
Abstract
Using markers for early diagnosis can help to reduce mortality and morbidity in systemic inflammatory response syndrome (SIRS). This study investigates the role of procalcitonin (PCT) as a prognostic value in dogs with SIRS in the intensive care unit. Fifty-five dogs were selected and studied. Blood samples were collected and investigated for PCT, white and red blood cells, iron, creatinine, platelet, glucose, albumin, urea, interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), bandcell, body temperature, and hospitalized days and costs. The animals were grouped into survivors and deceased groups, and their results were compared. The results showed negative significant relations between PCT with hematocrit (r2 = 0.294, P < 0.05) and the serum concentration of iron (r2 = 0.280, P < 0.05) and also positive relation with IL-6 (r2 = 0.456, P < 0.01) and TNF-α (r2 = 0.391, P < 0.01). Significant relations were not seen between PCT with other parameters (P > 0.05). The results also showed a significant relation between glucose and albumin with body temperature (P < 0.05). The results showed that the serum concentrations of PCT, IL-6, and TNF-α were significantly higher in deceased dogs compared with survivors, while white blood cells, glucose, albumin, urea, lymphocyte, neutrophil, and body temperature were higher in survivors compared with others. PCT can be utilized as a prognostic value and helps early diagnosis in dogs with SIRS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sepsis is known as one of the most common causes of morbidity and mortality in intensive care and is presented in different severities of systemic inflammatory response syndrome (SIRS) (Goggs and Letendre 2019). SIRS is an exaggerated defense response of the body against stressor factors, such as infection, trauma, and surgery for removing the endogenous and exogenous sources of the insult (Chakraborty and Burns 2019). The disease is known with signs such as abnormal body temperature, heart and respiratory rate, and leukocyte count (Pierini et al. 2019). The hematopoietic system and hematological disorders are also seen in patients with SIRS (Napolitano 2017). The disease causes the increase in cytokines in the blood plasma by 2–6 times (Yelins’Ka et al. 2019). In dogs with SIRS, criteria are including body temperature < 37.8 °C or > 39.4 °C, heart rate > 140 bpm, respiratory rate > 30 breaths/min or PCO2 < 32 mmHg, white blood cells < 6000 or > 16,000 cells/μL, or > 3% band neutrophils (Alves et al. 2020).
Clinicians have sought new tools to diagnose sepsis promptly. Early diagnosis and treatment may reduce mortality and morbidity (Rowe et al. 2018). A marker can help early detection and also distinguish between infectious and non-infectious causes of SIRS (Binnie et al. 2020). Traditional markers cannot be specific, such as heart and respiratory rates and white blood cell (WBC) count (Abedini et al. 2012). In addition, physicians are still faced with challenges in the correct use of antibiotics. The incorrect application of antibiotics not only increases mortalities but also leads to antibiotic-resistant, toxic side effects and healthcare costs (Gregoriano et al. 2020). Among biomarkers, procalcitonin is known to be a precise indicator of bacterial infection and/or severity of infection, and also good control of the success of a therapeutic procedure (Battaglia et al. 2021). It has been reported 79.00%, 84.00%, 69.00%, and 77.00% for sensitivity, specificity, sensitivity, and specificity (Yu et al. 2010).
Procalcitonin is an inactive propeptide of calcitonin released by C cells of the thyroid gland, hepatocytes, and peripheral monocytes. It has been reported as a useful biochemical marker to distinguish sepsis from other non-infectious causes of systemic inflammation (Rhodes et al. 2017). Indeed, pro-inflammatory cytokines stimulate the expression of genes responsible for the production of procalcitonin (Downes et al. 2020). Procalcitonin value is related to the severity of illness, and its changes are linked with severity of infection in patients (Tsui et al. 2021). Production of procalcitonin is increased 24 h after induction of infection. An appropriate treatment decreases its production, while incorrect treatment leads to future increases (Paudel et al. 2020). The serum concentration of procalcitonin is very low in healthy people while its concentration is higher in patients with infection (> 100 ng/mL) (Dever and Sheikh 2015).
Despite the role of procalcitonin as a value in human studies, it has not been still investigated as a prognostic value in dogs with SIRS. This new study works on the serum concentration of procalcitonin as a prognostic value in dogs with SIRS in the intensive care unit.
Materials and methods
Animals and protocols
This study was conducted in infectious and intensive care of a veterinary hospital for 7 months during 2020–2021 years. All the dogs with SIRS were studied. Animals with tachycardia, tachypnea, leukopenia, fewer, and/or hypothermia were studied. Clinical examinations of dogs were conducted as reported by previous studies (Giunti et al. 2017). In the current study, all the efforts were conducted to minimize stress. All the experimental procedures were in agreement with protocols advised by the Ethical Committee of Islamic Azad University, Sciences and Research Branch (IR.IAU.SRB.REC.1400.048). All dogs with trauma, surgery, burning, and other diseases interfering with this study were excluded. Finally, 55 dogs were selected and studied. Vital signs were daily recorded.
Blood sampling
Blood samples were collected from all the dogs and transferred in two tubes with and without anticoagulant (Marschner et al. 2012). A complete blood count (CBC) was daily performed to monitor dogs. To evaluate serum samples, the blood samples were centrifuged at 3000 rpm for 10 min. Sera were stored at−80 °C.
The measurement of biochemical parameters
To assess procalcitonin, specific kits (Procalcitonin Kryptor Sensitive B.R.A.H.M.S) were used as recommended by producer companies. To measure IL-6 and tumor necrosis factor-α (TNF-α), Bender Medsystem Kits were used and the results were reported as pg/mL. The serum concentration of glucose was assessed by glucose-hexokinase method using spectrophotometer (Biowave, S2100, England). The serum concentration of urease was assessed by Pars Azmoon Kit (UREA Berthelot, 18,940) as recommended by producer company. Creatinine was evaluated using Pars Azmoon Kit (UREA Berthelot, 18,940) based on recommendations of producer company. The serum concentration of iron was also assessed by Pars Azmoon Kit (BT-2000, 18,923) as recommended by producer company.
The measurement of CBC
The blood samples were analyzed for white and red blood cells, hematocrit, lymphocyte, monocytes, neutrophils, lymphocytes, and basophiles, as suggested by previous studies (Nazerian et al. 2013). At the end of the study, the animals were grouped and compared into survivors and deceased groups. Hospitalized days and treatment costs were also evaluated.
Data analysis
The blood samples were collected from 55 dogs, and sera were obtained from all the collected samples. The data were investigated for normality by Kolmogorov–Smirnov test in SPSS software (version 23). All the data were normalized and analyzed by t test. Pearson correlation was used to investigate the relationship between variables.
Results
The relation between parameters
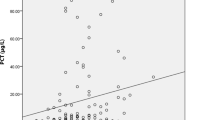
Table 1 depicts the results for the relation between parameters. The results showed negative significant relations between procalcitonin with hematocrit (r2 = 0.294, P < 0.05) and the serum concentration of iron (r2 = 0.280, P < 0.05) and also positive relation with IL-6 (r2 = 0.456, P < 0.01) and TNF-α (r2 = 0.391, P < 0.01). Significant relations were not seen between procalcitonin with other parameters (P > 0.05). There were positive relations between hematocrit with red blood cells (r2 = 0.846, P < 0.001), hemoglobin (r2 = 0.959, P < 0.001), iron (r2 = 0.791, P < 0.001), and creatinine (r2 = 0.281, P < 0.05). The results also showed significant relations between white blood cells with glucose (r2 = 0.466, P < 0.01), albumin (r2 = 0.589, P < 0.01), urea (r2 = 0.322, P < 0.05), neutrophil (r2 = 0.904, P < 0.001), eosinophil (r2 = 0.363, P < 0.05), monocyte (r2 = 0.983, P < 0.001), IL-6 (r2 = 0.486, P < 0.001), and TNF-α (r2 = 0.409, P < 0.001). There were significant relations between stress indexes of glucose and albumin with body temperature. Other significant relations are shown in Table 1.
The concentrations of parameters in survivors and deceased groups
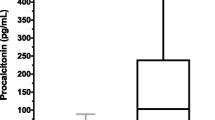
Table 2 shows the results for the concentrations of blood parameters and other parameters in survivors and deceased groups. The results showed significant differences between survivors and deceased groups for procalcitonin (P = 0.006), white blood cells (P = 0.017), glucose (P = 0.008), albumin (P = 0.0001), urea (P = 0.007), lymphocyte (P = 0.001), neutrophil (P = 0.020), IL-6 (P = 0.001), TNF-α (P = 0.001), and body temperature (P = 0.004). Based on findings, the serum concentrations of procalcitonin, IL-6, and TNF-α were significantly higher in deceased dogs compared with survivors, while white blood cells, glucose, albumin, urea, lymphocyte, neutrophil, and body temperature were higher in survivors compared with others.
Discussion
The pathogenesis of sepsis and SIRS causes to involve a complex interplay of factors and dysregulation of immunity. Early diagnosis, differentiation, and prognosis of SIRS help human and veterinary medicine with the use of appropriate treatments (Thames et al. 2019). In the current study, procalcitonin was evaluated as a prognosis factor in dogs in ICU. Several studies have reported the increase in procalcitonin in patients with sepsis and SIRS (Mustafić et al. 2018; Patil and Patil 2020; Sharma et al. 2020). The increased bacterial infection leads to increased procalcitonin (Moustafa et al. 2021). However, the serum concentration of procalcitonin has not been evaluated in dogs with SIRS in the intensive care unit.
The results showed an inverse relation between procalcitonin with hematocrit and iron. The results are in agreement with previous studies for the relation between procalcitonin with hematocrit in dogs with pyometra (Ahn et al. 2021). Our findings concur with other studies that reported a negative relationship between procalcitonin with hematocrit and iron in patients with coronary artery abnormalities (Liu et al. 2021). It has been also reported that an increase in serum concentration of procalcitonin concurs with a decrease in hematocrit and iron in patients with COVID-19 (Mertoglu et al. 2021). The increased serum concentration of procalcitonin could be attributed to greater inflammation and bacterial infection in patients in ICU. Iron and hematocrit deficiencies occur during infections (Riaty and Nursyam 2022). The decreased hematocrit and iron could be attributed to repeated hemorrhages and the administration of agents affecting iron and hematocrit.
Based on the findings, procalcitonin can be considered as a prognostic value in dogs with SIRS. There was also a positive relationship between the serum concentrations of IL-6 and TNF-α with procalcitonin. Several studies have reported a significant relations between procalcitonin with IL-6 and TNF-α in rats with mild and severe pancreatitis (Soyalp et al. 2017) and white swine (Chalkias et al. 2021). The increased serum concentrations of pro-inflammatory cytokines are directly associated with the severity and mortality of human sepsis. In fact, the cytokines lead to an increase in the variety of pathologic reactions and hypotension and shock (Chalkias et al. 2021). In fact, IL-6 is the main cytokine responsible to induce the systemic changes and promotes postoperative neurological dysfunction (Chalkias et al. 2021). TNF-α is a pro-inflammatory cytokine that participates in several physiological and pathophysiological processes and may encourage monocyte/macrophage differentiation and tumor cell necrosis/apoptosis (Sedger and McDermott 2014). SIRS is largely mediated by pro-inflammatory cytokines, and a SIRS-like clinical picture can be induced by the administration of pro-inflammatory cytokines (Natanson et al. 1989). IL-6 is known as a good diagnostic and prognostic marker in people with SIRS (Pettilä et al. 2002; Reinhart et al. 2000), and this has also been confirmed in dogs with SIRS (Rau et al. 2007). The results indicate significant relations between procalcitonin with TNF-α and IL-6. In addition, the results showed increase of 1.3 times serum concentrations of procalcitonin in deceased dogs compared with survivors. In fact, the concentration of procalcitonin is significantly higher in dogs with a chronic condition of disease. The increased procalcitonin in deceased dogs means to be appropriate as a prognostic value in dogs with SIRS in ICU.
The results also showed increased serum concentrations of IL-6 and TNF-α in deceased dogs. The findings are in agreement with those reported by Ghazizadeh et al. who showed to be high procalcitonin concentration in the acute phase of sepsis (Ghazizadeh et al. 2021). Other studies have also reported an increase in inflammatory factors in dogs with systematic infection (Gommeren et al. 2018; Kuzi et al. 2020). It has been reported that procalcitonin concentration is a marker for distinguishing infectious episodes from non-infectious episodes (Haeusler et al. 2013). The results are also parallel with those reported by Neumann and others who reported higher serum concentration of procalcitonin in dogs with sepsis in the acute phase compared with control healthy dogs (Neumann 2022). In addition, white blood cells, glucose, albumin, urea, lymphocyte, neutrophil, and body temperature were higher in survivors compared with others. The increase in parameters implicates the presence of infection and fighting the body against disease. Fighting against disease requires an energy source, and the increased glucose is a response to supplying energy for fighting against disease (Suleiman et al. 2022). The increased white blood cells and pro-inflammatory cytokines in survivor dogs highlight greater immunity in them compared with deceased dogs. All the findings show to be appropriate and specific procalcitonin as a prognostic value in dogs with SIRS.
The results did not show significant differences between survivors and non-survivors for hospitalized costs and days, although costs and days were numerically lower in survivors compared with other groups. The decrease in hospitalized days directly reduces the costs for dog owners.
Conclusion
In sum, the serum concentration of procalcitonin was higher in dogs with SIRS and especially in deceased dogs compared with survivors. It shows that pro-calcitonin is a good value for the prognosis of SIRS. In addition, procalcitonin showed a strong and positive correlation with pro-inflammatory cytokines of IL-6 and TNF-α. Based on findings, procalcitonin is a good marker for early diagnosis of SIRS in dogs admitted to ICU. Using procalcitonin helps early diagnosis of SIRS and reduces hospitalized days and costs.
References
Abedini M, Delpisheh A, Nikkhu B, Vahabi A, Afkhamzadeh A (2012) Procalcitonin and white blood cell count (WBC), erythrocyte sedimentation rate (ESR) and serum C-reactive protein (CRP) alterations in children with systemic inflammatory response syndrome before and after treatment. Afr J Biotechnol 11:10989–10993
Ahn S, Bae H, Kim J, Kim S, Park J, Kim SK, Jung DI, Yu D (2021) Comparison of clinical and inflammatory parameters in dogs with pyometra before and after ovariohysterectomy. Canad J Vet Res 85:271–278
Alves F, Prata S, Nunes T, Gomes J, Aguiar S, Aires da Silva F, Tavares L, Almeida V, Gil S (2020) Canine parvovirus: a predicting canine model for sepsis. BMC Vet Res 16:1–11
Battaglia F, Baldoneschi V, Meucci V, Intorre L, Minunni M, Scarano S (2021) Detection of canine and equine procalcitonin for sepsis diagnosis in veterinary clinic by the development of novel MIP-based SPR biosensors. Talanta 230:122347
Binnie A, Lage J, Dos Santos CC (2020) How can biomarkers be used to differentiate between infection and non-infectious causes of inflammation? Evidence-Based Prac Crit Care 14:319–335
Chakraborty RK, Burns B (2019) Systemic inflammatory response syndrome. Talanta 275:12547
Chalkias A, Spyropoulos V, Georgiou G, Laou E, Koutsovasilis A, Pantazopoulos I, Kolonia K, Vrakas S, Papalois A, Demeridou S (2021) Baseline values and kinetics of IL-6, procalcitonin, and TNF-α in landrace-large white swine anesthetized with propofol-based total intravenous anesthesia. BioMed Res Int 14:39–45
Dever J, Sheikh M (2015) spontaneous bacterial peritonitis–bacteriology, diagnosis, treatment, risk factors and prevention. Aliment Pharmacol Therap 41:1116–1131
Downes KJ, Fitzgerald JC, Weiss SL (2020) Utility of procalcitonin as a biomarker for sepsis in children. J Clin Microbiol 58:e01851-e1919
Ghazizadeh F, Noroozi M, Shekari M (2021) Comparison of the relationship between procalcitonin and crp with prognosis of fever and neutropenia in children with acute lymphoblastic leukemia. Studies Med Sci 32:335–341
Giunti M, Troia R, Battilani M, Giardino L, Dondi F, Andreani G, Fracassi F (2017) Retrospective evaluation of circulating thyroid hormones in critically ill dogs with systemic inflammatory response syndrome. J Vet Sci 18:471–477
Goggs R, Letendre J (2019) Evaluation of the host cytokine response in dogs with sepsis and noninfectious systemic inflammatory response syndrome. J Vet Emerg Crit Care 29:593–603
Gommeren K, Desmas I, Garcia A, Bauer N, Moritz A, Roth J, Peeters D (2018) Inflammatory cytokine and C-reactive protein concentrations in dogs with systemic inflammatory response syndrome. JJ Vet Emerg Crit Care 28:9–19
Gregoriano C, Heilmann E, Molitor A, Schuetz P (2020) Role of procalcitonin use in the management of sepsis. J Thoracic Dis 12:S5
Haeusler GM, Carlesse F, Phillips RS (2013) An updated systematic review and meta-analysis of the predictive value of serum biomarkers in the assessment of fever during neutropenia in children with cancer. Pediatr Infect Dis J 32:e390–e396
Kuzi S, Mazaki-Tovi M, Suchodolski JS, Rimer D, Lidbury JA, Steiner JM, Buono A, Nivy R, Segev G, Aroch I (2020) Protease inhibitors, inflammatory markers, and their association with outcome in dogs with naturally occurring acute pancreatitis. J Vet Inter Med 34:1801–1812
Liu HH, Chen WX, Niu MM, Jiang Q, Qiu Z, Fan GZ, Li RX, Mammadov G, Wu YF, Luo HH (2021) A new scoring system for coronary artery abnormalities in Kawasaki disease. Pediatr Res 14:1–9
Marschner CB, Kristensen AT, Spodsberg EH, Wiinberg B (2012) Evaluation of platelet aggregometry in dogs using the M ultiplate platelet analyzer: impact of anticoagulant choice and assay duration. J Vet Emerg Crit Care 22:107–115
Mertoglu C, Huyut MT, Arslan Y, Ceylan Y, Coban TA (2021) How do routine laboratory tests change in coronavirus disease 2019? Scand J Clin Lab Invest 81:24–33
Moustafa R, Albouni T, Aziz G (2021) The role of procalcitonin and presepsin in the septic febrile neutropenia in acute leukemia patients. PLoS ONE 16:e0253842
Mustafić S, Brkić S, Prnjavorac B, Sinanović A, Porobić-Jahić H, Salkić S (2018) Diagnostic and prognostic value of procalcitonin in patients with sepsis. Med Glas 15:10–20
Napolitano LM (2017) Anemia and red blood cell transfusion: advances in critical care. Crit Care Clin 33:345–364
Natanson C, Eichenholz PW, Danner RL, Eichacker P, Hoffman WD, Kuo GC, Banks S, MacVittie T, Parrillo J (1989) Endotoxin and tumor necrosis factor challenges in dogs simulate the cardiovascular profile of human septic shock. J Exper Med 169:823–832
Nazerian S, Gholipour KH, Jafarian MH, Soltani M, Esmaeili MA (2013) Effect of Dietary Garlic Powder on Some Hematological Indices of Beluga (huso Huso) 10:45–68
Neumann A (2022) Rapid release of sepsis markers heparin-binding protein and calprotectin triggered by anaerobic cocci poses an underestimated threat. Anaerobe 75:102584
Patil HV, Patil VC (2020) Comparative study of procalcitonin and C-reactive protein in patients with sepsis. J Natural Sci Biol Med 11:85–93
Paudel R, Dogra P, Montgomery-Yates AA, Yataco AC (2020) Procalcitonin: a promising tool or just another overhyped test? Int J Med Sci 17:332–352
Pettilä V, Hynninen M, Takkunen O, Kuusela P, Valtonen M (2002) Predictive value of procalcitonin and interleukin 6 in critically ill patients with suspected sepsis. Intens Care Med 28:1220–1225
Pierini A, Gori E, Lippi I, Ceccherini G, Lubas G, Marchetti V (2019) Neutrophil-to-lymphocyte ratio, nucleated red blood cells and erythrocyte abnormalities in canine systemic inflammatory response syndrome. Res Vet Sci 126:150–154
Rau S, Kohn B, Richter C, Fenske N, Küchenhoff H, Hartmann K, Härtle S, Kaspers B, Hirschberger J (2007) Plasma interleukin-6 response is predictive for severity and mortality in canine systemic inflammatory response syndrome and sepsis. Vet Clin Pathol 36:253–260
Reinhart K, Karzai W, Meisner M (2000) Procalcitonin as a marker of the systemic inflammatory response to infection. Intens Care Med 26:1193
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME (2017) Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 43:304–377
Riaty Z, Nursyam DE (2022) Analysis of hemoglobin levels and hematocrite value in stunting children in bukit sileh, solok regency. In "1st International Conference on Health Sciences and Biotechnology (ICHB 2021)", pp. 156–159. Atlantis Press
Rowe CR, Newberry DM, Jnah AJ (2018) Congenital syphilis: a discussion of epidemiology, diagnosis, management, and nurses’ role in early identification and treatment. Adv Neonatal Care 18:438–445
Sedger LM, McDermott M (2014) TNF and TNF-receptors: from mediators of cell death and inflammation to therapeutic giants–past, present and future. Cytokine Growth Factor Rev 25:453–472
Sharma A, Ray S, Mamidipalli R, Kakar A, Chugh P, Jain R, Ghalaut MS, Choudhury S (2020) A comparative study of the diagnostic and prognostic utility of soluble urokinase-type plasminogen activator receptor and procalcitonin in patients with sepsis and systemic inflammation response syndrome. Ind J Crit Care Med 24:245
Soyalp M, Yalcin M, Oter V, Ozgonul A (2017) Investigation of procalcitonin, IL-6, oxidative stress index (OSI) plasma and tissue levels in experimental mild and severe pancreatitis in rats. Bratisl Lek Listy 118:137–141
Suleiman MA, Umaru T, Dauda K, John SR, Usman MA (2022) Hyponatraemia and hypokalaemia relationship with alterations of glucose, cholesterol and total protein levels during human infection with Plasmodium falciparum. Compar Clin Pathol 31:557–563
Thames BE, Barr JW, Suchodolski JS, Steiner JM, Heilmann RM (2019) Prospective evaluation of S100A12 and S100A8/A9 (calprotectin) in dogs with sepsis or the systemic inflammatory response syndrome. J Vet Diagn Invest 31:645–651
Tsui T-L, Huang Y-T, Kan W-C, Huang M-S, Lai M-Y, Ueng K-C, Shiao C-C (2021) A novel procalcitonin-based score for detecting sepsis among critically ill patients. PLoS ONE 16:e0245748
Yelins’Ka AM, Akimov OY, Kostenko VO (2019) Role of AP-1 transcriptional factor in development of oxidative and nitrosative stress in periodontal tissues during systemic inflammatory response. Ukrain Biochem J 10:80–85
Yu Z, Liu J, Sun Q, Qiu Y, Han S, Guo X (2010) The accuracy of the procalcitonin test for the diagnosis of neonatal sepsis: a meta-analysis. Scand J Infect Dis 42:723–733
Acknowledgements
Authors would like to appreciate Islamic Azad University, Science and Research Branch for their support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was not supported by any funding.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All the experimental procedures were in agreement with protocols advised by Ethical Committee of Islamic Azad University, Sciences and Research Branch (IR.IAU.SRB.REC.1400.048).
Informed consent
For this type of study informed consent is not required.
Consent for publication
For this type of study consent for publication is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chadorneshin, J.R., Khaksar, E., Sharif, M.T. et al. The prognostic value of procalcitonin in critically ill cases of systematic inflammatory response syndrome in dogs. Comp Clin Pathol 32, 91–97 (2023). https://doi.org/10.1007/s00580-022-03417-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00580-022-03417-2