti L, Knezevic E, Knezevic NN, Sanapati MR, Thota S, Abd-Elsayed A, Hirsch JA (2021) Epidural Injections for lumbar radiculopathy or sciatica: a comparative systematic review and meta-analysis of Cochrane review. Pain Physician 24(5):E539–E554
Jonckheer P, Desomer A, Depreitere B, Berquin A, Bruneau M, Christiaens W, Coeckelberghs E et al (2017) Low back pain and radicular pain: development of a clinical pathway—Supplement. Health Services Research (HSR) Brussels: Belgian Health Care Knowledge Centre (KCE). KCE Reports 295. D/2017/10.273/88
Verburg AF, Schaafstra A, Spinnewijn WE, Kroes BW, Bouma M, Burgers JS. Herziene NHG-standaard (2015) 'Lumbosacraal radiculair syndroom' [Revised NHG practice guideline 'Lumbosacral radicular syndrome']. Ned Tijdschr Geneeskd. 159:A9122. Dutch. PMID: 26246062
Manchikanti L, Pampati V, Soin A, Sanapati MR, Kaye AD, Hirsch JA (2021) Declining utilization and inflation-adjusted expenditures for epidural procedures in chronic spinal pain in the Medicare population. Pain Physician 24(1):1–15
Wilby MJ, Best A, Wood E, Burnside G, Bedson E, Short H, Wheatley D et al (2021) Microdiscectomy compared with transforaminal epidural steroid injection for persistent radicular pain caused by prolapsed intervertebral disc: the NERVES RCT. Health Technol Assess 25(24):1–86. https://doi.org/10.3310/hta25240
https://gettingitrightfirsttime.co.uk/wp-content/uploads/2019/01/Spinal-Services-Report-Mar19-L1.pdf
Benny BV, Patel MY (2014) Predicting epidural steroid injections with laboratory markers and imaging techniques. Spine J 14:2500–2508. https://doi.org/10.1016/j.spinee.2014.04.003
Foster NE, Anema JR, Cherkin D et al (2018) Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet 391(10137):2368–2383. https://doi.org/10.1016/S0140-6736(18)30489-6
Page MJ, McKenzie JE, Bossuyt PM et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Riley RD, Moons KGM, Snell KIE et al (2019) A guide to systematic review and meta-analysis of prognostic factor studies. BMJ 364:k4597. https://doi.org/10.1136/bmj.k4597
Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C (2013) Assessing bias in studies of prognostic factors. Ann Intern Med 158(4):280–286. https://doi.org/10.7326/0003-4819-158-4-201302190-00009
Sauerbrei W, Taube SE, McShane LM, Cavenagh MM, Altman DG (2018) Reporting recommendations for tumor marker prognostic studies (REMARK): an abridged explanation and elaboration. J Natl Cancer Inst 110(8):803–811. https://doi.org/10.1093/jnci/djy088
Engle AM, Chen Y, Marascalchi B et al (2019) Lumbosacral radiculopathy: inciting events and their association with epidural steroid injection outcomes. Pain Med 20(12):2360–2370. https://doi.org/10.1093/pm/pnz097
Bahar-Ozdemir Y, Sencan S, Ercalik T, Kokar S, Gunduz OH (2020) The effect of pre-treatment depression, anxiety and somatization levels on transforaminal epidural steroid injection: a prospective observational study. Pain Physician 23(3):E273–E280
Rivest C, Katz JN, Ferrante FM, Jamison RN (1998) Effects of epidural steroid injection on pain due to lumbar spinal stenosis or herniated disks: a prospective study. Arthritis Care Res 11(4):291–297. https://doi.org/10.1002/art.1790110410
Schiff E, Eisenberg E (2003) Can quantitative sensory testing predict the outcome of epidural steroid injections in sciatica? A preliminary study. Anesth Analg 97(3):828–832. https://doi.org/10.1213/01.ANE.0000078583.47735.69
Shaikh H, Kumar A, Kishen TJ (2021) Temporal pattern of pain and disability following the administration of a selective nerve root block in lumbar disc herniation with radiculopathy. Int J Spine Surg 15(6):1090–1095. https://doi.org/10.14444/8195
Batistaki C, Angelopoulou A, Smyrnioti ME, Kitsou MC, Kostopanagiotou G (2017) Electromyographic findings after epidural steroid injections in patients with radicular low back pain: a prospective open-label study. Anesth Pain Med 7(6):e62556. https://doi.org/10.5812/aapm.62556
Tong HC, Williams JC, Haig AJ, Geisser ME, Chiodo A (2003) Predicting outcomes of transforaminal epidural injections for sciatica. Spine J 3(6):430–434. https://doi.org/10.1016/s1529-9430(03)00179-7
Şencan S, Çelenlioğlu AE, Asadov R, Gündüz OH (2020) Predictive factors for treatment success of transforaminal epidural steroid injection in lumbar disc herniation-induced sciatica. Turk J Med Sci 50(1):126–131. https://doi.org/10.3906/sag-1908-167
Ghahreman A, Bogduk N (2011) Predictors of a favorable response to transforaminal injection of steroids in patients with lumbar radicular pain due to disc herniation. Pain Med 12(6):871–879. https://doi.org/10.1111/j.1526-4637.2011.01116.x
Kanna RM, Shetty AP, Rajasekaran S (2019) Predictors of successful outcomes of selective nerve root blocks for acute lumbar disc herniation. Glob Spine J 9(5):473–479. https://doi.org/10.1177/2192568218800050
Choi SJ, Song JS, Kim C, Shin MJ, Ryu DS, Ahn JH, Jung SM, Park MS (2007) The use of magnetic resonance imaging to predict the clinical outcome of non-surgical treatment for lumbar intervertebral disc herniation. Korean J Radiol 8(2):156–163. https://doi.org/10.3348/kjr.2007.8.2.156
Cha SO, Jang CH, Hong JO, Park JS, Park JH (2014) Use of magnetic resonance imaging to identify outcome predictors of caudal epidural steroid injections for lower lumbar radicular pain caused by a herniated disc. Ann Rehabil Med 38(6):791–798. https://doi.org/10.5535/arm.2014.38.6.791
Paidin M, Hansen P, McFadden M, Kendall R (2011) Contrast dispersal patterns as a predictor of clinical outcome with transforaminal epidural steroid injection for lumbar radiculopathy. PMR 3(11):1022–1027. https://doi.org/10.1016/j.pmrj.2011.07.020
Elashmawy MA, Shaat RM, Abdelkhalek AM et al (2020) Caudal epidural steroid injection ultrasound-guided versus fluoroscopy-guided in treatment of refractory lumbar disc prolapse with radiculopathy. Egypt J Radiol Nucl Med 51:259. https://doi.org/10.1186/s43055-020-00388-8
Kwak S, Jang SH, Chang MC (2021) Long-term outcomes of transforaminal epidural steroid injection in patients with lumbosacral radicular pain according to the location, type, and size of herniated lumbar disc. Pain Pract 21(8):836–842. https://doi.org/10.1111/papr.13029
Pfirrmann C, Dora C, Schmid M, Zanelli M, Hodler J, Boos N (2004) MR image–based grading of lumbar nerve root compromise due to disk herniation: reliability study with surgical correlation. Radiology 230:583–588
Lee S, Lee J, Yeom J, Kim K-J, Kim H-J, Chung S, Kang H (2010) A practical MRI grading system for lumbar foraminal stenosis. Am J Roentgenology 194:1095–1098
Fardon D, Milette P (2001) Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine 26:E93–113
Jungen MJ, ter Meulen BC, van Osch T et al (2019) Inflammatory biomarkers in patients with sciatica: a systematic review. BMC Musculoskelet Disord 20:156. https://doi.org/10.1186/s12891-019-2541-0
Rushton A, Zoulas K, Powell A, Staal JB (2018) Physical prognostic factors predicting outcome following lumbar discectomy surgery: systematic review and narrative synthesis. BMC Musculoskelet Disord 19(1):326. https://doi.org/10.1186/s12891-018-2240-2
Verwoerd AJ, Luijsterburg PA, Lin CW, Jacobs WC, Koes BW, Verhagen AP (2013) Systematic review of prognostic factors predicting outcome in non-surgically treated patients with sciatica. Eur J Pain 17(8):1126–1137. https://doi.org/10.1002/j.1532-2149.2013.00301.x
Ashworth J, Konstantinou K, Dunn KM (2011) Prognostic factors in non-surgically treated sciatica: a systematic review. BMC Musculoskelet Disord 12:208. https://doi.org/10.1186/1471-2474-12-208
Konstantinou K, Dunn KM, Ogollah R et al (2018) Prognosis of sciatica and back-related leg pain in primary care: the ATLAS cohort. Spine J 18(6):1030–1040. https://doi.org/10.1016/j.spinee.2017.10.071
Konstantinou K, Lewis M, Dunn KM, Ogollah R, Artus M, Hill JC, Hughes G, Robinson M, Saunders B, Bartlam B, Kigozi J, Jowett S, Mallen CD, Hay EM, van der Windt DA, Foster NE (2020) Stratified care versus usual care for management of patients presenting with sciatica in primary care (SCOPiC): a randomised controlled trial. Lancet Rheumatol 2(7):e401–e411. https://doi.org/10.1016/S2665-9913(20)30099-0
Moons KG, Royston P, Vergouwe Y, Grobbee DE, Altman DG (2009) Prognosis and prognostic research: what, why, and how? BMJ 338:b375. https://doi.org/10.1136/bmj.b375
Wertli MM, Rasmussen-Barr E, Weiser S, Bachmann LM, Brunner F (2014) The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: a systematic review [published correction appears in Spine J 14(8):a18]. Spine J 14(5):816–36.e4. https://doi.org/10.1016/j.spinee.2013.09.036
Acknowledgements
We wish to thank Dr Nadia Corp who assisted with the search strategy
Funding
This study is supported by Health Education England and the National Institute for Health and Care Research (HEE/NIHR ICA Programme Clinical Lectureship, Dr Siobhan Stynes, NIHR300441). The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nagington, A., Foster, N.E., Snell, K. et al. Prognostic factors associated with outcome following an epidural steroid injection for disc-related sciatica: a systematic review and narrative synthesis. Eur Spine J 32, 1029–1053 (2023). https://doi.org/10.1007/s00586-023-07528-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07528-4