
Abstract
Purpose
Percutaneous in situ contouring is based on bilateral bending of rods on the spine, thus increasing lordosis at the fracture. It was analyzed if this technique would provide a better reduction than prone positioning and how sagittal alignment would behave.
Methods
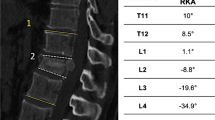
Twenty-nine patients were operated using in situ contouring and selective anterior fusion for non-neurologic A2, A3 or B2 fractures. Clinical results were assessed prospectively using visual analog scale (VAS) and Oswestry Disability Index (ODI). The radiographic deformity correction was measured by sagittal index and regional kyphosis. Sagittal balance was assessed using kyphosis, lordosis, T9 tilt, pelvic incidence, pelvic tilt and sacral slope. Posterior wall fragment reduction was evaluated by computed tomography.
Results
After 2 years, VAS and ODI were comparable to the status prior to the accident. The sagittal index was 19.7° preoperatively, 5.3° after prone positioning and −1.1° after in situ contouring (p < 0.001). The loss of correction was 2.4°, mainly during the first 3 months. Similar observations were made for regional kyphosis. The sagittal spino-pelvic alignment was stable postoperatively. A preoperative canal obstruction ≥50 % was observed in 16 patients, and the fragments migrated anteriorly in all patients.
Conclusions
Percutaneous instrumentation and anterior fusion provides good clinical results. In situ contouring increases lordosis obtained by prone positioning. Anterior column lengthening and ligamentotaxis reduce posterior wall fragments, which decompress the canal without laminectomy. The fusion of anterior defects prevents the loss of correction and provides a stable sagittal profile. The instrumentation may be removed without damaging the paravertebral muscles and loss of correction.






Similar content being viewed by others


References
Ringel F, Stoffel M, Stüer C, Meyer B (2006) Minimally invasive transmuscular pedicle screw fixation of the thoracic and lumbar spine. Neurosurgery 59:361–367
Grass R, Biewener A, Dickopf A, Rammelt S, Heineck J, Zwipp H (2006) Percutaneous dorsal versus open instrumentation for fractures of the thoracolumbar border. A comparative, prospective study. Unfallchirurg 109:297–305
Rampersaud YR, Annand N, Dekutoski MB (2006) Use of minimally invasive surgical techniques in the management of thoracolumbar trauma: current concepts. Spine 31(Suppl 1):S96–S102
Charles YP, Zairi F, Vincent C, Fuentes S, Bronsard N, Court C, Le Huec JC (2012) Minimally invasive posterior surgery for thoracolumbar fractures. New trends to decrease muscle damage. Eur J Orthop Surg Traumatol 22:1–7
Fuentes S, Blondel B, Metellus P, Gaudart J, Adetchessi T, Dufour H (2010) Percutaneous kyphoplasty and pedicle screw fixation for the management of thoraco-lumbar burst fractures. Eur Spine J 19:1281–1287
Wild MH, Glees M, Plieschnegger C, Wenda K (2007) Five-year follow-up examination after purely minimally invasive percutaneously and conventionally treated patients. Arch Orthop Trauma Surg 127:335–343
Steib JP, Aoui M, Mitulescu A, Bogorin J, Chiffolot X, Cognet JM, Simon P (2006) Thoracolumbar fractures surgically treated by “in situ contouring”. Eur Spine J 15:1823–1832
Steib JP, Charles YP, Aoui M (2010) In situ contouring technique in the treatment of thoracolumbar fractures. Eur Spine J 19(Suppl 1):S66–S68
Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S (1994) A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 3:184–201
Farcy JP, Weidenbaum M, Glassman SD (1990) Sagittal index in management of thoracolumbar fractures. Spine 15:958–965
Roussouly P, Nnadi C (2010) Sagittal plane deformity: an overview of interpretation and management. Eur Spine J 19:1824–1836
Kim DY, Lee SH, Chung SK, Lee HY (2005) Comparison of multifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixation. Spine 30:123–129
Blondel B, Fuentes S, Pech-Gourg G, Adetchessi T, Tropiano P, Dufour H (2011) Percutaneous management of thoracolumbar burst fractures: evolution of techniques and strategy. Orthop Traumatol Surg Res 97:527–532
Palmisani M, Gasbarrini A, Brodano GB, De Iure F, Cappuccio M, Boriani L, Amendola L, Boriani S (2009) Minimally invasive percutaneous fixation in the treatment of thoracic and lumbar spine fractures. Eur Spine J 18(Suppl 1):S71–S74
Pelegri C, Benchikh El Fegoun A, Winter M, Brassart N, Bronsard N, Hovorka I, de Peretti F (2008) Percutaneous osteosynthesis of lumbar and thoracolumbar spine fractures without neurological deficit: surgical technique and preliminary results. Rev Chir Orthop Reparatrice Appar Mot 94:456–463
Reinhold M, Knop C, Beisse R, Audigé L, Kandziora F, Pizanis A, Pranzl R, Gercek E, Schultheiss M, Weckbach A, Bühren V, Blauth M (2010) Operative treatment of 733 patients with acute thoracolumbar spinal injuries: comprehensive results from the second, prospective, internet-based multicenter study of the Spine study group of the German Association of Trauma Surgery. Eur Spine J 19:1657–1676
Burgos J, Rapariz JM, Gonzalez-Herranz P (1998) Anterior endoscopic approach to the thoracolumbar spine. Spine 23:2427–2431
Ni WF, Huang YX, Chi YL, Xu HZ, Lin Y, Wang XY, Huang QS, Mao FM (2010) Percutaneous pedicle screw fixation for neurologic intact thoracolumbar burst fractures. J Spinal Disord Tech 23:530–537
Rahamimov N, Mulla H, Shani A, Freiman S (2011) Percutaneous augmented instrumentation of unstable thoracolumbar burst fractures. Eur Spine J. doi:10.1007/s00586-011-2106-x
Eck JC (2011) Minimal invasive corpectomy and posterior stabilization for lumbar burst fracture. Spine J 11:904–908
Logroscino CA, Proietti L, Tamburrelli FC (2009) Minimally invasive spine stabilisation with long implants. Eur Spine J 18(Suppl 1):S75–S81
Altay M, Ozkurt B, Aktekin CN, Ozturk AM, Dogan O, Tabak AY (2007) Treatment of unstable thoracolumbar junction burst fractures with short- or long-segment posterior fixation in magerl type a fractures. Eur Spine J 16:1145–1155
Leferink VJ, Nijboer JM, Zimmerman KW, Veldhuis EF, ten Vergert EM, ten Duis HJ (2003) Burst fractures of the thoracolumbar spine: changes of the spinal canal during operative treatment and follow-up. Eur Spine J 12:255–260
Dai LY (2001) Remodeling of the spinal canal after thoracolumbar burst fractures. Clin Orthop Relat Res 382:119–123
Mueller LA, Degreif J, Schmidt R, Pfander D, Forst R, Rommens PM, Mueller LP, Rudig L (2006) Ultrasound-guided spinal fracture repositioning, ligamentotaxis, and remodeling after thoracolumbar burst fractures. Spine 31:E739–E747
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Charles, Y.P., Walter, A., Schuller, S. et al. Thoracolumbar fracture reduction by percutaneous in situ contouring. Eur Spine J 21, 2214–2221 (2012). https://doi.org/10.1007/s00586-012-2306-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-012-2306-z