
Abstract
Purpose
Osteogenesis Imperfecta (OI) is a rare group of congenital genetic disorders that consists of a collagen synthesis defect. The most severe phenotype is type III OI. Characterized by progressive bone deformity, fragility and pulmonary impairment, causing significant morbidity and mortality. Also, multilevel spine deformities are observed, such as scoliosis. The literature on the pathophysiology of pulmonary impairment in relation to scoliosis in these patients is scarce and conflicting. This study aims to determine the prevalence of scoliosis and its relation to pulmonary function in type III OI patients.
Methods
This retrospective cohort study took place between April 2020 and November 2021. Forty-two patients with type III OI were included. Anterior–posterior spine radiographs were evaluated for scoliosis. Pulmonary function was assessed using spirometry and partial pressure of carbon dioxide.
Results
All 42 patients had scoliosis, with a mean curve of 66° (95% CI of range). Vital lung capacity was decreased, compared to a non-OI population (mean 1.57 L). This was correlated to the degree of scoliosis (st. β − 0.40, P = 0.03), especially in increasing thoracic curves. Restrictive lung pathophysiology was shown in our study population with a mean FEV1/FVC ratio of 0.85.
Conclusions
Increasing thoracic scoliosis was correlated with decreased vital lung capacity in our study population of type III OI patients. High FEV1/FVC ratios found in this study population show restrictive lung pathophysiology. Therefore, it is plausible that the pulmonary impairment found in type III OI patients is a combined issue, partly associated to scoliosis and partly intrinsic to OI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteogenesis Imperfecta (OI) is a rare group of congenital genetic disorders that consists of a collagen synthesis defect. This disease is characterized by altered architecture of the patients’ connective tissue, usually caused by an inherited type I collagen mutation. The altered connective tissue architecture leads to low bone mineral density, with defective bone structure and strength, often with multiple associated fractures that are typically obtained after low-impact trauma [1,2,3]. Depending on the clinical presentation and severity of the disease, OI is currently classified into five different phenotypes [1, 2, 4, 5]. Type III OI is one of the most severe manifestations and is characterized by progressive bone deformity and fragility. It has an autosomal recessive inheritance and has neonatal manifestations of bone deformity. Patients with type III OI develop a short statue, multiple fractures, spine deformities, cardiovascular insufficiency and progressive bowing of the long bones [5,6,7]. Subsequently, quality of life is reduced by these factors [8]. Pulmonary impairment is a leading cause of morbidity and mortality. It is suggested to be caused by restrictive lung physiology, but the exact etiology remains unclear [9]. Life expectancy of patients with type III OI is reduced, mostly due to cardiovascular insufficiency and pulmonary impairment including pulmonary embolisms, respiratory failure and respiratory infections [8, 10,11,12,13].
In patients with type III OI, multilevel spine deformities are observed, including spondylolisthesis and spondylolysis, cranio-cervical junction abnormalities, osteoporotic fractures, scoliosis and kyphosis [1, 14, 15]. The prevalence of scoliosis is estimated to be 47–100% [16]. Together with chest wall abnormalities, scoliosis is suggested to be the major cause for impaired pulmonary function, especially in thoracic scoliosis ≥ 60° [9, 12, 13]. In addition to scoliosis, short statue, rib fractures, hyperkyphosis and higher incidences of pectus carinatum all modify the chest wall and can therefore play a role in pulmonary impairment [9, 12].
Previous literature on the etiology of pulmonary impairment in OI patients is scarce, limited to small study populations and shows conflicting results. Several studies have related pulmonary impairment to the continuous progression of spinal deformity in all types of OI patients [17, 18]. Other studies suggest that the (restrictive) lung physiology in OI is likely related to intrinsic factors, such as the underlying connective tissue disorder, as (cardio)pulmonary complications are highly prevalent in all OI phenotypes [8, 9, 19]. These conflicting results, in small study populations, triggered this study. A better understanding of the pathophysiological mechanisms behind pulmonary impairment is required to optimize the diagnostic and therapeutic options for type III OI patients. Therefore, the aim of this study was to describe the prevalence of scoliosis and evaluate determinants associated with impaired pulmonary function in a larger cohort of type III OI patients.
Patients and methods
Design and population
This retrospective cohort study took place between April 2020 and November 2021. All adult (≥ 18 years) type III OI patients that were seen in the Dutch National Centre of Expertise for adult OI (Isala, Zwolle, The Netherlands) between 2008 and 2020, were eligible for inclusion in this study. Patients were excluded when the initial spinal radiographs or pulmonary spirometry were unavailable.
Data collection
One orthopedic surgeon and physician assistant examined all patients from 2008 until 2020, according to a standardized protocol, to collect clinical data. The data was collected using (online) standardized forms (Research Manager, version 5.58.9, Cloud9 Software BV) and analyzed retrospectively. This included patient demographics, smoking status (yes or no), use of medication, spinal radiographs, spirometry results, and health-related quality of life (HRQOL) questionnaires.
Study definitions and endpoints
Scoliosis was defined as a lateral curvature of the spine greater than 10 degrees in accordance with the Scoliosis Research Society (SRS) [20]. Scoliosis measurements from the spinal radiographs were performed in Sectra IDS7 version 23.2.0.5047 (Sectra AB, Linköping, Sweden) by two independent investigators (MK and SL) using the Cobb method [20]. Measurements were checked for interobserver variance using the intraclass correlation coefficient, which were 0.99 (95% CI 0.99–1.00) for thoracic Cobb angles and 0.99 (95% CI 0.98–0.99) for lumbar Cobb angles.
Health-related Quality of Life (HRQOL) was assessed using the SF-36. The SF-36 is a validated and widely used, self-administered generic questionnaire with 36 items involving 8 subscales: physical functioning, role limitations due to physical health problems, bodily pain, general health perception, vitality, social functioning, role limitations due to emotional problems, and mental health. The scoring scale ranges from 0 to 100, with higher scores indicating a better HRQOL. In addition, physical and mental component summary (PCS and MCS) scores were determined [21].
Pulmonary function was assessed using spirometry, recording vital capacity (VC max), forced expiratory volume in one second (FEV1), the FEV1/VC max ratio, FEV1/Forced Vital Capacity (FVC) ratio and partial pressure of carbon dioxide (pCO2). Restrictive and obstructive lung physiology were defined as FEV1/FVC > 0.8% and < 0.7%, respectively [22].
Statistical analysis
Descriptive summaries included the mean with standard deviation (SD) for normally distributed variables and the median with the interquartile range (IQR, 25th–75th percentile) for other variables. Q-Q plots were used to determine whether the tested variables were normally distributed. Linear regression models were calculated to test the association between VC max, FEV1/FVC and individual parameters. First, univariate analysis for correlation, using the Pearson product-moment correlation coefficient for continuous data and point-biserial correlation coefficient for categorical data, was performed to investigate the association between VC max, FEV1/FVC and other variables. Linearity was checked on a scatter plot. Extreme outliers, defined as three times the IQR from the 25th or 75th percentiles, were identified on a box-whisker blot and were excluded if it was a multivariate outlier. Non-parametric Spearman’s rank order correlation was performed for non-normally distributed parameters. Next, multivariate linear regression analysis (forced-entry method) was performed to investigate associations between VC max and FEV1/FVC as dependent variables and multiple independent variables. Age and height were entered in a multivariate model based on previous literature and additional variables were selected in case the P-value was ≤ 0.1 in the univariate analysis. The model was checked for collinearity (variable with vif > 10 was determined as collinear) and for variables with a non-parametric distribution, natural logarithmic (ln) transformation was performed. The quality of the model was described using the accuracy of the variance prediction by the adjusted R2 value. Normality and homoscedasticity of residuals were checked with normality plots and scatter plots. All analyses were performed using SPSS version 25.0 (IBM Corp, Amonk, NY, USA). A (two-sided) P-value of less than 0.05 was considered statistically significant.
Ethical considerations
The study was performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all patients and the protocol was approved by the institutional Medical Ethics Committee (METC Isala, Zwolle, The Netherlands; file number: 210509).
Results
Patient demographics
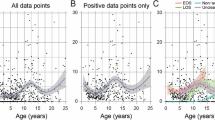
Between 2008 and 2020, a total of 42 patients were included in this study. Baseline characteristics are presented in Table 1. In brief, 52.4% of participants was male, with a median age of 25 years (19, 41.3) and the median body mass index (BMI) was 28.8 kg/m2 (23.1, 37.6). Baseline VC max was 1.57 L (0.87) and the mean capillary pCO2 was 5.04 kPa (0.61). The FEV1/FVC ratio was 85.11% (7.12), with 88% of the patients that had a FEV1/FVC ratio of > 80% (Fig. 1). All patients had scoliosis (Cobb angle > 10°). Figure 2 shows the distribution of the largest Cobb angle (thoracic or lumbar) measured. It demonstrates the severity of the scoliosis curves in this patient group, with a mean curve of 66.0° (SD 33.6°, range: 12.5°–151.4°).

FEV1/FVC ratio in patients with type III OI

Distribution of Cobb angles in patients with type III OI
Uni- and multivariate linear regression analysis
Univariate regression analysis identified height (P = 0.00), weight (P = 0.00), smoking (P = 0.04) and largest Cobb angle (P = 0.01) as statistically significant predictors for VC max (Table 2). When entered into a multivariate model, only height (st. β 0.64, P = 0.00) and largest Cobb angle (st. β − 0.40, P = 0.03) remained independent predictors of VC max.
In a post-hoc analysis, we performed multivariate regression analysis with the thoracic and lumbar Cobb angles as covariates (see supplementary Table S1). For the model with the thoracic Cobb angle (adjusted R2 for the model 0.46), the significant association was still present while in the model with the lumbar Cobb angle the association disappeared (adjusted R2 for the model 0.37) This indicates that the thoracic Cobb angle is a more important predictor for VC max than the lumbar Cobb angle. For FEV1/FVC, univariate analysis identified gender (P = 0.00) and weight (P = 0.03) as statistically significant predictors (see supplementary Table S2). When entered into a multivariate model, gender (st. β 0.48, P = 0.00) and weight (st. β − 0.34, P = 0.05) were statically significant determinants of the FEV1/FVC. Physical and mental health (measured by PCS and MCS) were not correlated to VC max (P = 0.41 and P = 0.72, respectively) or FEV1/FVC (P = 0.57 and P = 0.35, respectively) in univariate analysis, and therefore were not entered into the multivariate model.
Discussion
To our knowledge, this is the first study to evaluate pulmonary function in relation to scoliosis in type III OI patients. We found that all included type III OI patients had scoliosis and, as compared to a non-OI population, the VC max was decreased (mean 1.57 vs. 4–6 L, respectively) [22]. The degree of scoliosis was severe, with a mean curve of 66°, emphasizing the severity of the spine deformities observed in this group of type III OI patients. Most importantly, we found that the VC max was associated with the degree of scoliosis in type III OI patients. Especially increasing thoracic curves were strongly correlated with decreased VC max. Restrictive lung pathophysiology (FEV1/FVC ratio > 0.8) was present in 88% of patients, with a mean ratio of 0.85. Even though pulmonary impairment was clearly present in this study population, only two patients showed signs of respiratory failure (capillary pCO2 ≥ 6.0).
Pulmonary issues form a large part of morbidity and mortality in type III OI patients, accounting for approximately 81,6% of deaths [11, 13, 23]. Pulmonary related death in type III OI patients is higher than the 39% seen in type I and IV OI patients and 15.7% in the general population [11]. Widmann et al. found that a curve of ≥ 60 degrees in 15 OI patients resulted in a significant (< 50%) diminution in vital capacity [17]. In contrast, other authors suggest that pulmonary impairment is not correlated to scoliosis and also goes beyond chest wall deformities, stating it is intrinsic to OI [8, 19]. However, these studies are performed in small populations and do not specify between OI phenotypes. The review by Storoni et al. concluded a combined cause of pulmonary impairment. They suggested that the abnormal collagen type 1 intrinsically distorts the intrapulmonary structure and that skeletal dysplasia causes severe thoracic abnormalities [24]. Due to the correlation between continuous progression of spinal deformity and decreasing pulmonary function in patients with type III OI, we hypothesize that scoliosis increases the risk of premature death secondary to pulmonary disease. This is supported by several studies [11, 12, 17]. The restrictive lung pathophysiology that was evident in this cohort, further adds to that. These findings may have important implications for the functional evaluation and the treatment of type III OI patients. The results of this study emphasize the importance of pulmonary monitoring in this population, as spinal deformity is usually progressive and more severe degrees of (thoracic) scoliosis are related to an increased risk of pulmonary impairment. This study could help with the development of evidence-based clinical guidelines to improve overall health, quality of life and reduce morbidity and mortality.
A strength of this study is the relatively large population of type III OI patients (in light of the rarity of the disease). Limitations include lack of data on chest wall deformity, as only a few patients had a chest CT scan. Since chest wall deformity has been suggested to influence pulmonary function, inclusion of this data could have resulted in further understanding of the decreased VC max volumes. Furthermore, detailed pulmonary imaging would provide us with more information on the restrictive lung pathophysiology found in our population. Another limitation is the limited availability of lateral spinal radiographs; kyphosis measurements were not included in our analysis.
In conclusion, the degree of scoliosis was severe in this type III OI cohort, with a mean curve of 66°. This study further proves that pulmonary impairment is an important burden in type III OI patients and that increasing thoracic scoliosis is correlated with decreased vital lung capacity. The high FEV1/FVC ratios found in this study population shows restrictive lung pathophysiology. Consequently, it is plausible that the pulmonary impairment in type III OI patients is a combined issue, partly associated with scoliosis and partly intrinsic to OI. Therefore, we suggest assessing pulmonary function using spirometry starting at a young age in type III OI patients and in OI patients with severe scoliosis, in order to anticipate the health problems frequently observed in these patients.
References
Shapiro JR, Byers P, Glorieux F, Sponsellor P (2014) Osteogenesis imperfecta: a translational approach to brittle bone disease. Elsevier, New York. https://doi.org/10.1016/C2011-0-07790-6
Rauch F, Glorieux FH (2004) Osteogenesis imperfecta. Lancet 363(9418):1377–1385. https://doi.org/10.1016/S0140-6736(04)16051-0
Gertner JM, Root L (1990) Osteogenesis imperfecta. Orthop Clin North Am 21(1):151–162. https://doi.org/10.1016/S0030-5898(20)31572-8
Sillence DO, Senn A, Danks DM (1979) Genetic heterogeneity in osteogenesis imperfecta. J Med Genet 16(2):101–116. https://doi.org/10.1136/jmg.16.2.101
van Dijk FS, Sillence DO (2014) Osteogenesis imperfecta: clinical diagnosis, nomenclature and severity assessment. Am J Med Genet A 164A(6):1470–1481. https://doi.org/10.1002/ajmg.a.36545
Sillence DO, Barlow KK, Cole WG et al (1986) Osteogenesis imperfacta type delineation of the phenotype with reference to genetic heterogeneity. Am J Med Genet 23(3):821–32. https://doi.org/10.1002/ajmg.1320230309
Janus GJM, Finidori G, Engelbert RHH et al (2000) Operative treatment of severe scoliosis in osteogenesis imperfecta: results of 20 patients after halo traction and posterior spondylodesis with instrumentation. Eur Spine J 9(6):486–491. https://doi.org/10.1007/s005860000165
Khan S, Yonko E, Carter E et al (2020) Cardiopulmonary status in adults with osteogenesis imperfecta: intrinsic lung disease may contribute more than scoliosis. Clin Orthop and Relat Res 478(12):2833–2843. https://doi.org/10.1097/corr.0000000000001400
Sandhaus RA (2014) Pulmonary function in osteogenesis imperfecta. Osteogenesis imperfecta. Elsevier, New York, pp 335–342. https://doi.org/10.1016/B978-0-12-397165-4.00035-6
Radunovic Z, Wekre LL, Diep LM, Steine K (2011) Cardiovascular abnormalities in adults with osteogenesis imperfecta. Am Heart J 161(3):523–529. https://doi.org/10.1016/j.ahj.2010.11.006
McAllion SJ, Paterson CR (1996) Causes of death in osteogenesis imperfecta. J Clin Pathol 49(8):627–30. https://doi.org/10.1136/2Fjcp.49.8.627
LoMauro A, Pochintesta S, Romei M, D’Angelo MG et al (2012) Rib cage deformities alter respiratory muscle action and chest wall function in patients with severe Osteogenesis imperfecta. PLoS ONE 7(4):e35965. https://doi.org/10.1371/journal.pone.0035965
Yonko EA, Emanuel JS, Carter EM et al (2020) Respiratory impairment impacts QOL in osteogenesis imperfecta independent of skeletal abnormalities. Arch Osteoporos 15(1):153. https://doi.org/10.1007/s11657-020-00818-0
De Lima MV, De Lima FV, Akkari M et al (2015) Roentgenographic evaluation of the spine in patients with osteogenesis imperfecta. Medicine 94(47):e1841. https://doi.org/10.1097/md.0000000000001841
Arponen H, Mäkitie O, Waltimo-Sirén J (2014) Association between joint hypermobility, scoliosis, and cranial base anomalies in paediatric Osteogenesis imperfecta patients: a retrospective cross-sectional study. BMC Musculoskelet Disord 15:428. https://doi.org/10.1186/1471-2474-15-428
Liu G, Chen J, Zhou Y et al (2017) The genetic implication of scoliosis in osteogenesis imperfecta: a review. J Spine Surg 3(4):666–78. https://doi.org/10.21037/2Fjss.2017.10.01
Widmann RF, Bitan FD, Laplaza FJ et al (1999) Spinal deformity, pulmonary compromise, and quality of life in osteogenesis imperfecta. Spine 24(16):1673–1678. https://doi.org/10.1097/00007632-199908150-00008
Wekre LL, Kjensli A, Aasand K et al (2014) Spinal deformities and lung function in adults with osteogenesis imperfecta. Clin Respir J 8(4):437–443. https://doi.org/10.1111/crj.12092
Bronheim R, Khan S, Carter E et al (2019) Scoliosis and cardiopulmonary outcomes in osteogenesis imperfecta patients. Spine 44(15):1057–1063. https://doi.org/10.1097/brs.0000000000003012
Cobb JR (1948) Outline for the study of scoliosis. In: The American Academy of Orthopedic Surgeons Instructional Course Lectures, vol 5, pp 261–275
Ware JE (2000) SF-36 health survey update. Spine 26(18):2062. https://doi.org/10.1097/00007632-200012150-00008
Johnson J, Theurer W (2014) A stepwise approach to the interpretation of pulmonary function tests. Am Fam Physician 89(5):359–366
Paterson CR, Ogston SA, Henry RM (1996) Life expectancy in osteogenesis imperfecta. BMJ 312(7027):351–351. https://doi.org/10.1136/bmj.312.7027.351
Storoni S, Treurniet S, Micha D et al (2021) Pathophysiology of respiratory failure in patients with osteogenesis imperfecta: a systematic review. Ann Med 53(1):1676–87. https://doi.org/10.1080/07853890.2021.1980819
Acknowledgements
The authors thank K. Gooijer for his contribution to the SF-36 data.
Funding
No funds, grants, or other support was received for conducting this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [MC], [SL] and [PD]. The first draft of the manuscript was written by [MC] and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Keuning, M.C., Leeuwerke, S.J.G., van Dijk, P.R. et al. Prevalence of scoliosis and impaired pulmonary function in patients with type III osteogenesis imperfecta. Eur Spine J 31, 2295–2300 (2022). https://doi.org/10.1007/s00586-022-07260-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-022-07260-5