
Abstract
Purpose
To describe health-related quality of life in adolescents with idiopathic scoliosis and controls.
Methods
This cross-sectional study analysed data from 307 individuals with idiopathic scoliosis and 80 controls without scoliosis (mean age 15.5 ± 2.1 and 14.0 ± 2.2 years, respectively). Health-related quality of life (HRQoL) was assessed using EuroQol 5-dimensions (EQ-5D) questionnaire, and the scoliosis specific Scoliosis Research Society-22r questionnaire (SRS-22r). HRQoL data in individuals with scoliosis were compared to controls, between treatment groups (untreated, ongoing brace, previously braced and surgically treated) and stratified according to curve size.
Results
Adolescents with idiopathic scoliosis had reduced HRQoL compared with controls, observed through lower SRS-22r subscore (respective means 4.16 and 4.68, p < 0.001) and lower EQ-5D index (respective means 0.92 and 0.95, p = 0.032).
No differences in SRS-22r subscore or EQ-5D index were detected when comparing different scoliosis treatment groups. Within the SRS-22r function domain the surgically treated group scored 4.40, significantly lower compared to the untreated (4.65) and ongoing brace groups (4.68, p = 0.005). The surgically treated and untreated group were more affected by pain, compared to the ongoing brace group (p = 0.01) with the surgically treated group scoring lowest. Non-surgically treated scoliosis individuals with larger curves (> 30 degrees) had a lower SRS-22r subscore (4.08) compared to those with smaller curves (4.31, p = 0.001).
Conclusion
Adolescents with idiopathic scoliosis had a reduced HRQoL compared to healthy controls. Minor differences were detected when comparing between idiopathic scoliosis treatment groups. Non-surgically treated scoliosis patients with larger curves had a lower HRQoL shown by lower SRS-22r values.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Idiopathic scoliosis is a three-dimensional torsional deformity of the spine affecting otherwise healthy individuals and often detected during rapid periods of growth [1]. Over the past few decades, a paradigm shift has occurred in understanding health and disability with increased emphasis on health-related quality of life (HRQoL) measures and understanding disability with regard to functioning after health changes. The impact of scoliosis on quality of life is therefore well documented and may affect psychological well-being through concerns for physical appearance, pain, lower self-esteem, uncertain prognosis, and concerns over peer interactions [2,3,4]. It has been argued that treatment modalities, such as bracing, may further affect HRQoL negatively and in a previous adolescent cohort study, individuals who were undergoing or previously received brace treatment had impaired HRQoL, as estimated with the disease-specific Scoliosis Research Society-22r (SRS-22r) and generic EuroQol 5-Dimensions index (EQ-5D), compared to untreated individuals [5]. The evidence however is conflicting, and not all studies have supported the theory that bracing may be detrimental to HRQoL scores in adolescents undergoing brace treatment [6, 7].
Avoiding long-term compromise to HRQoL is an indication for treatment and therefore of relevance in future research. Surgically treated individuals have been shown to have improved HRQoL, pain, satisfaction, and self-image scores, compared to brace treated individuals [8,9,10]. This is, however, with questionable clinical significance [11] and long-term follow-up has illustrated lower scores in function and self-image domains within the SRS-22r compared to brace treated or untreated individuals [12].
The aim of the current study was to further delineate health-related quality of life in adolescents treated or observed for idiopathic scoliosis, as well as making comparisons with a group of healthy controls.
Methods
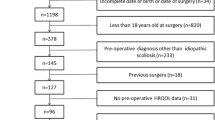
Individuals with idiopathic scoliosis who were formerly or currently treated or observed at one of five Swedish Orthopaedic Departments (Karolinska University Hospital, Sahlgrenska University Hospital, Skåne University Hospital, Linköping University Hospital and Sundsvall and Härnösand County Hospital) were invited to participate in this study from September 2010 until October 2018. Individuals were included if they had a diagnosis of Idiopathic Scoliosis on standing radiographs with a curve in the frontal plane of at least 10 degrees, measured according to the methods described by Cobb [13], were between 10 and 18 years of age and were able to understand and read the Swedish language. Individuals were excluded if they had signs or symptoms associated with scoliosis of non-idiopathic origin. In total, 307 individuals with Idiopathic Scoliosis with a mean age (standard deviation) of 15.5 (2.1) years met the inclusion criteria were included in this ongoing study which had the primary purpose to study genetics of idiopathic scoliosis [14, 15]. Figure 1 shows the inclusion process. Of the individuals with Idiopathic Scoliosis, 111 individuals were untreated, 64 individuals had ongoing brace treatment, 47 individuals had previously been braced and 85 individuals were surgically treated. The untreated patient group comprised of individuals who had not reached the Cobb threshold of 25° indicated for brace treatment, individuals who had reached skeletal maturity, those who had declined brace treatment, as well as individuals who were being planned for surgery. The ongoing brace group had been undergoing treatment for a mean time of 1.3 ± 1.6 years and the previously braced group had, on average, ceased wearing the brace 1.8 ± 1.6 years previously. Bracing was recommended to adolescents with curves ranging from 25 to 40 degrees, where further skeletal growth was expected, as suggested by the Scoliosis Research Society [16]. A full-time rigid thoracosacral (TLSO) orthosis was utilised by 38 individuals in the ongoing brace group, and 41 individuals in the previously braced group. Hyperextension night-time brace was utilised by 26 individuals in the ongoing brace group (41.3%) and 6 individuals in the previously braced group (12.8%). Individuals wearing a full-time brace were encouraged to wear the brace for 20 h a day and for those with a night-time brace 8–10 h. Surgical treatment was recommended in larger curves (usually 45° or above), if progression was expected. Time after surgery for this group of 85 individuals was a mean of 1.7 ± 1.7 years. Controls without scoliosis were selected from a previous study investigating normative data for SRS-22r and EQ-5D as described earlier [17]. In total, 80 individuals within the same age category as the adolescents with scoliosis at a mean age of 14.0 (2.2) were included in this study.

Flowchart of the individuals with idiopathic scoliosis in the study
Health-related quality of life questionnaires
All participants answered the SRS-22r and EQ-5D questionnaires. The SRS-22r consists of 22 questions distributed over five domains: function, pain, self-image, mental health and satisfaction, and has been translated into Swedish [18]. The domain scores range from 1 (worst) to 5 (best). An index for each domain has been derived as well as a total index for all the domains. The satisfaction question cannot be answered by those not being treated for scoliosis or controls and for that reason, the subscore has been used, which is a total score average of all valued SRS-22r items excluding the satisfaction domain.
EQ-5D 3-level version is one of the most widely used generic instruments for measuring HRQoL [19]. Individuals assess their health in five dimensions including mobility, self-care, usual activities, pain/discomfort and anxiety/depression. For each dimension 1 of 3 options is possible to choose and reflects the responders ability to manage each dimension [20]. An index will be obtained using the Swedish tariff where the index values are between 0.34 (worst) and 0.97 (best) [19]. The EQ-5D has been validated for its use in the AIS population [21] and shown to have moderate to good correlation properties with SRS-22r [17].
Exercise participation
Exercise participation was measured subjectively by answering yes or no to the question; “Do you participate in any exercise or competitive sports?” The duration, intensity or exercise type was not taken into consideration for the purpose of this study.
Radiography
Curve size was assessed according to the Cobb measurement method [13] and was obtained from the radiograph available from the most recent clinical follow-up appointment previous to the date of questionnaire completion. Cobb angles mean (min–max) were for the subgroups as follows: untreated 30 (11–78) degrees, ongoing brace group 34 (21–57) degrees, previously braced group 35 (25–50) degrees, and for the surgically treated group 24 (5–44) degrees.
Statistical analysis
Data are presented as the mean, standard deviation and range or number and percentage. The Chi2 test was used for categorical data. Mann–Whitney U test and analysis of covariance (ANCOVA) were used for continuous data, with adjustments for age, sex, and exercise participation. Descriptive and demographic statistics between the four different scoliosis treatment groups were completed with analysis of variance (ANOVA) with post hoc analysis using Tamhanes test for BMI and curve size as equal variances could not be assumed according to Levenes test. Statistical analysis between these four groups was completed with ANCOVA with adjustments for age, sex, and body mass index (BMI).
For comparisons based on curve severity, individuals with ongoing or previous brace treatment as well as untreated individuals were stratified according to Cobb angles (≤ 30° or > 30°) as well as larger angles (< 45° or ≥ 45°). Surgically treated individuals were stratified according to lowest fusion level (L2 as most caudal vertebra or below). Statistical analyses were performed with ANOVA. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) statistical software for Windows (SPSS V26, IBM Corporation, New York, NY, USA).
Results
Health-related quality of life in adolescents with and without idiopathic scoliosis
Descriptive statistics for the entire scoliosis group compared to healthy controls are shown in Table 1. Group comparisons showed that the idiopathic scoliosis individuals were significantly older, contained a larger proportion of females and were less likely to be currently participating in exercise or sports compared to the healthy control group (p < 0.001, p = 0.023 and p = 0.014, respectively).
The scoliosis group had significantly lower scores compared with the individuals without scoliosis in the SRS-22r subscore (p < 0.001) as well as in the separate domains of function (p = 0.009), pain (p < 0.001) and self-image (p < 0.001), Table 2. The EQ-5D index showed similar findings with the individuals with Idiopathic Scoliosis scoring significantly lower (p = 0.032) compared to the healthy controls.
Comparisons between the different scoliosis treatment groups
Descriptive data are presented in Table 3. Significant differences were detected between the groups with regard to proportion of females, age, BMI and curve size (p = 0.005, p < 0.001, p = 0.012 and p < 0.001, respectively).
Comparisons between the four treatment scoliosis groups are presented in Table 4. There was no significant difference between the groups in SRS-22r subscore (p = 0.67). Post hoc analysis of the SRS-22r function domain showed significantly lower scores in the surgically treated group (4.40 ± 0.63) compared to the untreated (4.65 ± 0.40, p = 0.002) and ongoing brace groups (4.68 ± 0.39, p = 0.002). There were no differences in function scores between the remainder of the groups. In the SRS-22r pain domain, the surgically treated group had a significantly lower score (3.95 ± 0.90) compared to the ongoing brace group (4.46 ± 0.48, p = 0.003), and the untreated group also had a significantly lower score (4.17 ± 0.79) compared to the ongoing brace group (p = 0.03). There were no statistical differences between the groups in the domains of self-image (p = 0.35) and mental health (p = 0.51). There were no significant differences in EQ-5D index scores between the groups (p = 0.51).
When comparing the three scoliosis groups who received treatment, significantly higher treatment satisfaction scores were evident in the surgically treated group (4.03 ± 0.92) compared to both ongoing brace (3.73 ± 0.90) and previously braced (3.44 ± 0.81) groups (p = 0.001). No difference between these three groups was seen with regard to the total SRS-22r score with satisfaction taken into consideration.
Curve size characteristics
When stratifying the non-surgically treated scoliosis individuals by curve size (≤ 30° or > 30°), the group with larger curves (n = 112) had a lower SRS-22r subscore (4.08 ± 0.53) compared to those with smaller curves (n = 110, 4.31 ± 0.48, p = 0.001), which was mainly driven by differences in the SRS-22r domains function, pain, and self-image (p = 0.001, p = 0.006 and p < 0.001, respectively). The mean scores for the SRS-22r domains function, pain and self-image were, for the group with larger curves: 4.55 ± 0.43, 4.16 ± 0.78 and 3.66 ± 0.83, respectively, and for the group with smaller curves: 4.71 ± 0.39, 4.38 ± 0.63 and 4.10 ± 0.71, respectively. These results are illustrated in Fig. 2. No significant differences in EQ-5D index score were detected between the groups (p = 0.245).

SRS-22r: comparisons based on curve severity. Mean values are plotted
When stratifying the non-surgically treated scoliosis individuals by curve size (< 45º or ≥ 45°), those with larger curves (n = 30) had a lower SRS-22r subscore (3.91 ± 0.58) compared to those with smaller curves (n = 192, 4.24 ± 0.50, p = 0.002), as well as a lower EQ-5D subscore compared to those with larger curves (0.89 ± 0.08 and 0.93 ± 0.06, respectively, p = 0.006).
Surgical characteristics
There were no differences in EQ-5D score, SRS-22r subscore or SRS-22r subdomains when stratifying the surgical group by lowest fusion level (all p ≥ 0.28).
Discussion
This study found an overall reduced health-related quality of life in Swedish adolescents with idiopathic scoliosis compared with healthy controls, as estimated with the disease-specific SRS-22r and the generic EQ-5D. The difference in the SRS-22r was mainly driven by the separate domains of function, pain and self-image, the mental health domain did not differ between the groups.
In a previous study, Mariconda et al. 2016 detected reduced HRQoL pre-operatively in a cohort of adolescents with idiopathic scoliosis (n = 87) compared to age- and sex-matched healthy controls in physical domains of the SF-36 questionnaire as well as reduced SRS-23 scores within the self-image and pain domain [3], which is similar to the results in the current study.
When comparing between the scoliosis subgroups, no differences were detected with regard to HRQoL as demonstrated by EQ-5D or the SRS-22r subscore. In the separate SRS-22r domains, the surgically treated group had lower function and pain scores compared to the ongoing brace group as well as lower function scores compared to the untreated group, which is similar to that of previous studies [22, 23]. In contrast however, these studies also detected superior self-image scores in surgically treated individuals compared to conservatively treated individuals. In the study by Bunge et al. better self-image scores were only detected in surgically treated individuals without prior brace treatment, which may to some extent explain the disparity as the surgical group in the current study also includes 24 individuals (28%) previously treated with a brace.
In a large cohort (n = 652) of adolescents with scoliosis, Cheung et al. detected lower HRQoL scores in adolescents with ongoing and previous brace treatment compared to observed scoliosis adolescents [5]. HRQoL in this study was also estimated using SRS-22 and EQ-5D scores, but the results differed somewhat to the current study. Possible explanations for differences may be due to brace characteristics, time after brace cessation, differences in compliance or cultural differences.
The lower function and pain scores in the surgical group in this study may arguably be due to short-term follow-up (mean 1.7 years) following surgery. Diarbakerli et al. have, in a large cohort study, studied the effect of different scoliosis treatments during adolescence on HRQoL in adulthood [12]. In this study, surgically treated individuals had lower function scores, as well as lower SRS-22r subscore and self-image, compared to their conservatively treated peers. This would suggest that reduced function in surgically treated individuals compared to conservatively treated individuals, is not only temporary, but something that continues to extend into adult life. Those with a more caudal fusion level in Diarbakerli’s study also scored lower on EQ-5D index, SRS-22r subscore as well as subdomains of pain and function [12]. This differs from the results of the current study where no differences were detected, and it may be hypothesised that fusion level affects surgically treated individuals more long term, rather than during adolescence, due to degenerative processes affecting the spine.
Our results show that, despite reduction in function and an increase in pain, the surgical group was more satisfied with their treatment compared to both brace groups. This is in keeping with findings from other studies [12, 22, 23]. Satisfaction with management did not differ between the two brace groups. Possible explanations for improved satisfaction scores in the surgical group may be due to the direct improvement in curve size on the frontal radiograph following surgery and improvements in cosmetic appearance. Similarly to our findings, a previous study detected reduced function (measured using the SRS-24) at a 5-year follow-up in surgically treated scoliosis individuals compared to healthy controls [19]. However, pain, self-image and HRQoL in the surgically treated scoliosis individuals were superior to untreated scoliosis individuals and similar to that of healthy controls [19].
In the current study, an inferior HRQoL was detected in the group with larger curves, illustrated by lower SRS-22r subscore. This is in keeping with the study by Berliner et al. where adolescents (n = 286) with curves smaller than 40 degrees had a higher SRS-22r total score as well as superior scores in the subdomains of pain and self-image [24]. Differences in HRQoL in this study were mainly driven by differences in the SRS-22r domains function, pain, and self-image which is in keeping with previous research [24,25,26]. A large difference was seen within the self-image domain, which is supported by other studies which have shown good correlations between self-image and clinical and radiographic deformity [25, 27]. The current study showed differences in SRS-22r subscore when scoliosis individuals were stratified by curve size at both 30 and 45 degrees. Differences within the EQ-5D were, however, only detected with stratification above and below 45 degrees, indicating that this outcome measure may be less sensitive in detecting HRQoL changes within this population group.
Statistical differences between the adolescents with idiopathic scoliosis and the healthy control group showed that scoliosis individuals had a reduced SRS-22r subscore, more pain and worse self-image scores on SRS-22r which exceeded minimal clinically important difference (MCID) values previously published [28]. No differences in the SRS-22r domains between the scoliosis treatment groups or the curve severity groups reached a level of clinical significance. Previously published MCID values are based on individual changes pre- and post-operatively and not necessarily applicable to comparing data on group level.
To the best of our knowledge, this study is the first of its kind to compare so many different scoliosis treatment groups, including a surgical group, as well as a group of healthy adolescents. The internal validity is however, arguably, somewhat compromised since brace type (full-time or night-time) differs within the ongoing and previously braced groups. The cross-sectional design of this study limits results to descriptive findings as opposed to conclusions with regard to causality. The results from this study are thought to have sound generalisability should therefore be taken into consideration by clinicians, especially in comparison to healthy controls, and as a platform for further research in this field.
Conclusions
In conclusion, adolescents with Idiopathic Scoliosis had a lower health-related quality of life compared to healthy controls as measured by both scoliosis specific and generic outcome measures. Adolescents with idiopathic scoliosis are mostly concerned with pain and self-image. Surgically treated individuals were to a larger extent satisfied with their management, despite having decreased HRQoL otherwise, compared with brace treated individuals. Finally, larger curves were shown to be associated with overall decreased HRQoL.
References
Negrini S et al (2018) 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord 13:3. https://doi.org/10.1186/s13013-017-0145-8
Payne WK et al (1997) Does scoliosis have a psychological impact and does gender make a difference? Spine (Phila Pa 1976) 22(12):1380–1384
Mariconda M et al (2016) Effect of surgical correction of adolescent idiopathic scoliosis on the quality of life: a prospective study with a minimum 5-year follow-up. Eur Spine J 25(10):3331–3340. https://doi.org/10.1007/s00586-016-4510-8
Savvides P et al (2020) Self-experienced trunk appearance in individuals with and without idiopathic scoliosis. Spine (Phila Pa 1976) 45(8):522–527. https://doi.org/10.1097/BRS.0000000000003308
Cheung PWH, Wong CKH, Cheung JPY (2019) An insight into the health-related quality of life of adolescent idiopathic scoliosis patients who are braced, observed, and previously braced. Spine (Phila Pa 1976) 44(10):E596–E605. https://doi.org/10.1097/BRS.0000000000002918
Ugwonali OF et al (2004) Effect of bracing on the quality of life of adolescents with idiopathic scoliosis. Spine J 4(3):254–260. https://doi.org/10.1016/j.spinee.2003.12.001
Olafsson Y, Saraste H, Ahlgren RM (1999) Does bracing affect self-image? a prospective study on 54 patients with adolescent idiopathic scoliosis. Eur Spine J 8(5):402–405
Howard A et al (2007) Improvement in quality of life following surgery for adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 32(24):2715–2718. https://doi.org/10.1097/BRS.0b013e31815a51cd
Ward WT et al (2017) SRS-22r scores in nonoperated adolescent idiopathic scoliosis patients with curves greater than forty degrees. Spine (Phila Pa 1976) 42(16):1233–1240. https://doi.org/10.1097/BRS.0000000000002004
Merola AA et al (2002) A multicenter study of the outcomes of the surgical treatment of adolescent idiopathic scoliosis using the Scoliosis Research Society (SRS) outcome instrument. Spine (Phila Pa 1976) 27(18):2046–2051
Rushton PR, Grevitt MP (2013) What is the effect of surgery on the quality of life of the adolescent with adolescent idiopathic scoliosis? a review and statistical analysis of the literature. Spine (Phila Pa 1976) 38(9):786–794. https://doi.org/10.1097/BRS.0b013e3182837c95
Diarbakerli E et al (2018) Health-related quality of life in adulthood in untreated and treated individuals with adolescent or juvenile idiopathic scoliosis. J Bone Joint Surg Am 100(10):811–817. https://doi.org/10.2106/JBJS.17.00822
Cobb JR (1948) Outline for the study of scoliosis. Instr Course Lect AAOS 5:261–275
Einarsdottir E et al (2017) CELSR2 is a candidate susceptibility gene in idiopathic scoliosis. PLoS ONE 12(12):e0189591. https://doi.org/10.1371/journal.pone.0189591
Grauers A et al (2015) Candidate gene analysis and exome sequencing confirm LBX1 as a susceptibility gene for idiopathic scoliosis. Spine J 15(10):2239–2246. https://doi.org/10.1016/j.spinee.2015.05.013
Rowe D (2003) SRS bracing manual. Idiopathic scoliosis [cited 15 Nov 2018]. Available from: https://www.srs.org/professionals/online-education-and-resources/srs-bracing-manual
Diarbakerli E, Grauers A, Gerdhem P (2017) Population-based normative data for the scoliosis research society 22r questionnaire in adolescents and adults, including a comparison with EQ-5D. Eur Spine J 26(6):1631–1637. https://doi.org/10.1007/s00586-016-4854-0
Danielsson AJ, Romberg K (2013) Reliability and validity of the Swedish version of the scoliosis research society-22 (SRS-22r) patient questionnaire for idiopathic scoliosis. Spine (Phila Pa 1976) 38(21):1875–1884. https://doi.org/10.1097/BRS.0b013e3182a211c0
Burström K et al (2014) Swedish experience-based value sets for EQ-5D health states. Qual Life Res 23(2):431–442. https://doi.org/10.1007/s11136-013-0496-4
Rabin R, de Charro F (2001) EQ-5D: a measure of health status from the EuroQol Group. Ann Med 33(5):337–343
Cheung PWH et al (2016) Psychometric validation of the EuroQoL 5-dimension 5-level (EQ-5D-5L) in Chinese patients with adolescent idiopathic scoliosis. Scoliosis Spinal Disord 11:19. https://doi.org/10.1186/s13013-016-0083-x
Bunge EM et al (2007) Health-related quality of life in patients with adolescent idiopathic scoliosis after treatment: short-term effects after brace or surgical treatment. Eur Spine J 16(1):83–89. https://doi.org/10.1007/s00586-006-0097-9
Çolak TK et al (2017) Health related quality of life and perception of deformity in patients with adolescent idiopathic scoliosis. J Back Musculoskelet Rehabil 30(3):597–602. https://doi.org/10.3233/BMR-160564
Berliner JL et al (2013) Discriminative validity of the scoliosis research society 22 questionnaire among five curve-severity subgroups of adolescents with idiopathic scoliosis. Spine J 13(2):127–133. https://doi.org/10.1016/j.spinee.2012.10.025
Parent EC et al (2009) Discriminative and predictive validity of the scoliosis research society-22 questionnaire in management and curve-severity subgroups of adolescents with idiopathic scoliosis. Spine (Phila Pa 1976) 34(22):2450–2457. https://doi.org/10.1097/BRS.0b013e3181af28bf
Rainoldi L et al (2015) Quality of life in normal and idiopathic scoliosis adolescents before diagnosis: reference values and discriminative validity of the SRS-22. A cross-sectional study of 1,205 pupils. Spine J 15(4):662–667. https://doi.org/10.1016/j.spinee.2014.12.004
Asher M et al (2003) Discrimination validity of the scoliosis research society-22 patient questionnaire: relationship to idiopathic scoliosis curve pattern and curve size. Spine (Phila Pa 1976) 28(1):74–78. https://doi.org/10.1097/01.BRS.0000047636.95839.F5
Bagó J et al (2009) Minimal important differences of the SRS-22 patient questionnaire following surgical treatment of idiopathic scoliosis. Eur Spine J 18(12):1898–1904. https://doi.org/10.1007/s00586-009-1066-x
Acknowledgements
We would like to acknowledge Luigi Belcastro for assistance with recruitment of the subjects.
Funding
Open access funding provided by Karolinska Institute. This study was financially supported by funds from the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet, the Karolinska Institutet research funds, the Swedish Research Council (K2013-99X-22268-01-3), and the Swedish Society of Spinal Surgeons.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None declared.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Torén, S., Diarbakerli, E. Health-related quality of life in adolescents with idiopathic scoliosis: a cross-sectional study including healthy controls. Eur Spine J 31, 3512–3518 (2022). https://doi.org/10.1007/s00586-022-07428-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-022-07428-z