
Abstract
The study focused on designing a portable, objective device for assessing and addressing Cervical Motor Control (CMC) impairments. This device is based on a proposed architecture that employs advanced technology to evaluate and enhance patients’ CMC. During a pilot study with 10 participants, the device’s feasibility and usability were verified, including an initial assessment using the Head Relocation Test and a 12-session intervention over 4 weeks. The architecture of the proposed system is responsible for gathering pertinent data concerning patients’ cervical motor control. It employs advanced algorithms to process this data and objectively assess CMC function. Furthermore, the system tailors the therapy to each patient’s individual needs. Preliminary results indicate that the device and the proposed architecture positively impact assessment test performance accuracy. While additional validation tests are required to confirm their effectiveness, this device emerges as a promising and valuable alternative for assessing and treating patients with CMC impairments. Its focus on advanced technology and personalized adaptation aligns with previous research in telerehabilitation and classroom physical activity promotion.
Similar content being viewed by others


1 Introduction
Neck pain is a significant public health issue in the general population. Cervical Motor Control (CMC) stands out as one of the most common motor impairments in the general population, with an even higher incidence in individuals suffering from chronic conditions [1]. This motor impairment of the neck and head is manifested through challenging symptoms, including balance issues, vertigo, dizziness, and an increased risk of falls [2]. It is often accompanied by discomfort and pain in the cervical area, further complicating this condition.
The assessment and effective treatment of Cervical Motor Control (CMC) become crucial aspects in the care of these patients. On the one hand, appropriate assessment is essential to identify the origin of this impairment, evaluate the functional status of the cervical area, and precisely monitor the condition’s progression [3]. On the other hand, treatment requires specific approaches to improve both the ability to maintain the cervical spine stable in a static position and the capacity to perform controlled and precise movements. Currently, devices used for assessing and treating CMC are predominantly analog or involve equipment that, due to their weight or volume, restrict patient mobility [4]. Moreover, they often rely on subjective measures that hinder accurately tracking a patient’s progress.
Technological advancements have played a pivotal role in enhancing Cervical Motor Control (CMC) solutions. In recent years, researchers have employed various technologies to address this condition and improve the quality of life for patients. Among the technologies used for CMC assessment, motion analysis systems utilizing motion-tracking cameras and position sensors to evaluate cervical mobility have been implemented [5]. These systems enable an objective and precise measurement of neck and head movements. Virtual and augmented reality technologies have proven valuable in CMC treatment by providing immersive and customizable training environments [6]. These systems allow patients to engage in therapeutic exercises more engagingly and effectively [7].
Our study presents a dual-front approach to advance the assessment and treatment of Cervical Motor Control (CMC) impairments. The first facet of our work is the development of a device that stands out from conventional machines due to its compact shape and user-friendly design, allowing for a precise evaluation of CMC. The size and ease of use of our device overcome the common obstacles associated with bulkier traditional equipment, ensuring greater accessibility, and facilitating customization. The second facet, the core of the research, delves into the complexities of the proposed architecture as well as the pilot study. Here, we leverage the latest advances in technology, forging a system that combines multi-agent frameworks with context-aware capabilities. This fusion is critical for managing complex information flows and fine-tuning therapeutic exercises to align with the unique needs of each patient. We articulate specific technological pathways, such as the application of miniaturized sensors for motion tracking and the integration of machine learning algorithms for adaptable therapy, which together contribute to the enhanced size and customization capabilities of our system. These innovations represent a significant leap over traditional methods, which often lack this degree of customization and sophistication in data handling and treatment adaptation. To elaborate, our technical route includes detailed algorithmic processes that transform patient data into actionable insights, allowing the device to offer personalized treatment regimes that evolve in real-time with the patient’s recovery trajectory. To validate our proposal, we conducted a pilot study with 10 participants, which included a longitudinal intervention over 4 weeks with structured sessions. The participants, divided into healthy individuals and those with CMC impairments, interacted with a series of games designed to measure and improve CMC in a gamified context, which facilitated the collection of objective data and dynamic treatment adaptation.
This article is structured into several essential sections. Subsequently, Sect. 1.1 details the current methods of therapeutic intervention, and 1.2 discusses technological solutions in the context of research. Section 2 elaborates on the system architecture, and Sect. 3 addresses the methodology used, including participant selection and evaluation procedures, highlighting the pilot study conducted. Section 4 describes the therapeutic intervention and participant interaction with the device during a 4-week study. Key findings and collected data are presented in Sect. 5, followed by the discussion of results in Sect. 6, and the conclusions and recommendations for future research in Sect. 7.
1.1 Therapeutic intervention methods
Cervical Motor Control (CMC) results from the interplay of afferent and efferent information flow and central processing that integrates these two types of information. CMC encompasses the control of head and neck movement, eye movement control, and postural balance. To regulate these functions, CMC relies on multiple subsystems: proprioception, kinesthesia (both responsible for head and neck orientation to the body), the visuomotor system, and the vestibular system [8]. The cervical spine plays a crucial role in postural control and balance. Impairment of proprioception in this area can lead to common conditions such as chronic neck pain [9].
The function of CMC is achieved through the receptors in the cervical spine, which have significant connections to various parts of the central nervous system, such as the visual and vestibular systems. When sensory input is disrupted in these receptors, the entire process is affected due to inadequate information integration. This information can be altered by different mechanisms, including trauma, receptors’ functional impairment, receptor sensitivity changes, and pain’s effects at various levels of the nervous system [10].
Therefore, regulation at the central nervous system level is essential for achieving functional CMC. Continuous sensory information, in conjunction with the vestibular and visual systems, ensures coordinated motor functions throughout the body, maintenance of posture and stability in static and dynamic situations, and a swift neck response to the surrounding environment. In this function, the information collected by muscle spindles in the suboccipital muscles is particularly relevant for fine motor control of posture [11].
Another key element in the CMC process, alongside the musculature and the central nervous system, is the osteoligamentous structures, which provide 20% of cervical mechanical stability. Thus, the synchronization of ligaments as stabilizing factors, muscles responsible for performing movements, and the central nervous system integrating information and making precise adjustments ensure that the neck moves correctly and allows for appropriate postural adjustments to maintain balance [11]. The diagram presented in Fig. 1 illustrates this intricate feedback process among systems. It shows how all the elements that participate in the CMC are interrelated. Proprioceptors and passive structures collect sensory information about the position and movement of the body. These elements are in direct relationship with the muscles, effectors of the postural adjustment and movement response. In addition to these structures, the central nervous system and cervical kinematics act as integrating elements and elaborate the response executed, so they are the elements that will determine the postural and movement adjustments.

Processes involved in CMC.The figure shows the effectors and the relationships between them. The solid line unites the elements that collect sensitive information and execute the motor command. The dashed lines show the relationship with the elements of information integration and movement control
Dysfunction in cervical afferents for these reasons leads to the development of a range of symptoms in patients, such as the onset of dizziness, postural instability, visual disturbances, balance impairment, and altered control of eye, head, and neck movements [12]. Given the intricate process of CMC and its clinical complications, a proper assessment process becomes essential for tailoring patient treatment to optimize outcomes. However, scientific literature indicates that, although various methods exist for assessment and treatment, they all have limitations.
Regarding assessment, numerous CMC evaluation tools have been developed. The most commonly used procedure is the Head Relocation Test (HRT). In this test, a patient wears a helmet with a laser beam, and their ability to recognize head position (proprioception) and the amount of movement (kinesthesia) is assessed [13]. Several studies have employed this test to determine CMC capacity [14, 15]. The test measures the error when repositioning the head to the target. However, while it may appear to be a suitable tool for determining head position, it does not encompass assessing the oculomotor or vestibular systems. Additionally, it relies on analog equipment and can sometimes lack precision. Therefore, despite its widespread use, there is a lack of evidence to support its use as a sole assessment tool, as it has not been validated due to the absence of a gold standard and limited research on extensive populations [8].
The HRT assesses head positioning and kinesthesia but does not evaluate how movement occurs in individuals with Cervical Motor Control (CMC) impairments. Methods such as the continuous linear motion technique, which evaluates movement in cervical rotations, have been designed to overcome this limitation. Another system that enhances the former is The Fly®, which records the movement of a nonlinear trajectory following objects, focusing more on the sense of movement than position. It also incorporates a virtual reality system to display movement targets [13].
The limitations of these systems are that they are better at assessing movement but do not evaluate position. The Fly® improves upon the HRT by incorporating an assessment of the visuomotor system through object trajectory tracking, but it still does not assess the vestibular system [8]. Each measurement system captures a specific CMC aspect but does not provide complete information. This problem poses a challenge for clinicians, as they encounter difficulties selecting an appropriate assessment method. The heterogeneity of tests used in scientific studies also hinders the generalization of results to the population. Furthermore, these methods require wired apparatuses that hinder task execution or large devices that limit mobility.
On the other hand, the treatment of Cervical Motor Control (CMC) impairments is more complex. There are various methodologies, ranging from transcranial magnetic stimulation [16] to education in pain neuroscience [17]. However, motor training appears to be the technique that has demonstrated the most effectiveness, particularly retraining aimed at improving cervical proprioception and coordination [9].
Current studies approach cervical training with motor control exercises combined with other techniques, such as oculomotor exercises, balance exercises [15], motor imagery exercises [18], or sensorimotor incongruity exercises [19].
Considering the background presented, this study aims to design a portable device that enables proper movement and overcomes the limitations presented by other assessment and treatment methods. Furthermore, the goal is to analyze its feasibility and utility in clinical practice.
1.2 Technological solutions
The methods used to address CMC impairments have witnessed significant advancements due to the convergence of modern technologies and healthcare. The introduction of innovative technological solutions has enabled the overcoming some limitations associated with traditional assessment and treatment of CMC.
One of the most notable advancements is the use of advanced motion sensors. These sensors allow for accurate tracking and recording of the patient’s head and neck movements [20]. These sensors [21] can be inertial, such as accelerometers and gyroscopes, which measure acceleration and angular orientation, or camera-based, using images to track position and movement. Sensor technology provides an objective and quantitative assessment of Cervical Motor Control (CMC). By measuring movements in real-time, therapists can identify specific deficiencies and track the patient’s progression throughout treatment. Additionally, collecting objective data reduces subjectivity in assessment, enhancing the accuracy and reliability of results [22].
Another advancement is in Virtual Reality (VR) and Augmented Reality (AR), technologies that have revolutionized the treatment of CMC impairments. These technologies enable the creation of interactive virtual environments that simulate real-world situations or provide real-time visual feedback during therapeutic exercises [23]. Currently, VR is used to design engaging and personalized therapeutic exercises. Patients can engage in virtual activities requiring specific neck and head movements, making training more accessible and enhancing motivation [24]. Furthermore, VR allows therapists to adjust exercise difficulty based on individual patient’s physiological needs. Similarly, patients can see graphical representations of their movements concerning therapeutic goals. This visual feedback aids in correcting improper movements and improves the accuracy and effectiveness of training exercises [25].
Finally, some research uses data analysis and machine learning, including multiagent systems, which enable the processing and interpreting of large datasets generated during CMC assessment and treatment. Data analysis is used to identify patterns and trends in patient movements [26]. Therapists can use these analyses to understand CMC deficiencies better and tailor treatment accordingly. Furthermore, data analysis facilitates tracking patient progress over time [27], which is crucial for assessing treatment effectiveness. All of this is made possible through the capabilities provided by multi-agent systems, including [28] the ability to contextualize scenarios quickly, address uncertainties related to planning and problem-solving, coordinate distributed sources of information, and sophisticatedly control distributed systems. Similarly, their adaptability allows for the personalization of treatment programs [29]. Along with machine learning algorithms, they can analyze patient data and recommend specific exercises and adjustments to address identified deficiencies [30]. These solutions enable a more precise and personalized approach for each patient, maximizing treatment outcomes.
These technological solutions have collectively opened new perspectives in assessing and treating CMC impairments. The limitations of traditional assessment methods, the lack of objectivity in measurement, and the absence of customization in treatment programs have been persistent challenges in caring for patients with CMC impairments.
In this context, the proposed system emerges as a promising response to these needs. Based on sensor technologies, VR, data analysis, and multi-agent systems, the system comprehensively addresses these limitations. It provides an objective and quantitative assessment of Cervical Motor Control (CMC), allows customized treatment programs, and offers real-time visual feedback. In doing so, it improves the accuracy and effectiveness of treatment and provides a versatile and accessible tool for healthcare professionals.
2 Description of system
In the context of CMC assessment and rehabilitation, technology integration has become an area of growing interest. Dysfunction in cervical afferents can lead to debilitating symptoms, emphasizing the importance of developing innovative approaches to address this clinical challenge. This section presents a comprehensive overview of the platform, which encompasses a physical device designed for capturing motion and position metrics during each moment of rehabilitation exercises. The characteristics of the platform’s architecture responsible for data collection and patient progress tracking will also be described.
2.1 System architecture
In the last decade, the development and application of multi-agent systems in rehabilitation and medical monitoring have seen significant growth, showcasing their potential in enhancing monitoring accuracy and therapy personalization. Recent studies like [31], presenting an agent-based health monitoring system utilizing 5G technology for chronic, elderly, and remote patients, demonstrate how these systems aid real-time data collection and dynamically tailor treatments to individual patient needs. Moreover, [32] provides an extensive overview of the applications of agents in healthcare, pinpointing key trends and challenges in merging these emerging technologies. In their systematic review, a pivotal contribution is made by [33], underscoring conversational agents’ nuanced roles in augmenting patient and provider interactions, enhancing adherence, and facilitating remote healthcare delivery. These conversational agents, capable of engaging users in natural language dialogue, extend the capabilities of multiagent systems by offering personalized, interactive support to patients and healthcare professionals alike. Despite the advances achieved, challenges in integrating new technologies, scalability of solutions, and deeper personalization of interventions persist. This research aims to tackle these issues by introducing a novel multi-agent system model that enhances user interaction and broadens the applicability of personalized therapies, marking a significant advancement in the effectiveness of rehabilitation and medical monitoring.
This research presents an innovative architecture designed to address the assessment and treatment needs of CMC impairments. CMC impairments can lead to dizziness, postural instability, and visual problems, highlighting the importance of precise assessment and treatment tools. Available solutions still need the necessary features for comprehensive patient progress monitoring in this field.
The proposed architecture addresses this challenge by implementing an advanced and adaptable platform. This platform utilizes cutting-edge technologies such as the Internet of Things (IoT) and pattern detection to gather essential data related to CMC.
One of the main aspects of this architecture is its ability to dynamically adapt to each patient’s individual needs. We achieve this purpose by integrating a multiagent system adapted to the context-aware framework, allowing for the customization of assessments and treatments based on the characteristics and progress of each individual.
In addition to the precise assessment of CMC, this architecture also incorporates a therapeutic dimension. The results obtained in a pilot study indicate that therapeutic interventions performed with this platform’s assistance can positively impact the accuracy of performance in various CMC tests.
This architectural approach not only focuses on objective assessment but also on improving CMC through personalized therapeutic interventions. More specifically, the proposed architecture can be observed in Fig. 2.

System Architecture
2.1.1 Monitoring organization (MO)
This organization is responsible for managing and controlling the various virtual organizations and agents on the platform, along with the context collected by the other organizations. The agents that make up this organization are:
-
Services Agent (SA): This agent enables the communication of external services with the virtual organization of agents. In this way, it allows for the integration of new agents, as well as virtual organizations, seamlessly. Similarly, it manages system information, enables high-level context analysis, and distributes global system information.
-
Monitor Agent (MA): This agent is responsible for periodically checking the system’s status. It is responsible for detecting information overload, conflicts between agents, component or resource failures, and inconsistencies in agent states.
-
Administrative Agent (AA): This agent is responsible for indicating the services available from all agents that system agents can request. When a new agent wants to join the system, it must inform this agent of the services it provides so that it can determine which services are available to other agents.
-
Timestamp Agent (TA): This agent must include date/time information in the data before storage.
-
Context Reasoner Agent (CRA): This agent aims to produce high-level context information based on the output obtained from the context aggregation organization. Applying pattern recognition techniques enables the determination of the correct execution of the exercise by the patient, their current status, and their progression during the exercise. It also provides a broader context by detecting patterns, irregularities, patient needs, and more.
-
Repository Manager Agent (RMA): This agent manages all the data generated by the system’s organizations. It serves as an interface between applications and other modules with the database, addressing all computational needs related to data privacy and security.
2.1.2 Acquisition organization
This organization plays a crucial role in gathering information about head and neck movement postural balance. This organization aims to provide accurate data for assessing and treating cervical motor control impairments. The agents that are part of this organization include:
-
Accelerometer Agent (AcA): This agent specializes in processing data from the accelerometer component of an IMU. Its primary function is to interpret variations in linear motion and determine the device’s orientation with respect to gravity. By analyzing acceleration patterns, it can ascertain movements like tilting, shaking, or swift changes in direction, ensuring that the IMU captures accurate motion dynamics.
-
Gyroscope Agent (GA): Focused on the rotational aspects of movement, the Gyroscope Agent interprets the angular velocity data derived from the gyroscope. It provides insights into how fast and in which direction the device is rotating. By continuously monitoring these rotations, the agent aids in determining the device’s orientation and any changes to its position in three-dimensional space.
-
Magnetometer Agent (MagA): Operating in tandem with the other sensors, the Magnetometer Agent is responsible for capturing the Earth’s magnetic field data. It essentially functions as a digital compass, helping determine the device’s orientation relative to the North. This agent’s readings, when combined with those from the accelerometer and gyroscope, can offer a comprehensive understanding of the device’s position in the world.
-
Calibration Agent: The accuracy of an IMU is paramount, and the Calibration Agent ensures this by regularly checking the sensor’s outputs against expected values. If discrepancies or drifts are detected, this agent instigates corrective measures, recalibrating the IMU to maintain precision. Its proactive monitoring helps in mitigating errors that could arise from environmental factors or prolonged usage.
-
Sensor Fusion Agent (SFA): As the name suggests, this agent acts as the integrator of data from the accelerometer, gyroscope, and magnetometer. By synergizing the information from these sources, the Sensor Fusion Agent creates a cohesive and enhanced representation of the device’s movement and orientation. This fusion process ensures that the combined output is more accurate and reliable than any single sensor’s readings on its own.
-
Acquisiton Comunication Agent (ACA): It is a central point for integrating data from all the previously mentioned agents. Subsequently, it sends the information obtained from the multiple data sources in the system for context analysis.
2.1.3 Context analysis organization
It carries out the interpretation of the data collected by the Acquisition Organization and the identification of patterns that can help understand CMC impairments and guide the treatment. More specifically, the agents belonging to this layer are as follows:
-
Preprocessor Data Agent (PDA): This agent exists as a preliminary step before feature extraction and context management. It is responsible for gathering information from interdependent devices and unifying the data received from them. It also filters the data, validating and correcting it if necessary.
-
Feature Extractor Agent (FEA): This agent is responsible for characterizing the raw information received, which allows it to identify the user and their environment. Specifically, this component identifies the movements captured by the motion sensors. It also identifies other features, such as posture and coordination.
-
Context Classifier Agent (CCA): This agent is responsible for classifying the previously extracted features, resulting in mid-level information. To do this, it will combine the extracted features, and by using time series algorithms, it will be possible to detect abnormal patterns such as uncontrolled movements, tremors, or restrictions in the range of motion of the head. It also analyzes postural stability and looks for patterns of imbalance or unusual responses to balance tests.
2.1.4 Applications organization
This organization is responsible for interacting with the developed system and users, including healthcare professionals and patients. The agents that make up this organization are as follows:
-
Healthcare Professional Interface Agent (HPIA): It focuses on providing a user interface specifically designed for healthcare professionals, such as physiotherapists and doctors. It allows users to record patient data, access assessment results, and track treatment progress. Additionally, it provides data visualization tools and graphs to assist professionals in making informed treatment decisions.
-
Patient Interface Agent (PIA): It focuses on patients, providing a user interface to participate in the assessment and treatment of CMC. It offers a user-friendly interface that guides patients through the prescribed tests and exercises in a virtual environment. It provides real-time feedback during treatment sessions, such as visual and auditory instructions, to ensure that patients perform the correct movements and follow the guidelines effectively.
-
Data Visualization Agent (DVA): It focuses on presenting data clearly and understandably for healthcare professionals and patients. It offers interactive charts, tables, and visual representations that display the patient’s progress over time. This agent helps users better visualize the results and the evolution of CMC impairments.
-
Communication and Notification Agent (CNA): It allows communication between healthcare professionals and patients through the platform. It enables the exchange of secure messages and important notifications, such as appointment reminders, treatment updates, or patient progress feedback. This communication feature enhances collaboration and treatment monitoring.
2.1.5 Personalization and therapeutic intervention organization
This organization is responsible for adapting tests and treatments to the individual needs of patients, as well as providing continuous monitoring to improve patient function. This organization includes specialized agents that work together to ensure a highly personalized assessment and treatment experience. They also execute personalized treatments and monitor the progress of patients. The agents that make up this organization are:
-
User Profiling Agent (UPA): It is responsible for collecting and analyzing each patient’s medical history, cervical injury history, and previous CMC test results. It uses this data to create a unique profile for each patient, enabling effective customization of tests and treatments.
-
Personalization and Adaptation Agent (PAA): It uses the information collected by the other agents to personalize the tests and treatments. It adjusts the difficulty of the tests based on the patient’s skill level and tailors therapeutic interventions to individual needs. This agent aims to optimize the effectiveness of the assessment and treatment.
-
Treatment Planning and Scheduling Agent (TPSA): It is responsible for designing individualized treatment plans for each patient, considering their profile and needs. This agent also schedules therapeutic sessions and ensures that patients follow them efficiently.
-
Therapeutic Session Execution Agent (TSEA): It is involved in the execution of the planned therapeutic sessions. It provides instructions and guides the patient through the specific therapies designed to address CMC alterations.
-
Outcome Evaluation and Reporting Agent (OERA): It is responsible for assessing the long-term treatment results. It generates detailed reports on the patient’s progress over time and contributes to decision-making regarding the continuation or modification of therapies.
-
Progress Monitoring and Adjustment Agent (PMAA): It performs ongoing monitoring of the patient’s progress during treatment. It uses data collected during therapeutic sessions and makes real-time adjustments to treatment plans when necessary to achieve the best results.
Regarding agent communication, the designed architecture utilizes the AMQP (Advanced Message Queuing Protocol) [34]. This open and standardized messaging protocol offers advanced message routing and queuing features, simplifying robust and real-time communication implementation. Furthermore, with multiple broker implementations and libraries available, it can be employed for agent communication across different environments, as with this platform.
On the other hand, the system employs various databases for its proper operation and scalability. The system utilizes the database within the monitoring organization to store information about the system’s agents, the services each one provides, and the tasks each agent can perform. It also stores context-related information for each patient, as determined by the organization’s agents. Additionally, the system has an additional database to store specific information related to the case study.
This multiagent architecture provides a collaborative and highly adaptive solution for assessing and treating Cervical Motor Control. The agents work together within virtual organizations to ensure personalized and coordinated care for each patient. This characteristic enhances the accuracy of assessments and the effectiveness of therapeutic interventions, thereby improving the patient’s cervical motor control health.
2.2 Device
In rehabilitative medicine and motor control assessment, the evolution and application of sensor technologies, particularly Inertial Measurement Units (IMU), have ushered in a new era of precision and personalization. The intricate dance between technology and healthcare has led to significant strides in understanding and treating motor impairments, evidenced by groundbreaking research.
A pivotal study [35] delves into the kinematic analysis of 360-degree turning in stroke survivors, utilizing wearable motion sensors to capture the nuanced movements often overlooked by traditional assessment methods. This research underscores the capability of modern sensor technology to provide detailed, dynamic insights into patient mobility and the effectiveness of rehabilitative strategies.
Similarly, the research [36] has systematically reviewed the use of wearable IMU sensors in individuals with spasticity, highlighting the vast potential of these devices in enhancing the diagnostic process and monitoring progressive treatment outcomes. These investigations demonstrate the practical applications of IMU sensors in addressing specific motor impairments and illustrate the broader implications of sensor technology in revolutionizing patient care.
Integrating IMU sensors into clinical practice represents a significant leap forward, enabling clinicians to gather real-time data on patient movement patterns with unprecedented accuracy and granularity [37]. Beyond stroke and spasticity, this technology holds promise for many conditions, offering a window into the patient’s functional abilities and limitations. As we continue to harness the power of advanced sensor technologies, the next frontier involves the development of sophisticated analytical models capable of deciphering the complex data streams these devices generate. The goal is to craft personalized, adaptive interventions that respond to each patient’s unique needs, thereby enhancing the efficacy of rehabilitation efforts.
The focus of this proposal lies in a physical device specifically designed to capture cervical movements precisely. This device is based on a microcontroller with an ESP32 chip and inertial sensors (IMUs).
Regarding the device, its ergonomic design is worth noting. The device is small and lightweight to be comfortable for patients. Although the device is designed for the head, it can be used on other body parts to treat other conditions due to its adjustable strap. Figure 3 illustrates the developed device.

Developed device; a side view; b top view
The main component of the device is the MPU6050 inertial sensor. This compact device combines a six-axis accelerometer and gyroscope, allowing it to measure various movements and orientations in three-dimensional space. The accelerometer detects linear accelerations in three directions, providing information about how the patient’s neck moves in terms of acceleration and deceleration along different axes. On the other hand, the gyroscope measures angular rotation speeds along those same axes, offering a detailed view of the speed and direction of cervical movements.
The ESP32 can fuse the data captured by the accelerometer and gyroscope. This data fusion combines the advantages of both sensors and corrects their respective.
limitations. For example, the gyroscope may suffer from drift over time, while the accelerometer may be affected by noise. By fusing the data, we obtain a more accurate and stable measurement of head and neck movements in all directions. This technique is important for precise assessment and the design of specific rehabilitation exercises. The MPU6050 inertial sensor, with its adjustable sampling frequency set to 500.
Hz for our study, coupled with its high measurement precision, ensures the collection of a reliable dataset crucial for the detailed understanding of cervical kinematics. The high-frequency data capture allows for a more nuanced analysis of movement patterns, making the information gathered by this sensor invaluable for accurately assessing the patient’s condition. These detailed data are essential not only for evaluating the patient’s cervical motor function but also for tailoring rehabilitation exercises to meet their specific needs, ensuring that therapeutic interventions are both precise and effective.
The device is portable and practical, powered by a battery that ensures unrestricted operation during assessment and rehabilitation sessions. One of its standout features is its automated calibration process. When we initialize an exercise, the device performs an automatic calibration that adapts to the initial conditions and the patient’s position. This feature always guarantees precise and consistent measurements.
Bluetooth communication enables the instant transfer of motion data captured by the inertial sensor to other devices, such as computers or mobile devices. This type of communication adds versatility to the device, deleting intermediary cables.
The portable device allows patients to carry it without difficulty both within and outside the clinical environment. Due to its size, it would be possible for patients to take it with them to perform assessments and exercises at home.
It is worth noting that the information captured by the MPU6050, once filtered, and fused, is presented in the form of quaternions (see Fig. 4), a mathematical representation of orientation in three-dimensional space. Quaternions provide an accurate and efficient description of the device’s orientation in real time, which is essential for assessing cervical movements accurately. Through quaternions, we obtain linear accelerations and angular rotation velocities in different axes, allowing a detailed understanding of the patient’s neck movements.

Capture data, filter and data fusion
A data fusion process combines readings from the accelerometer and gyroscope to distinguish movements and understand cervical kinematics. This data fusion leverages both sensors’ strengths and corrects their limitations. For instance, while the gyroscope may experience drift over time, the accelerometer can be affected by noise. Data fusion ensures more accurate and stable measurements, crucial for precise assessment and customization of rehabilitation exercises.
The information collected through quaternions is not only essential for assessing the patient’s condition but also crucial for designing specific rehabilitation exercises. This information is integrated with the virtual scenarios used in therapy, creating an interactive and personalized rehabilitation experience. Quaternion data tracks the patient’s movement in the virtual environment and provides real-time feedback.
To collect the data necessary accurately and reliably for our research on cervical kinematics, it is essential to highlight the strategic placement of the device. It is positioned directly on the patient’s forehead, allowing for optimal capture of neck movements and orientations in three-dimensional space. The choice of this location ensures the device’s stability during evaluation and rehabilitation activities, minimizing interference with the patient’s natural movement and maximizing the quality of the collected data. This methodology underscores our commitment to generating a reliable and high-quality data set to properly assess the patient’s condition and effectively customize rehabilitation exercises.
2.3 Exercises
The platform features two main categories of exercises, each designed to collect crucial metrics related to the patient’s positions and accelerations. All metrics are recorded at a sampling frequency of 100 Hz, ensuring accurate and detailed data capture.
The first type of exercise presents the patient with a challenge involving navigating a virtual course. On the screen, the platform projects a course that can be customized. Alongside this course, it displays a pointer controlled by the device held by the patient. The task is to use this pointer to complete the course, which extends from a starting point to an endpoint within the virtual environment. During the course execution, crucial metrics are captured, such as the time required to complete it, the average deviation from the desired path, and the maximum deviation from the course.
The customization of the courses on the platform is a crucial feature that provides flexibility for healthcare professionals to tailor the platform to patients’ individual needs. In this context, virtual courses can be configured in multiple ways to offer a personalized rehabilitation experience. Besides the type of course, whether linear or curved, the platform allows adjusting the width of the course, adding an extra level of customization. Courses can be narrower to challenge the patient’s precision and coordination or wider to focus on the range of motion and fluidity.
The second type of exercise challenges the user to keep the pointer, controlled by the device, within a target. These exercises focus on assessing and improving the user’s ability to maintain a specific position for a set period and determine the maximum deviations from that point. The exercises can be performed with the target in a stationary or mobile position, adding an extra challenging component.
In the case of a moving target, there is customization in the path it can follow. This exercise includes settings for linear, circular, or accessible movement paths and the ability to adjust the speed of the target’s movement. This variety of options allows us to tailor exercises to each patient’s specific needs and progress in cervical motor control.
The collected data provides valuable information about the patient’s movement accuracy and speed, contributing to the evaluation and monitoring of cervical motor control rehabilitation.
3 Description of methodology employed
3.1 Participants
A pilot study was conducted with the device to determine its feasibility and usability. A total of 10 participants were involved, who completed various games offered on the platform. The sample was chosen for convenience and included five healthy participants and 5 participants with CMC impairments due to various reasons:
-
Two participants had whiplash-related issues.
-
Two participants had chronic nonspecific cervical pain.
-
One participant had sequelae from cerebral palsy with CMC impairment.
The sample was made up of 5 men and 5 women. In the group with pathology, there were 3 men and 2 women. In the healthy group, the sample was made up of 2 men and 3 women. The average age of the sample was 40.6 years. The average height was 1.69 m, and the weight was 69.9 kg, so the average body mass index was established at 24.5 kg/m2. This value establishes that the sample was within the normal weight range.
The present study adheres to the ethical principles of the Helsinki Declaration. All participants were informed about the study’s objectives and the intervention to be conducted and provided informed consent before any interventions.
3.2 Design
A prospective longitudinal intervention study was conducted with the participants to determine the effect of an intervention on the usability and feasibility of the device developed as an intervention tool for treating CMC in patients.
Once the participants were included in the study, their CMC was assessed in various tests under different conditions.
3.3 Assessment
We used the HRT (Head Repositioning Test), Fig. 5, as the objective test. To perform it, each participant was seated with their head and neck in a neutral position and their hands resting on their legs. In front of them, we placed a board with four squares one meter away from the participant. Each square represents a 30º rotation to each side, a 25º flexion, and a 25º extension. The central point of each square was marked with a 5 mm diameter circle. A laser attached to a tape was placed on the participant’s head and guided them to the center of each square. After reaching the center, the participant had to close their eyes and return to the starting position as accurately as possible. Several test attempts were made until the participant understood the task, and finally, the deviation from each position (flexion, extension, and rotation) to the starting point was measured [38].

CMC assessment with the HRT (head relocation test)
Furthermore, the system, along with the proposed architecture, was used to determine if the developed device can serve as a tool to assess patients’ progress after therapeutic intervention. We considered that both would assess different CMC components for selecting these games. Therefore, one game with a fixed background and another with a moving background were selected. Additionally, both games had moderate difficulty challenging participants without being excessively difficult, ensuring that all participants could complete the test.
Regarding the section on CMC evaluation with a fixed background, we used the first type of game on the platform, which includes fixed circuits that the participants must complete. This game assesses the ability to make precise movements in all directions while trying to follow a path without deviation. This is one of the challenges faced by people with CMC disorders, making it highly relevant to determine the participants’ capacity to complete a task with these characteristics.
Once the type of task was determined, the first circuit within this game was selected due to its requirement for movements in all directions, including flexion, extension, and rotation. It was the most homogeneous circuit in terms of the movements required. The difficulty level of the game was also taken into account. A pilot test was conducted among the participants to determine a level at which they could all complete the circuit satisfactorily but would still make errors. This pilot test allowed the participants to practice and avoid the potential effects of subsequent training on the results. Consequently, the participants showed the training effect in the initial and final assessments.
To align the test with the HRT, the participants sat in a chair with their backs straight and necks in a neutral position, with their hands on their legs. They positioned one meter away from a television screen where the game was projected, placing the device in the middle of their forehead. In this position, the game was calibrated to determine the initial position, set at level 3 of circuit 1 in the first game (Fig. 6). We asked them to complete the circuit from the initial point to the end at an appropriate speed while trying not to leave the green-colored area. The time spent correctly completing the circuit, the time spent outside of it, the number of errors made, and instances of leaving the circuit, as well as the maximum distance they traveled during these errors, were recorded.

Evaluation of the CMC with the circuit belonging to the first set of the device
The last assessment test also used the developed device, but a test with a moving background was employed this time. For this test, we used the system’s second type of game, where targets appear, and the participant’s goal is to keep the reference point within the center of the target. In this test, the objective was to determine if the participant could track a moving background, which requires a strong CMC since it demands that the participant adapt their movements to the speed set by the test. We discarded the stationary target because the goal was to track a moving background. To choose the test that best determined the ability of our participants, a pilot test was carried out with all of them to determine the test that best discriminated their situation. Once again, this pilot test was used to prevent the training effect from interfering with the study’s results.
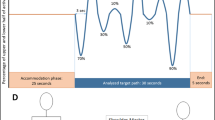
After conducting this pilot test, we determined that the assessment with a moving background should be performed outside, within the second game (Fig. 7), with the horizontally moving target. Considering the average time taken to complete the circuit in the previous test and aiming for a similar time, we used a recording time of 20 s, and the difficulty level was set at 3. Participants were placed in the same position as in the previous test, and the developed device was calibrated to start in the middle position. Once the participants moved the mark to the center of the target, it began moving horizontally, from side to side. We asked the participants to try to keep the mark within the center of the target, which required them to make rotational movements in both directions.

Evaluation of the CMC with the second set of the device
4 Intervention
After assessing the participants, the intervention with the developed platform to improve their CMC began. Before conducting the intervention, we instructed participants on how to use the device, the steps to follow, and the importance of carrying out the intervention as specified. We provided them with an instruction booklet detailing all the intervention steps. The participants went to a room set up for the intervention at the University of Salamanca. In this room was a television connected to a computer where the program for the various games was projected. Participants were responsible for handling all the elements (television, mouse, and device) under the supervision of the research team members. Once the device was in place, the participants stood on a mark located one meter from the television, and if they needed assistance, they could request it at any point in the process. The television was positioned on a stand to ensure it was at eye level to properly adjust the device’s calibration and work on the cervical movements as accurately as possible.
4.1 Procedure
The participants completed 12 sessions, with a frequency of three sessions per week, spanning four weeks. In each session, the participant was required to complete each proposed game three times. The system adjusted the difficulty level of the games based on the participant’s progression. Participants were instructed to conduct training sessions on alternate days to achieve the three weekly sessions, typically on Mondays, Wednesdays, and Fridays, ensuring at least one day of rest between sessions. They were advised to perform the standing exercises to challenge their CMC from a more demanding position than sitting.
In the circuits proposed for evaluation, in the case of the first game, the instruction was that completing it without errors was the primary goal. Participants were advised to adjust their movement speed to complete the circuit without leaving the green-colored area. This game was completed by the participants who achieved the best performance up to level 5, but none of them completed this level without making some errors along the way.
For the targets in the second game, participants were instructed to try to adapt to the moving target as accurately as possible. In the case of the game with the fixed target, the goal was to keep the marker inside the target with their eyes closed, so the participant had to position the marker in the center and then close their eyes, attempting to maintain the posture without errors. This game is especially relevant for CMC disorders because, in addition to difficulties with precise movements, problems with maintaining posture are common due to the impact on the postural tonic musculature. Participants with greater skill could reach level 4 in the moving horizontal and vertical targets, level 5 in the stationary target, and level 3 in the circular moving target without making errors. These levels were reached without surpassing the next level.
In addition to the instructions for the various interventions, the importance of taking breaks between each game was emphasized. This reason is critical to prevent muscular fatigue from interfering with the intervention’s performance. Excessive muscular fatigue is a sequela of individuals with CMC disorders when performing tasks. All participants were instructed to rest their necks, relax, or move them fluidly for 15 or 20 s after each game to prevent interference from fatigue.
The approximate time spent in each session was about 20 min, with 10 min dedicated to playing the games, 5 min for transitioning between games, and the remaining 5 min used for breaks between games.
Participants had a weekly interview with the research team to report on the intervention’s progress. They provided information about possible technical issues addressed to ensure they did not disrupt the intervention. Participants also shared any difficulties encountered during the exercises and asked questions about the progression clarified during the interview. Additionally, they shared their overall experience, which was generally positive. All participants reported a high level of motivation, expressed interest in continuing with the intervention, and, in some cases, even mentioned that the session felt short and that they would have liked to do it longer.
After completing the intervention, we conducted a final assessment to determine the effect of the intervention. To do this, they repeated the tests during the initial evaluation, and the values were recorded after completing the intervention.
4.2 Statistical analysis
After collecting the data from the two assessments, an analysis of this data was carried out. We used the IBM Statistics SPSS program, version 28, for the statistical data analysis. Initially, an analysis of the data obtained from all participants was conducted. Then, the data from each group (individuals with cervical motor control impairments and healthy individuals) were analyzed separately. The mean value and standard deviation for each test were recorded for all groups and the overall assessment of the participants. After the results, we conducted an inferential analysis. Non-parametric tests were used due to the small sample size, as this was a feasibility pilot study of the device. The Wilcoxon signed-rank test was used to determine the effect in each group after the intervention.
Additionally, the differences obtained in each test before and after the intervention were calculated, and intergroup differences were determined using the Mann–Whitney U test. Finally, to determine whether the tests performed with the device could be comparable to a validated test for cervical motor control assessment, correlations were examined between the different tests using Spearman’s correlation. These tests were conducted with a 95% confidence and significance levels of α = 0.005.
5 Results
As shown in Table 1, all participants in the sample completed the intervention and underwent the final evaluation. In all tests used to assess CMC, a positive change was observed after the intervention in both groups and the overall sample considered.
In the HRT, we observed that the movements that benefited the most from the intervention were cervical flexion and right rotation, where, after completing the intervention, a minor deviation with a higher mean value was observed. The movement with the least difference was cervical internal rotation, where the deviation value changed by only 0.1 degrees. When looking at the groups in this same test, we observed that the group with cervical pathology showed the most significant difference after the intervention, as there was a substantial change in all movements except for left rotation, where the change was smaller. In the group of healthy individuals, we observed minor changes, maintaining similar values, with a slight decrease in deviation in all of them.
Regarding the evaluation carried out with the developed device while maintaining a fixed background and asking the participant to move their neck to complete the proposed circuit, a global observation revealed that the time the participant took to complete the test was reduced. Both the time spent inside the circuit and the time spent outside decreased. The number of errors decreased to less than half after completing the intervention. Additionally, the maximum deviation in one of the errors decreased by nearly half, resulting in a maximum deviation of only 0.14 cm.
In this same test, the performance of participants with CMC disorders improved after the intervention. The average time they took to complete the circuit in the test decreased by almost two seconds. The time the participant spent outside the circuit was reduced, and the number of errors too. They also exhibited a lower maximum circuit deviation, with a 0.15 mm difference between the beginning and end of the intervention.
The differences found in this test were more significant in the group of healthy participants. The average time they needed to complete the test was three seconds less. The time spent outside the circuit was reduced to less than a second, and the average number of errors was less than two, halving the average value obtained before the intervention. The maximum circuit deviation after completing the intervention was less than 1 mm.
When analyzing the evaluation conducted using the developed device with a moving target that participants had to track for 20 s, we found that the results were consistent with the other two tests. Overall, the results were satisfactory, as the participants demonstrated that they could stay within the target longer. The time they made errors was reduced by up to two seconds (10% of the total test time). The number of errors decreased by three points, and the maximum deviation from the target decreased by 1 cm.
In this same test, the group with cervical pathology demonstrated an increased ability to stay within the target for a longer duration, reducing their average number of errors to almost half, decreasing from nearly 12 to 6 errors. The values obtained for the maximum deviation from the target were lower, although not statistically significant. Conversely, in the group of healthy individuals, the performance in this test significantly improved by the end of the study. They showed the capacity to correctly perform the task for nearly two seconds longer than at the beginning of the study, reducing their average number of errors by threefold, decreasing from 7 to 2 errors, and the maximum deviation from the target decreased by almost two centimeters.
While both groups improved in the measured parameters, it was observed that the difference in the number of errors was more remarkable for the group of individuals with cervical motion disorders in the assessment with a fixed background, and the improvement was more evident in the group of healthy individuals in the assessment with a moving background.
When conducting an inferential analysis of the results, the following was observed (Table 2):
In the HRT test, statistically significant values were only found in the group of individuals with CMC alterations to compare post-intervention and pre-intervention values in the extension movement. In all other cases, the values were not statistically significant.
The most significant statistical differences were found in the CMC assessment using the developed device with a fixed screen background. We observed significant values in both groups in the number of errors between the beginning and the end, which decreased in both groups. In the group of healthy individuals, these differences were also observed in the time they spent inside the circuit, which was longer than at the beginning of the study. Furthermore, in this test, significant differences were found between the two groups when analyzing the differences in both the time spent inside the circuit, with the group of healthy individuals showing a more significant difference, and in the number of errors, in which case, the group of individuals with pathology showed a greater difference.
Finally, in the assessment test using the developed device with a moving screen background, differences were found in the number of errors between the beginning and the end in both groups, with fewer errors in both cases. Additionally, we observed a significantly shorter time outside the circuit at the end of the study in the group of healthy individuals. No statistically significant differences were found when analyzing the intergroup data.
In the analysis of correlations between the various assessment tests, the following results were found (Table 3):
The test of the developed device with a fixed background, completing a circuit, showed statistically significant correlations between its different recorded aspects. Thus, an inverse correlation was found between the time inside and outside the circuit, the time inside the circuit and the errors, and the time inside the circuit with the maximum deviation that occurred during the test. When analyzing data pairs, there was a direct correlation between the time outside the circuit, the number of errors produced, and the maximum deviation reached.
In addition to the correlations found within the same test, statistically significant correlations were found with the rest of the tests. When comparing this test with the HRT, the most commonly used test to assess the CMC, we found a significant direct correlation between the time participants spent making errors and the extension, right rotation, and left rotation parameters of the HRT. There was also a significant direct relationship between the number of errors during the circuit test and the extension and left rotation parameters of the HRT.
Regarding the test performed with the developed device with a moving background, that is, keeping the mark inside the target, it was observed that there was a statistically significant correlation between its different aspects, except for the maximum deviation produced. We found an inverse correlation between the time spent inside the target and the time spent outside and the number of errors during the test. The number of errors correlated directly with the time spent outside the target.
This test demonstrated that the number of errors made in the target test had a statistically significant and direct correlation with all the parameters assessed in the HRT. Within the HRT test, the only parameters that showed a statistically significant and direct relationship were extension and flexion.
6 Discussion
This study demonstrates the platform’s feasibility and the device’s utility as an assessment and treatment tool for individuals with CMC disorders of various causes. Regarding the effectiveness of this device for treating these disorders, we observed that a 4-week intervention is sufficient to improve CMC in healthy individuals and those with pathology. All the variables studied improved in both groups at the end of the study, indicating that the device positively affects the neck. If we look at the results obtained with the HRT, they show that the component of movement that benefited the least from this training was internal rotation. This benefit may be because, especially in the first game, the component is worked on the least. The circuits were designed to be performed from left to right, so except for the initial movement to start the circuit, the rest of the time, the other components are worked on more specifically. This can be a simple limitation in designing new circuits following the reverse direction.
When using the assessment test with a fixed background on the device, we found that participants quickly made fewer errors, and the errors they did make were less significant. The training effect improved both groups, with better results in terms of the number of errors for participants with CMC disorders.
On the other hand, when applying the test with a moving background, healthy participants showed better results in the number of errors made. This may be because, in this type of test, the fact that the background is in motion involves the oculomotor system and contributes to cervical motor control. This task may require less effort in healthy individuals than in those with CMC disorders. Even though the visual system may not be specifically affected, disruptions in other sensory information can complicate the task for those with CMC disorders. For this reason, this type of test becomes an ideal tool for assessing healthy individuals or individuals with minor cervical abnormalities.
Nonetheless, despite the differences observed in both tests, all the collected values improved at the end of the study. Therefore, although the number of errors was the only statistically significant value in both groups, the failure to achieve greater differences may be due to the small sample size characteristic of the type of study conducted.
When evaluating the device as an assessment tool, we observed that the two tests conducted were consistent, and the provided values correlated. As a future line of research, we propose expanding the study and undertaking a validation process. Suppose the results align with the current findings. In that case, choosing the test value that provides the most information might be possible, thus reducing data collection time and the number of study variables.
The most significant finding for us was the correlation between the number of errors in the test with a moving background, which appears to have a strong relationship with the HRT. In this regard, it would be interesting to conduct a validation study to determine if they have the same reliability and sensitivity [13]. If so, the developed device assessment is more straightforward, quicker, and easier to administer. It is also more engaging and understandable for patients. All of these are clinical advantages that should be considered. Furthermore, the provided values are much more precise than those from the HRT, allowing for greater objectivity in assessing a patient’s condition and tracking even minor changes in their progress.
Undoubtedly, one of the significant advantages of this device is its compact size and portability. Participants reported that it did not cause any discomfort, and after a few minutes of wearing it, they hardly noticed it was there. This allowed participants to move freely without their posture or mobility being affected by the device.
This is also achieved with tools like Motion Guidance [39]. However, data recording with analog devices becomes a process that involves a high degree of subjectivity. The records are manual and approximate. In contrast, the developed device provides all this information with high precision, digitally, and with easy access to the data.
Furthermore, another advantage it offers is the ability to adjust the exercise difficulty progressively and automatically according to the patient’s functional status. This means participants could use it independently at home and supplement their therapy with the device.
The most prominent aspect highlighted by the participants was its interface. The fact that it is designed as a game distracts the participants from being in therapy and immerses them in the gaming experience. Everyone reported high satisfaction with the program, high motivation when using it, and a willingness to continue if necessary. This makes the developed device a highly viable element for use in clinical practice.
Finally, it is important to highlight the growing importance of Inertial Measurement Units (IMU) in assessing the range of motion and diagnosing movement disorders. Specifically, studies like [40, 41] have conducted their research in a context like ours, reinforcing the relevance of our investigations in this field. The study [40] provides evidence of the reliability and validity of IMUs in measuring cervical range of motion, establishing a solid foundation for their clinical application. Study [41] extends this application to a specific context of patients with cervical dysfunction, showing how IMUs can capture functional limitations in daily life. Our study builds on this foundation, further exploring the accuracy of IMUs across a broader spectrum of movement disorders, highlighting both the capabilities and limitations of this technology.
Comparing these works, it is evident that while the accuracy and applicability of IMUs in movement evaluation have been widely demonstrated, the specific context of use (e.g., populations with specific conditions like CMC disorders) can significantly influence the findings. Our study adds to this discussion by examining how these contextual differences affect the interpretation of IMU data and its relevance for diagnosis and treatment. Study [40] focused on the detailed evaluation of the cervical range of motion in a healthy population, showing the reliability and validity of IMUs. Study [41], on the other hand, explores functional limitations in patients with cervical pathology, revealing how IMUs can capture significant differences in ROM during daily activities. Our study contributes to this conversation by assessing the effectiveness of IMUs in a wider spectrum of movement disorders, highlighting both the universality and limitations of this technology in various clinical contexts. This discussion reinforces the idea that although IMUs are powerful tools for movement evaluation, their application must be carefully considered based on the specific clinical context and patient needs. This discussion highlights the need to adapt IMU technology to the clinical context and specific characteristics of the patient, a fundamental principle in our study. By comparing the methodological approaches and outcomes of [40] and [41] with ours, we emphasize how each study contributes to a deeper understanding of IMU application in movement disorder evaluation. This comparison not only underscores the validity and utility of IMUs in various contexts but also emphasizes the importance of ongoing innovation and the development of more precise and adaptive measurement techniques. Aligning with these previous research efforts and extending their application, our work proposes future directions for research and clinical practice, supporting a more personalized and contextualized use of IMU technology in diagnosing and treating movement disorders, paving the way for significant advancements in the field.
7 Conclusions and future work
The present study has demonstrated the feasibility and utility of the developed device as an effective instrument for assessing and treating individuals with Cervical Motor Control (CMC) impairments of various causes. One of the most notable advantages of the device is its size and portability. Participants reported that they did not experience discomfort and practically forgot they were wearing the device after a few minutes of use. This result allowed them to maintain their freedom of movement without restrictions. Data recording with analog devices, such as Motion Guidance, often involves high subjectivity and approximate manual records.
In contrast, the developed device provides high-precision digital and accessible information. Another significant advantage is the ability to automatically adjust the exercise difficulty based on the patient’s functional status. This allows patients to use the device autonomously in their homes, thereby complementing their therapy. Participants highly praised the platform’s interface. The gamification approach allowed patients to immerse themselves in the experience without feeling like they were receiving therapy. The high levels of satisfaction, motivation, and willingness to continue using the device make it a promising tool for clinical practice implementation.
In future lines of work, expanding the study and undergoing a validation process to consolidate the findings is suggested. The correlation between the test with moving background and the HRT should be further explored to determine its reliability and sensitivity. The development of new circuits that include reverse movements to address the observed limitation in left rotation could also be considered.
Availability of data and material
No datasets were generated or analysed during the current study.
References
Kazeminasab, S., Nejadghaderi, S.A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M.J., Kolahi, A.-A., Safiri, S.: Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 23(1), 1–13 (2022)
Grazioli, E., Tranchita, E., Borriello, G., Cerulli, C., Minganti, C., Parisi, A.: The effects of concurrent resistance and aerobic exercise training on functional status in patients with multiple sclerosis. Curr. Sports Med. Reports 18, 452–457 (2019). https://doi.org/10.1249/JSR.0000000000000661
Peng, B., Yang, L., Li, Y., Liu, T., Liu, Y.: Cervical proprioception impairment in neck pain-pathophysiology, clinical evaluation, and management: a narrative review. Pain Ther. 10, 143–164 (2021)
Kumar, S., Ravella, U.K., Shrivastava, A.K., Anil, M., Swamy, S.K.: A review on human cervical fatigue measurement technologies and data analysis methods
Du, Q., Bai, H., Zhu, Z.: Intelligent evaluation method of human cervical vertebra rehabilitation based on computer vision. Sensors 23(8), 3825 (2023)
Chen, K.B., Sesto, M.E., Ponto, K., Leonard, J., Mason, A., Vanderheiden, G., Williams, J., Radwin, R.G.: Use of virtual reality feedback for patients with chronic neck pain and kinesiophobia. IEEE Trans. Neural Syst. Rehabil. Eng. 25(8), 1240–1248 (2016)
Mihajlovic, Z., Popovic, S., Brkic, K., Cosic, K.: A system for head-neck rehabilitation exercises based on serious gaming and virtual reality. Multimed. Tools Appl. 77, 19113–19137 (2018)
Zoete, R.M.J., Osmotherly, P.G., Rivett, D.A., Snodgrass, S.J.: Seven cervical sensorimotor control tests measure different skills in individuals with chronic idiopathic neck pain. Braz. J. Phys. Ther. 24(1), 69–78 (2020). https://doi.org/10.1016/j.bjpt.2018.10.013
Peng, B., Yang, L., Li, Y., Liu, T., Liu, Y.: Cervical proprioception impairment in neck pain-pathophysiology, clinical evaluation, and management: a narrative review. Pain Ther. 10(1), 143–164 (2021). https://doi.org/10.1007/s40122-020-00230-z
Treleaven, J.: Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man. Ther. 13(1), 2–11 (2008). https://doi.org/10.1016/j.math.2007.06.003
Qu, N., Tian, H., De Martino, E., Zhang, B.: Neck pain: do we know enough about the sensorimotor control system? Front. Comput. Neurosci. (2022). https://doi.org/10.3389/fncom.2022.946514
Treleaven, J.: Dizziness, unsteadiness, visual disturbances, and sensorimotor control in traumatic neck pain. J. Orthop. Sports Phys. Ther. 47(7), 492–502 (2017). https://doi.org/10.2519/jospt.2017.7052
Michiels, S., Hertogh, W.D., Truijen, S., November, D., Wuyts, F., Heyning, P.V.: The assessment of cervical sensory motor control: a systematic review focusing on measuring methods and their clinimetric characteristics. Gait Posture 38(1), 1–7 (2013). https://doi.org/10.1016/j.gaitpost.2012.10.007
De Pauw, J., Mercelis, R., Hallemans, A., Michiels, S., Truijen, S., Cras, P., De Hertogh, W.: Cervical sensorimotor control in idiopathic cervical dystonia: a cross-sectional study. Brain Behav. 7(9), 00735 (2017). https://doi.org/10.1002/brb3.735
Sremakaew, M., Jull, G., Treleaven, J., Uthaikhup, S.: Effectiveness of adding rehabilitation of cervical related sensorimotor control to manual therapy and exercise for neck pain: a randomized controlled trial. Musculoskelet. Sci. Pract. 63, 102690 (2023). https://doi.org/10.1016/j.msksp.2022.102690
Qu, N., Tian, H., Martino, E.D., Zhang, B.: Neck pain: do we know enough about the sensorimotor control system? Front. Comput. Neurosci. (2022). https://doi.org/10.3389/fncom.2022.946514
Malfliet, A., Kregel, J., Coppieters, I., Pauw, R.D., Meeus, M., Roussel, N., Cagnie, B., Danneels, L., Nijs, J.: Effect of pain neuroscience education combined with cognition-targeted motor control training on chronic spinal pain. JAMA Neurol. 75(7), 808 (2018). https://doi.org/10.1001/jamaneurol.2018.0492
Hidalgo-Peréz, A., Fernández-García, Á., López-de-Uralde-Villanueva, I., Gil-Martínez, A., Paris-Alemany, A., Fernández-Carnero, J., La Touche, R.: Effectiveness of a motor control therapeutic exercise program combined with motor imagery on the sensorimotor function of the cervical spine: a randomized controlled trial. Int. J. Sports Phys. Ther. 10(6), 877–892 (2015)
Don, S., De Kooning, M., Voogt, L., Ickmans, K., Daenen, L., Nijs, J.: The effect of visual feedback of the neck during movement in people with chronic whiplashassociated disorders: an experimental study. J. Orthop. Sports Phys. Ther. 47(3), 190–199 (2017). https://doi.org/10.2519/jospt.2017.689110.2519/jospt.2017.6891
Barra Ortiz, H.A., Matamala, A.M., Inostroza, F.L., Araya, C.L., Mondaca, V.N.: Efficacy of biofeedback in rehabilitation of musculoskeletal disorders: a systematic review. Postepy Rehabilitacji 36(1), 41 (2022)
Spencer, J., Wolf, S.L., Kesar, T.M.: Biofeedback for post-stroke gait retraining: a review of current evidence and future research directions in the context of emerging technologies. Front. Neurol. 12, 637199 (2021)
Barzegar Khanghah, A., Fernie, G., Roshan Fekr, A.: Design and validation of vision-based exercise biofeedback for tele-rehabilitation. Sensors 23(3), 1206 (2023)
Kim, W.-S., Cho, S., Ku, J., Kim, Y., Lee, K., Hwang, H.-J., Paik, N.-J.: Clinical application of virtual reality for upper limb motor rehabilitation in stroke: review of technologies and clinical evidence. J. Clin. Med. 9(10), 3369 (2020)
Park, J.-S., Jung, Y.-J., Lee, G.: Virtual reality-based cognitive–motor rehabilitation in older adults with mild cognitive impairment: a randomized controlled study on motivation and cognitive function. Healthcare 8, 335 (2020)
Chen, J., Or, C.K., Chen, T.: Effectiveness of using virtual reality–supported exercise therapy for upper extremity motor rehabilitation in patients with stroke: Systematic review and meta-analysis of randomized controlled trials. J. Med. Internet Res. 24(6), 24111 (2022)
Ai, Q., Liu, Z., Meng, W., Liu, Q., Xie, S.Q.: Machine learning in robot assisted upper limb rehabilitation: a focused review. IEEE Transactions on Cognitive and Developmental Systems (2021)
Khera, P., Kumar, N.: Role of machine learning in gait analysis: a review. J. Med. Eng. Technol. 44(8), 441–467 (2020)
Calvaresi, D., Marinoni, M., Dragoni, A.F., Hilfiker, R., Schumacher, M.: Realtime multi-agent systems for telerehabilitation scenarios. Artif. Intell. Med. 96, 217–231 (2019)
Blas, H.S.S., Mendes, A.S., Encinas, F.G., Silva, L.A., Gonz´alez, G.V.: A multiagent system for data fusion techniques applied to the internet of things enabling physical rehabilitation monitoring. Appl. Sci. 11(1), 331 (2020)
Roda, C., Rodríguez, A.C., López-Jaquero, V., Navarro, E., González, P.: A multi-agent system for acquired brain injury rehabilitation in ambient intelligence environments. Neurocomputing 231, 11–18 (2017)
Humayun, M., Jhanjhi, N.Z., Almotilag, A., Almufareh, M.F.: Agent-based medical health monitoring system. Sensors 22(8), 2820 (2022)
Sulis, E., Mariani, S., Montagna, S.: A survey on agents applications in healthcare: Opportunities, challenges and trends. Comput. Methods Programs Biomed. 107525 (2023)
Laranjo, L., Dunn, A.G., Tong, H.L., Kocaballi, A.B., Chen, J., Bashir, R., Surian, D., Gallego, B., Magrabi, F., Lau, A.Y., et al.: Conversational agents in healthcare: a systematic review. J. Am. Med. Inform. Assoc. 25(9), 1248–1258 (2018)
Vinoski, S.: Advanced message queuing protocol. IEEE Internet Comput. 10(6), 87–89 (2006). https://doi.org/10.1109/MIC.2006.116
Abdollahi, M., Kuber, P.M., Shiraishi, M., Soangra, R., Rashedi, E.: Kinematic analysis of 360 turning in stroke survivors using wearable motion sensors. Sensors 22(1), 385 (2022)
Weizman, Y., Tirosh, O., Fuss, F.K., Tan, A.M., Rutz, E.: Recent state of wearable imu sensors use in people living with spasticity: a systematic review. Sensors 22(5), 1791 (2022)
Bisio, I., Garibotto, C., Lavagetto, F., Sciarrone, A.: When ehealth meets iot: a smart wireless system for post-stroke home rehabilitation. IEEE Wirel. Commun. 26(6), 24–29 (2019)
Grip, H., Sundelin, G., Gerdle, B., Karlsson, J.S.: Variations in the axis of motion during head repositioning—a comparison of subjects with whiplash-associated disorders or non-specific neck pain and healthy controls. Clin. Biomech. 22(8), 865–873 (2007). https://doi.org/10.1016/j.clinbiomech.2007.05.008
Guidance, M.: Motion Guidance. https://www.motionguidance.com/. Accessed 31 Agu 2023
Yoon, T.-L., Kim, H.-N., Min, J.-H.: Validity and reliability of an inertial measurement unit–based 3-dimensional angular measurement of cervical range of motion. J. Manipulat. Physiol. Ther. 42(1), 75–81 (2019)
Riffitts, M., Oh, A., Alemu, A., Patel, V., Smith, C.N., Murati, S., Bailes, A., Allen, M., Dombrowski, M., Lee, J.Y., et al.: Functional range of motion of the cervical spine in cervical fusion patients during activities of daily living. J. Biomech. 152, 111528 (2023)
Acknowledgements
Héctor Sánchez San Blas research was supported by the Spanish Ministry of Universities (FPU Fellowship under Grant FPU20/03014). This work has been supported by the Junta De Castilla y Leon Consejería De Economía Y Empleo: Caracterización, análisis e intervención en la prevención de riesgos laborales en entornos de trabajo tradicionales mediante la aplicación de tecnologías disruptivas identified by 2022/00384/001-J125.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Contributions
André Sales Mendes: Conceptualization, Formal analysis, Methodology, Software, Visualization. Héctor Sánchez San Blas: Conceptualization, Investigation, Software, Validation, Visualization, Writing-originaldraft. Fátima Pérez Robledo: Investigation, Resources, Data-curation, Validation, Writing-original-draft. Juan F. de Paz Santana: Investigation, Methodology, Supervision, Resources. Gabriel Villarrubia González: Formal Analysis, Methodology, Data-curation, Supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Communicated by B. Bao.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sales Mendes, A.F., Sánchez San Blas, H., Pérez Robledo, F. et al. A novel multiagent system for cervical motor control evaluation and individualized therapy: integrating gamification and portable solutions. Multimedia Systems 30, 131 (2024). https://doi.org/10.1007/s00530-024-01328-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00530-024-01328-6