
Abstract
Purpose
We investigated the impact of surgical masks (SM) during oxygen therapy using oxygen masks in volunteer- and simulation-based studies.
Methods
Fifteen volunteers wore the Hudson RCI® or Open-Face Mask® with/without an SM. The fraction of inspired oxygen concentration (FIO2), end-tidal CO2 (EtCO2), partial pressure of inspired CO2 (PICO2), and respiratory rate (RR) were measured. The oxygen flow rate increased from 0 to 10 L/min. In the simulation-based study, FIO2 was measured using a simulator that reproduced spontaneous breathing. RR was 12 or 24 bpm, and the tidal volume (Tv) was 300, 500, or 700 mL. The effect of oxygen mask fitting conditions was also examined. The primary outcome measure was FIO2 at 6 L/min.
Results
In the volunteer-based study, FIO2 was reduced when the SM was used with the Hudson RCI® or Open-Face Mask®. The FIO2 drop was larger with the Open-Face Mask® than with the Hudson RCI®. The RR, EtCO2, and PICO2 significantly changed with the SM, but the differences were not clinically meaningful. In the simulation-based study, the SM with the Hudson RCI® did not reduce FIO2, but the SM with the Open-Face Mask® significantly decreased FIO2 under several conditions. However, the SM with the Hudson Mask® reduced FIO2 when the fit of the mask was inadequate. With the Open-Face Mask®, lower RR and Tv resulted in larger differences in FIO2.
Conclusions
The SM decreased FIO2 during oxygen therapy with oxygen masks. The impact of SM depended on the type of the oxygen mask, mask fitting, and respiratory condition.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since the beginning of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic, infection prevention measures have become more important than ever. The coexistence of effective oxygen supply and droplet prevention in patients with respiratory symptoms is an urgent issue. The simple oxygen mask may disperse potentially infectious exhaled air, even when the nose and mouth are covered. Hui et al. showed that exhaled air at peak exhalation dispersed into a surrounding distance of approximately 0.40 m when the simple oxygen mask was used at an oxygen flow rate of 4 L/min, breathing, 12 bpm, and a tidal volume of 500 mL [1]. Coughing could extend the dispersion distance beyond 0.4 m [2].
The use of a surgical mask significantly reduces cough-related aerosol dispersion, which is helpful for infection control [3, 4]. To prevent infection, patients on oxygen therapy may also be required to wear a surgical mask [5]. Some reports have investigated the risks of surgical masks during oxygen therapy using an oxygen mask [6,7,8,9]; however, the evidence regarding the conditions involved in the impact of the surgical masks on FIO2 has been limited. Additionally, the presence of a surgical mask may cause difficulty in breathing and affect breathing patterns [10].
This study aimed to investigate the impact of a surgical mask during oxygen therapy on the fraction of inspired oxygen concentration (FIO2). The volunteer and simulation-based studies were conducted using two types of oxygen masks with different mechanisms: simple and open designs. Our findings may be useful in cases where surgical masks must be worn during oxygen therapy for infection control.
Methods
Volunteer-based study
This study was reviewed and approved by the Ethics Committee of Tokushima University Hospital in advance (approval number: 3854). This clinical trial was registered at the University Hospital Medical Information Network center (UMIN000042557). Prior written informed consent was obtained from all volunteers. This randomized, cross-over, single-blind study complies with the CONSORT statement.
Male and female volunteers aged 20–60 years with an American Society of Anesthesiologists’ physical status (ASA PS) score of 1–2 and Hugh-Jones of 1 were recruited at the Department of Anesthesiology, Tokushima University Hospital. The study was conducted in the operating room of Tokushima University Hospital. A sampling tube was inserted from the volunteer’s nasal cavity toward the oropharynx by 13–15 cm to collect inhalation and exhalation samples. Volunteers wore the Hudson RCI® (Teleflex Inc., Pennsylvania, USA) or Open-Face Mask® (Atom Medical Inc., Tokyo, Japan) with or without a surgical mask (PRO-LANE® Level-1, Medicom Inc., Montreal, Canada) (Fig. 1). The elastics of the surgical mask were placed over the ears so that the mask covered the mouse and nose. The participants were instructed to use a headband when wearing the oxygen mask. The surgical mask was placed under the oxygen mask for volunteers equipped with both. The volunteers assumed a supine resting position and listened to their preferred music to relax. Breathing techniques were not specified or advised; volunteers breathed as they felt comfortable. The oxygen flow rate was increased from 0 to 10 L/min in increments of 2 L/min, and FIO2, end-tidal carbon dioxide (EtCO2 mmHg), and partial pressure of inspired carbon dioxide (PICO2 mmHg) were measured from inhalation and exhalation samples (Sampling Flow Rate 200 mL min−1, GF-220R and CSM-1502, NIHON KOHDEN, Tokyo). Measurements were started at least 1 min after each oxygen flow rate was changed. Five respirations were recorded when the EtCO2 waveform showed a good shape, which clearly appeared from phase 1 to phase 4 and avoided disruption of the EtCO2 waveform. The median of the data for five breaths was adopted. Volunteers drew lots randomly to determine the sequence of wearing a surgical mask. The washout period between the first and second sequence was at least 5 min, and the second measurement was started after confirming that the fraction of exhaled oxygen had returned to the first baseline. The observer was blinded to whether the volunteer was wearing a surgical mask. Volunteers were blinded to the oxygen flow rate, the values of samples from respirations, and the onset of data measurement. The primary outcome measure was FIO2 at an oxygen flow rate of 6 L/min with and without the surgical mask. The secondary outcome measures were the number of participants who had a decrease in FIO2 by 1 standard deviation (SD) due to the surgical mask. FIO2, EtCO2, PICO2, and respiratory rate at each oxygen flow rate were also considered.

Experimental mask fitting. The mannequin wore the Hudson RCI® or open-Face Mask®, with or without a surgical mask
Simulation-based study
We constructed a simulation model of oxygen therapy using an oxygen mask using the Dual Adult Lung Simulator (Michigan Instruments Inc., Michigan, USA) that can reproduce spontaneous breathing (Fig. 2). Two oxygen masks with different mechanisms were used: the Hudson RCI® (Teleflex Inc., Pennsylvania, USA), commonly referred to as the simple mask; and Open-Face Mask® (Atom Medical Inc., Tokyo, Japan), commonly referred to as the open-design mask. FIO2 was measured in these oxygen masks, with or without a surgical mask (PRO-LANE® Level-1, Medicom Inc., Montreal, Canada). The surgical mask was placed under each oxygen mask. The compliance of the lung simulator was 0.05 L/cmH2O, and the airway resistance was 5 cmH2O/L/sec. The respiratory rate was set at 12 or 24 bpm, and the tidal volume was set at 300, 500, or 700 mL. The oxygen flow rate was increased from 0 to 10 L/min in increments of 2 L/min, and FIO2 was measured from the sample in the trachea of the simulator (Sampling Flow Rate 200 mL/min, GF-220R and CSM-1502, NIHON KOHDEN, Tokyo, Japan). Measurements were started at least 1 min after each oxygen flow rate was changed. Data were collected in triplicate. The washout periods between the experiments were at least 5 min, and the subsequent measurement was started after confirming that the oxygen concentration inside the simulator had returned to the baseline. The primary outcome measure was FIO2 at an oxygen flow rate of 6 L/min with and without the surgical mask. The secondary outcome measures were FIO2 at each oxygen flow rate.

Experimental diagrams
The following simulator-based experiments were also conducted to determine whether the fit of the oxygen mask would affect the impact of a surgical mask on FIO2. As in the above experiment, two type of masks, the Hudson RCI® and Open-Face Mask® were worn with or without a surgical mask (PRO-LANE® Level-1). In a scenario where the oxygen mask was ideally worn, the rubber headband of the oxygen mask was securely attached so that there was as minimal space around the oxygen mask. In a scenario where the oxygen mask was roughly worn, the headband was not used and the oxygen mask was simply placed on the simulator’s face. The respiratory rate was set at 12 bpm, and the tidal volume was set at 500 mL. The oxygen flow rate was set to 6 L/min, and FIO2 was measured from the sample in the trachea of the simulator. A gas sampling tube was also placed on the lips and on the surgical mask to measure oxygen concentrations. The oxygen ratio inside and outside the surgical mask was calculated.
Statistical analysis
The sample size was determined as follows. The sample size of the volunteer-based study was determined to be 15. With this sample size, an effect size dz of 0.8 can be detected with the paired t test when the α error and power (1−β) are set to 0.05 (two sided) and 0.8, respectively. The effect size of 0.8 corresponds to mean difference of 0.08 when the SD is set to be 0.1 in a volunteer-based study. Triplicate measurements were performed in the simulation-based study. This sample size of 3 can detect an effect size dz of 3.3 when α was set to 0.05 (two sided) and power to 0.8 with the Student’s t test. The effect size of 3.3 corresponds to the mean difference of 0.1 when we estimated the standard deviation (SD) to be 0.03 in a simulation-based study. The sample size was calculated using G* power version 3.1.9.6 (Heinrich Heine University, Düsseldorf, Germany).
Data are shown as the mean (SD) or [95% confidence interval (95% CI)]. Paired t tests were performed on paired samples in the volunteer-based study after confirming that the carryover effect and period effect of the cross-over design were denied by repeated measure analysis of variance (ANOVA). Ratios were compared by the chi-square test or Fisher’s exact test if there were five or fewer cells. Student’s t tests were performed in the values between the presence and absence of surgical masks in the simulation-based study. Comparisons of two factors were performed by two-way ANOVA followed by the Student’s t tests (Bonferroni correction) as post-hoc tests. All p-values were two sided, and p < 0.05 was considered statistically significant. Statistical analyses were performed using EZR (Saitama Medical Centre, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R version 4.0.3 (The R Foundation for Statistical Computing, Vienna, Austria). More precisely, it is a modified version of R commander designed to add statistical functions frequently used in biostatistics. [11]
Results
Volunteer-based study
Fifteen volunteers were enrolled in the volunteer-based study (Fig. 3). The characteristics of the volunteers were as follows: 8 male (53.3%) and 7 female (46.7%); mean age 36.3 (8.4) years; mean height 163.5 (9.9) cm; mean body weight 58.7 (15.5) kg; and mean body mass index (BMI) 21.6 (3.4). At an oxygen flow rate of 0 L/min (baseline) there was no significant difference in FIO2, EtCO2, PICO2, and respiration rate with or without a surgical mask.

Study flow diagram. n number
The FIO2 significantly decreased when participants were wearing a surgical mask with the Hudson RCI®. The FIO2 at an oxygen flow rate of 6 L/min were 0.56 (0.08) and 0.49 (0.07) without and with a surgical mask, respectively, and the mean difference was − 0.07 (95% CI − 0.13 to − 0.02, p = 0.011) (Fig. 4a, Online resource 1). Additionally, the FIO2 significantly decreased when participants were wearing a surgical mask with the Open-Face Mask®. The FIO2 at an oxygen flow rate of 6 L/min was 0.48 (0.07) and 0.37 (0.10) without and with a surgical mask, respectively, and the mean difference was − 0.12 (95% CI − 0.16 to − 0.07, p < 0.001) (Fig. 4b, Online resource 1).

The results of the volunteer-based study. FIO2 the fraction of inspired oxygen concentration. Data are given as mean (standard deviation SD). *indicates statistically significant values
Six (40.0%) participants using the Hudson RCI® and 13 (86.7%) participants using the Open-Face Mask® experienced a decrease in FIO2 by 1 SD or greater due to the surgical mask, respectively. The Hudson RCI® resulted in significant fewer incidences of decreased FIO2 compared to the Open-Face Mask® (p = 0.021).
There were statistically significant differences in respiratory rate, EtCO2, and PICO2 between with and without surgical masks. However, the mean difference was small (Online resource 1).
Simulation-based study
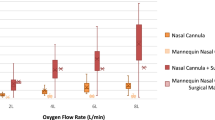
When used with the Hudson RCI®, the surgical mask did not decrease FIO2 at an oxygen flow rate of 6 L/min at all respiratory conditions. Rather, the surgical mask significantly increased FIO2 under the following conditions: at a respiratory rate of 12 bpm and tidal volume of 300 mL, the FIO2 at an oxygen flow rate of 6 L/min were 0.48 (0.01) and 0.57 (0.03) without and with surgical masks, respectively, and the mean difference was 0.09 (95% CI 0.04–0.14, p = 0.010). At a respiratory rate of 12 bpm and tidal volume of 500 or 700 mL, there were no significant differences in FIO2 at an oxygen flow rate of 6 L/min with or without a surgical mask. At a respiratory rate of 24 bpm and tidal volume of 300 mL, there was no significant difference in FIO2 at an oxygen flow rate of 6 L/min. At a respiratory rate of 24 bpm and tidal volume of 500 or 700 mL, the FIO2 at an oxygen flow rate of 6 L/min was statistically significantly higher in the presence of the surgical mask, but the mean difference was small (Fig. 5a, Online resource 2).

FIO2 at each breathing condition in the simulation-based study. FIO2 the fraction of inspired oxygen concentration; RR Respiratory Rate; Tv tidal volume. Data are given as mean (standard deviation SD). *indicates statistically significant values
When used with the Open-Face Mask®, the surgical mask significantly decreased FIO2 at an oxygen flow rate of 6 L/min at the following respiratory conditions: at a respiratory rate of 12 bpm and tidal volume of 300 mL, the FIO2 at an oxygen flow rate of 6 L/min were 0.67 (0.02) and 0.43 (0.02) without and with surgical mask, respectively, and the mean difference was − 0.24 (95% CI − 0.28 to − 0.20, p < 0.001). The mean difference in FIO2 reduced with an increase in tidal volume. At a respiratory rate of 24 bpm and tidal volume of 300 mL, the FIO2 at an oxygen flow rate of 6 L/min were 0.54 (0.01) and 0.42 (0.01) without and with surgical masks, respectively, and the mean difference was − 0.12 (95% CI − 0.13 to − 0.11, p < 0.001). The mean difference in FIO2 reduced as the tidal volume increased. At a respiratory rate of 24 bpm and tidal volume of 700 mL, there was no significant difference in FIO2 at an oxygen flow rate of 6 L/min (Fig. 5b, Online resource 2).
The results regarding the impact of mask fitting and surgical masks on FIO2 are as follows. For the Hudson RCI®, there was a significant difference in the mask fitting factor (F [1, 8] = 726.07, p < 0.001), surgical mask factor (F [1, 8] = 130.67, p < 0.001), and the interaction effects (F [1, 8] = 130.67, p < 0.001). Post hoc tests revealed a significant effect of a surgical mask with the rough mask fit (with surgical mask < without surgical mask, p < 0.001) but not the ideal fit (p = 1) (Fig. 6a). The rough mask fit resulted in a significant larger difference in oxygen concentration inside and outside the surgical mask compared to the ideal fit [91.4% (2.6%), 73.8% (2.2%), respectively, p < 0.001] (Online resource 3). As for the Open-Face Mask®, there was a significant difference in surgical mask factor (F [1, 8] = 208.33, p < 0.001) but not the mask fitting factor (F [1, 8] = 4.48, p = 0.067) and the interaction effects (F [1, 8] = 4.48, p = 0.067). (Fig. 6b).

FIO2 at each mask fitting condition, the simulation-based study. FIO2 the fraction of inspired oxygen concentration. Data are given as mean (standard deviation, SD). *indicates statistically significant values
Discussion
In the present study, two oxygen masks with different mechanisms were used: the Hudson RCI®, commonly referred to as the simple mask, and the Open-Face Mask®, commonly referred to as the open-design mask. A volunteer-based study showed that the surgical mask reduced the FIO2 when the Hudson RCI® or Open-Face Mask® was also used. However, the incidence rate of large FIO2 drops was higher with the use of the Open-Face Mask® than the Hudson Mask®. The respiratory rate, the EtCO2, and PICO2 were slightly changed by the surgical mask, but the differences were not clinically meaningful. These results support the findings of previous studies, which showed that the surgical mask did not provide clinically significant physiological impact [12, 13]. The decrease in FIO2 observed in the volunteers was unlikely to have been significantly affected by changes in breathing conditions.
The simulation-based study showed that no decrease in FIO2 was observed when the Hudson RCI® was combined with a surgical mask. However, FIO2 became significantly lower with a surgical mask when the Hudson RCI® was worn inadequately. This result may explain the risk of the lower FIO2 when volunteers wore surgical masks with the Hudson Mask® because mask fitting varies from person to person. It is possible that the presence of a surgical mask may have affected the fitting of the volunteer’s oxygen mask. On the other hand, the simulation-based study showed that the FIO2 was significantly decreased when the Open-Face Mask® was combined with a surgical mask despite an ideal fit. A reduced respiratory frequency and tidal volume was associated with a larger the difference in FIO2.
The mechanisms of oxygen supply in the simple and open-design oxygen masks are different. The simple oxygen mask allows oxygen to accumulate in the mask area. As our simulator-based study showed, if the simple oxygen mask can be fitted without gaps, it was possible to take in oxygen-enriched air from the mask area even when a surgical mask is used. However, if the simple oxygen mask is poorly fitted, a surgical mask may decrease FIO2 because of the increased leakage around the mask. On the other hand, the open-type oxygen mask does not have any reservoir to accumulate oxygen. The open-design oxygen mask was designed to increase the oxygen concentration in the nose-mouth zone by blowing oxygen and allowing for oxygen-enriched air to move around the nose-mouth zone [14]. It is possible that subjects could not efficiently inhale air from the high-concentration oxygen area in the presence of the surgical mask, while the open-design oxygen mask has the advantage of reducing the amount of carbon dioxide that is rebreathed compared to a simple mask [14,15,16].
This study has the following limitations. The values obtained from the simulation-based and volunteer-based studies may be different from the values in actual clinical practice. Patients receiving oxygen therapy have varying degrees of respiratory function and status. The performance of a low-flow oxygen device depends on the respiratory rate, tidal volumes, and the fit of the mask [15, 17, 18]. Moreover, a variety of oxygen delivery devices are available in the market from different companies; the effect of surgical masks on other oxygen delivery devices remains unknown. However, similar open-design oxygen delivery devices, such as the OxyMask™ (Southmedic Inc, Ontario, Canada), have the same basic principle as the open-type mask that was used in this study, which is to create a high-oxygen gradient in the nasal-mouth area, although there are minor differences. These open-design oxygen devices also carry a risk of lowering FIO2 from normal values when a surgical mask is worn.
In this study, the surgical masks decreased FIO2 when two different types of oxygen masks are used: the Hudson RCI® and Open-Face Mask®. Our results showed that the impact of the surgical mask on oxygen therapy depended on the type of the oxygen mask, mask fitting, and breathing condition.
References
Hui DS, Ip M, Tang JW, Wong AL, Chan MT, Hall SD, Chan PK, Sung JJ. Airflows around oxygen masks: a potential source of infection? Chest. 2006;130:822–6.
Hui DS, Hall SD, Chan MT, Chow BK, Ng SS, Gin T, Sung JJ. Exhaled air dispersion during oxygen delivery via a simple oxygen mask. Chest. 2007;132:540–6.
Leung NHL, Chu DKW, Shiu EYC, Chan KH, McDevitt JJ, Hau BJP, Yen HL, Li Y, Ip DKM, Peiris JSM, Seto WH, Leung GM, Milton DK, Cowling BJ. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. 2020;26:676–80.
Hui DS, Chow BK, Chu L, Ng SS, Lee N, Gin T, Chan MT. Exhaled air dispersion during coughing with and without wearing a surgical or N95 mask. PLoS ONE. 2012;7: e50845.
Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: guidelines from the difficult airway society, the association of anaesthetists the intensive care society, the faculty of intensive care medicine and the royal college of anaesthetists. Anaesthesia. 2020;75:785–99.
Hamada S, Tanabe N, Hirai T. Effects of combined oxygen and surgical masks on inspired fraction of oxygen: relevance to COVID-19-induced respiratory failure. Br J Anaesth. 2021;126:e215–7.
Binks AC, Parkinson SM, Sabbouh V. Oxygen: under or over a surgical facemask for COVID-19 patients? Anaesthesia. 2020;75:1691–2.
Matsui Y, Takazawa T, Takemae A, Saito S. Does a surgical mask improve oxygenation in COVID-19 patients? JA Clin Rep. 2021;7:34.
Matsui Y, Takazawa T, Takemae A, Murooka Y, Kanamoto M, Saito S. Investigation of the optimal method of oxygen administration with simultaneous use of a surgical mask: a randomized control study. J Anesth. 2022;36:26–31.
Matusiak L, Szepietowska M, Krajewski P, Bialynicki-Birula R, Szepietowski JC. Inconveniences due to the use of face masks during the COVID-19 pandemic: a survey study of 876 young people. Dermatol Ther. 2020;33: e13567.
Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48:452–8.
Roberge RJ, Kim JH, Benson SM. Absence of consequential changes in physiological, thermal and subjective responses from wearing a surgical mask. Respir Physiol Neurobiol. 2012;181:29–35.
Samannan R, Holt G, Calderon-Candelario R, Mirsaeidi M, Campos M. Effect of face masks on gas exchange in healthy persons and patients with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2021;18:541–4.
Lamb K, Piper D. Southmedic oxymask(TM) compared with the hudson RCI(®) non-rebreather mask(TM): safety and performance comparison. Can J Respir Ther. 2016;52:13–5.
Kallstrom TJ. American association for respiratory C AARC clinical practice guideline: oxygen therapy for adults in the acute care facility 2002 revision & update. Respir Care. 2002;47:717–20.
Bateman NT, Leach RM. ABC of oxygen. Acute oxygen therapy BMJ. 1998;317:798–801.
Wagstaff TA, Soni N. Performance of six types of oxygen delivery devices at varying respiratory rates. Anaesthesia. 2007;62:492–503.
Sim MA, Dean P, Kinsella J, Black R, Carter R, Hughes M. Performance of oxygen delivery devices when the breathing pattern of respiratory failure is simulated. Anaesthesia. 2008;63:938–40.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
This work did not receive any external funding.
Author information
Authors and Affiliations
Contributions
MK: Conceptualization, Methodology, Investigation, Analysis, Writing—Original Draft; YI: Methodology, Investigation, Analysis; RK: Methodology, Investigation, Analysis; MM: Investigation, Visualization; KT: Conceptualization, Data Curation, Writing—Review and Editing, Supervision, Project administration.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
About this article

Cite this article
Kinoshita, M., Ishikawa, Y., Sekiguchi, R. et al. Impact of surgical masks on fraction of inspired oxygen during oxygen therapy depends on the type of oxygen masks and respiratory conditions: volunteer- and simulation-based studies. J Anesth 36, 633–641 (2022). https://doi.org/10.1007/s00540-022-03083-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-022-03083-2