
Abstract
Purpose
We report on prevalence of anxiety, depression, and concentration difficulties and their associations in survivors of cancer in a nationally representative sample up to 25 years after diagnosis.
Methods
Using the National Health and Nutrition Examination Survey (NHANES) data from 2015 to 2018, participants between the ages of 18 and 79 self-reported on cancer history, symptoms of anxiety, depression, and difficulties with concentration.
Results
Of 10,337 participants, 691 (6.7%) reported a previous diagnosis of cancer; the median time since diagnosis was 8 years. Prevalence was similar between those with and without cancer for anxiety (45.8% versus 46.9%) and depression (19.7% versus 20.0%). Concentration difficulties were more common (11.3% versus 9.0%) for those with a history of cancer compared to those without (adjusted OR = 1.38, 95% CI: 1.00–1.90). Prevalence of mental health symptoms was not related to time since diagnosis. Anxiety and depression were highly correlated (r = 0.81, 95% CI: 0.74–0.86) and moderately correlated with difficulty with concentration (r = 0.52, 95%CI: 0.40–0.64 and r = 0.64, 95% CI: 0.53–0.74 respectively).
Conclusions
Difficulty with concentration was more commonly reported by participants with than without a cancer history. Report of anxiety and depression was no different between participants with and without a history of cancer. Anxiety, depression, and difficulties with concentration were strongly related. Further research is needed to explore if there is a causal association, and if so, the direction of these correlations, so that interventions may be appropriately targeted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Cancer survivors are at risk of physical and psychological morbidity in the years after treatment completion. Survivors experience anxiety, depression, and reduced cognitive function at rates greater than the general population. For example, 14–24% experience symptoms consistent with clinical levels of depression [1,2,3], and approximately 10% of survivors report clinical levels of anxiety [2]. In comparison, population estimates of depression and anxiety in the last year are 5% and 7% respectively [3,4,5]. Up to 75% of survivors also report difficulties with cognitive function, a rate higher than that detected by objective neuropsychological assessment [6,7,8]. Experiencing anxiety, depression, and decreased cognitive function impacts quality of life after cancer. Survivors reporting impaired memory and concentration experience difficulties returning to previous roles and work [8], greater reliance on psychotropic medication [9], and increased sleep disturbance [8]. Similar functional impacts are reported by survivors experiencing anxiety and/or depression [5, 10].
Some risk factors for increased anxiety, depression, and cognitive impairment appear to be shared. Survivors who are younger at diagnosis and female, and have lower education are more likely to report anxiety, depression, and impaired cognitive function [8, 9, 11, 12]. Older age at diagnosis is protective against anxiety and depression in the long term [12], but may be a risk factor for increased self-report of cognitive difficulties [13]. Those who are further from treatment appear to experience less depression [14], and self-reported cognitive difficulties [15], though anxiety may be more persistent over time [14]. However, there may be important differences in this trajectory according to cancer type, stage, and treatments received.
Self-reported cognitive symptoms, anxiety, and depression are strongly related [7, 16, 17]. The shared profile of risk factors has led some researchers and clinicians to consider the co-occurrence of mental health difficulties (i.e., anxiety, depression, and cognitive impairment) as a psychoneurological symptom cluster after cancer [16, 18]. To date, most research has focused on survivors of breast cancer. Research at the population level documenting the occurrence, and co-occurrence of mental health concerns across survivors of all cancers is scarce [15]. The aim of this study was to investigate whether cancer survivors have greater self-reported mental health symptoms (anxiety, depression, concentration difficulties) than individuals without a history of cancer using a population-based sample from the USA. A secondary aim was to investigate the effect of time since diagnosis for mental health symptoms among cancer survivors.
Methods
Study design and setting
National Health and Nutrition Examination Survey (NHANES) is a program of studies designed to assess the health and nutritional status of adults and children in the USA. The program has been administered every 2 years since 1999 and combines interviews and physical examinations. Data are collected on a voluntary basis and all results are either self-reported responses to interview questions or quantitative measurements administered by trained medical personnel. The survey examines a nationally representative sample of about 5000 persons through complex survey sampling. Oversampled subgroups include Hispanic persons, non-Hispanic Black persons, non-Hispanic Asian persons, and persons at or below the 185% of the US federal poverty line. Participants from the 2015–2016 and 2017–2018 datasets who were between the ages of 18 and 79 and recorded responses to mental health outcomes, age, gender, race/ethnicity, education, and cancer history were included in the analysis. All participants gave informed consent and ethical approval was granted by the National Center for Health Statistics Research Ethics Review Board Protocol #2011–17.
Measures
The primary outcomes for this analysis are three mental health outcomes: anxiety (How often do you feel worried or anxious?); depression (How often do you feel depressed?); and concentration difficulties (Do you have serious difficulty concentrating?). These items are taken from the Disability Questionnaire, as developed by the National Center for Health Statistics of the Centers for Disease Control and Prevention. Development involved input from federal agencies, and academic and private researchers. Questionnaires were tested in the NCHS Questionnaire Design Research Laboratory and in field tests. For more information, see https://www.cdc.gov/nchs/nhis/nhis_disability.htm. The anxiety and depression outcomes were dichotomized as either at least once a month or less than once a month and the concentration difficulties outcome remained as either yes or no. The exposure of interest was past history of cancer or malignancy (Have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?) and was dichotomized as either yes or no. Non-melanoma skin cancer was excluded from the history of cancer group.
Statistical methods
All analyses accounted for the complex survey design (clustering, stratification, weighting) using survey procedures available in SAS version 9.4 (SAS Institute, Cary, NC), using NHANES guidelines [19]. Descriptive statistics were stratified by cancer history. All percentages reported were survey-weighted. For the primary analysis, each mental health outcome was assessed through one unadjusted and two adjusted logistic regression models resulting in a total of nine models. Adjusted models included covariates selected a priori based on background knowledge and literature review. Covariates included age, gender (male/female), race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, and Other), and education (at least some college, no college). The first adjusted model estimated the effects of any type of cancer; the second modeled each tumor type. We categorized age into four separate strata: 18–35, 36–50, 51–65, 66–79 years.
Odds ratios (OR) and 95% confidence intervals (CI) were reported with the unexposed group being used as the reference group. Likelihood ratio tests were used to determine whether gender modified the relationship between cancer exposure and mental health outcomes. If the likelihood ratio test produced a statistically significant interaction, we stratified by gender and refit the models. Logistic regression was also used for our secondary analysis investigating the effect of self-reported time since cancer diagnosis among persons with a history of cancer. Polychoric correlation between each pair of mental health outcomes among persons with a history of cancer was also undertaken.
We performed a sensitivity analysis using propensity score stratification to account for large covariate imbalances (standardized mean differences > 0.25) in our study sample [20]. The propensity score model included gender, age, and race/ethnicity and accounted for the complex survey design using the methods outlined in Dugoff et al. [21]. Results from the sensitivity analysis were compared with the primary analysis to assess the robustness of the adjusted logistic regression models.
Results
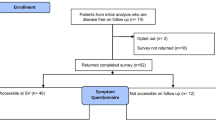
Of the 10,337 participants used for our analysis, 691 (6.7%) reported a previous history of cancer, excluding those with non-melanoma skin cancer (Table 1). As compared to participants with no history of cancer, participants with a history of cancer were more likely to be female (58% versus 51%), older (median = 63 versus 45 years), non-Hispanic White (76.5% versus 61.3%), and of slightly higher education (69% versus 64% with some college or more). Participants with a history of cancer were more heavily concentrated in the 51–65 (34.1%) and 66–79 (43.7%) age groups. The median time since diagnosis was 8 years (interquartile range, IQR = 4, 16) and median age at diagnosis was 51 years (IQR = 36, 61).
Tables 2 shows the results from the primary analysis as well as the proportion of participants with negative mental health outcomes within each exposure group. Anxiety was reported in 45.8% of participants with a history of cancer, and 46.9% of participants with no history of cancer. Prevalence of depression was similar between the groups (19.7% and 20%) and concentration difficulties were slightly higher in those with a history of cancer, 11.3% versus 9.0%. Prevalence of each of the outcomes prior to dichotomization is given in supplementary table S2. A high correlation between outcomes was found among cancer survivors. The overall correlation between anxiety and depression was 0.81 (95% CI: 0.74–0.86); between anxiety and concentration difficulties 0.52 (95% CI: 0.40–0.64); and between depression and concentration difficulties 0.64 (95% CI: 0.53–0.74). Figure 1 shows the correlation between anxiety, depression, and reported concentration difficulties across each 5-year interval since diagnosis.

Proportion of participants with a history of cancer (N = 691) reporting anxiety, depression, and difficulty concentrating across time since diagnosis. Error bars are 95% CI. rAD shows the correlation between anxiety and depression across time since diagnosis, rDC shows the correlation between depression and difficulty concentrating, and rAC shows the correlation between anxiety and difficulty concentrating. Missing correlations in rAC are due to zero cells in the 2 × 2 table
Statistically significant results were not found in any unadjusted models, although 95% CIs included potentially important values for each outcome. As compared to participants without a history of cancer, participants with a history of cancer had a higher adjusted odds of concentration difficulties (adjusted odds ratio (AOR) = 1.38, 95% CI: 1.00, 1.90). Adjusted odds were slightly elevated, but not statistically significant for depression (AOR 1.10 (95% CI: 0.86, 1.41)) and anxiety (AOR 1.12 (95% CI: 0.87, 1.43)) for persons with a history of cancer compared to those without. When comparing specific tumor types with no history of cancer, there was no evidence of an effect, except for upper gastrointestinal tumors for anxiety (AOR = 2.18, 95% CI 1.13, 4.21) and depression (AOR = 3.66, 95% CI 1.28, 10.5); and colorectal cancer and breast cancer for concentration difficulties (colorectal cancer AOR = 2.40, 95%CI 1.07, 5.37; and breast cancer AOR = 2.07, 95%CI 1.02, 4.20). No specific tumor types showed significant results for more than one mental health outcome. Given the small numbers in many of the cells by tumor type, care should be taken when interpreting the results. Gender modified the effect of cancer history on concentration difficulties (pinteraction, adjusted = 0.04), with larger effects seen for women (AOR = 1.66, 95% CI: 1.16, 2.37) than men (AOR = 0.9495% CI: 0.56, 1.58). There was no evidence of effect modification by gender for anxiety (pinteraction, adjusted = 0.23) or depression (pinteraction, adjusted = 0.64).
Table 3 shows the results from the secondary analysis which investigated the time since diagnosis among cancer survivors. Figure 1 shows similar proportions of survivors report anxiety, depression, and difficulty with concentration across each 5-year interval since diagnosis. No statistically significant results were discovered in unadjusted or adjusted models for anxiety (AOR for each 10 years since diagnosis = 0.98, 95% CI: 0.74, 1.30), depression (AOR = 0.90, 95% CI: 0.61, 1.35), or concentration difficulties (AOR = 0.77, 95% CI: 0.49, 1.20). Comparisons by tumor type in adjusted models did not yield any statistically significant results.
Results from the sensitivity analysis mirrored those of the primary analysis. Supplementary Table 1 presents the results from the adjusted models in our sensitivity analysis and compares the results to the adjusted models of our primary analysis.
Discussion
This paper reports on data from 10,337 participants in NHANES, 2015–2018, comparing those with a history of cancer to those without cancer on self-reported mental health outcomes. We found comparable rates of self-reported anxiety (around 46%) and depression (around 20%) between participants with and without a history of cancer. Overall, 11% of cancer survivors reported difficulties with their concentration compared to 9% of participants without a history of cancer. Cancer survivors had a 38% increased odds of self-reporting problems with their concentration compared with participants without a history of cancer. Colorectal and breast cancer survivors had a twofold increased odds of reporting difficulties concentrating compared to participants without a history of cancer. Women with a history of cancer were at higher odds of reporting cognitive symptoms compared to men with a history of cancer. Time since diagnosis did not impact the odds of reporting mental health concerns. There were strong correlations between mental health outcomes, particularly between anxiety and depression.
Anxiety and depression were commonly reported in our sample, regardless of cancer history, in contrast to previous studies identifying a difference in prevalence of symptoms between cancer survivors and controls or normative data [1,2,3, 12, 14]. We found approximately 20% and 46% of participants reported some degree of depression or anxiety at least once a month. This may be due to the sample and differences in measures employed. NHANES is a nationally representative sample for the USA, and most previous studies have not been population-based. Further systematic reviews including studies with validated and clinical measures indicate approximately 20% and 10% of cancer survivors have symptoms consistent with a diagnosis of depression or anxiety respectively [2, 14]. Participants with a history of upper gastrointestinal cancer were more likely to report experiencing depression or anxiety, and the odds of reporting anxiety and depression were 2.18 and 3.66 greater for those with upper gastrointestinal cancer compared to those with no cancer history. Upper gastrointestinal cancer survivors can experience physical symptoms, changes in eating behaviors, and physical functioning leading to appreciable impacts on quality of life [22, 23], which in turn may increase risk of depression and anxiety [23, 24]. However, due to small sample sizes in this diagnosis group, this result should be interpreted with caution and warrants further research.
Participants with a history of cancer were more likely to report difficulties with concentrating than participants without a history of cancer, and those with colorectal or breast cancer diagnosis were at particular risk, as were women. These results are largely consistent with previous studies employing large nationally representative samples [15, 25], and a recent review of longitudinal studies of self-reported cognitive impairment after chemotherapy which indicated between 11 and 37% of survivors experienced significant cognitive decline after initiating chemotherapy [17].
For all mental health outcomes, we did not find an effect of time since diagnosis, with a relatively consistent proportion of participants reporting difficulties with anxiety, depression, and concentration after treatment. Mental health concerns may remain relatively stable in the early years after diagnosis. For example, in the first 12 months after diagnosis, prevalence of anxiety and depression in a population-based sample was relatively stable at around 20% and 13% respectively [26]. Longitudinal studies with a longer follow-up suggest some improvement in symptoms of depression [14, 27, 28], and self-reported cognitive difficulties [17], as time post treatment increases. However, there appears to be a proportion of survivors that continue to experience significant mental health symptoms that impact on their quality of life [29], and ability to return to usual roles (e.g., work) [30].
Consistent with previous research, we found strong correlations between mental health outcomes. Anxiety and depression were highly correlated while difficulty with concentration was moderately correlated with both anxiety and depression. These results add to the growing body of literature demonstrating interrelatedness of anxiety, depression, and cognitive symptoms [9, 12, 16, 31]. However, our study and most previous studies have been cross-sectional, making causal inferences impossible about whether one symptom precedes another or whether they are co-occurring. Furthermore, it is possible that fatigue, sleep quality, and other psychological factors such as stress and loneliness contribute to reporting mental health symptoms [8, 32,33,34]. Given many of these symptoms are amenable to intervention [35], further research is needed to understand the interrelatedness, any potential confounds, and causal directions of psychological symptoms experienced during survivorship to offer tailored support with the potential to improve quality of life overall.
There are several limitations worth noting. This study relied on single-item measures of anxiety, depression, and cognitive symptoms. While a single question covering mental health symptoms is brief and potentially mimics clinical encounters, they may miss important impacts. For example, only difficulties regarding concentration were assessed, yet previous research has consistently demonstrated survivors often report difficulties with memory and other cognitive abilities [36]. Further research investigating the utility of single-item questions for screening for mental health concerns is warranted [37]. Our sample had a median age at diagnosis of 51 years, over-representation of non-Hispanic White, and well-educated participants, as well as small sample sizes in some diagnostic groups. As such, our results may not generalize to all cancer survivors and should be interpreted cautiously for survivors of respiratory, upper gastrointestinal, and hematological cancers. Furthermore, we had no data regarding stage of disease and treatment which may also impact symptom severity.
We report on data from a large national sample of participants using single-item measures of three commonly experienced mental health concerns. We found no evidence of difference in the prevalence of anxiety and depression between participants with and without a history of cancer, but those with a history of cancer were more likely to report difficulties with concentration. Incidence of these symptoms was stable in the years after cancer diagnosis. Anxiety, depression, and difficulties with concentration were strongly related; however, further research is needed to explore the causal direction of these correlations, so that interventions may be appropriately targeted.
Data availability
All data are available for download from the NHANES website. Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, https://wwwn.cdc.gov/nchs/nhanes/Default.aspx.
References
Niedzwiedz CL, Knifton L, Robb KA, Katikireddi SV, Smith DJ (2019) Depression and anxiety among people living with and beyond cancer: a growing clinical and research priority. BMC Cancer 19(1):943
Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, Johansen C et al (2011) Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol 12(2):160–174
Hartung TJ, Brähler E, Faller H, Härter M, Hinz A, Johansen C et al (2017) The risk of being depressed is significantly higher in cancer patients than in the general population: prevalence and severity of depressive symptoms across major cancer types. Eur J Cancer 72:46–53
Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V et al (2014) The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. Int J Epidemiol 43(2):476–493
Pitman A, Suleman S, Hyde N, Hodgkiss A (2018) Depression and anxiety in patients with cancer. BMJ 361:k1415
Henneghan AM, Van Dyk K, Kaufmann T, Harrison R, Gibbons C, Heijnen C, et al. (2021) Measuring self-reported cancer-related cognitive impairment: recommendations from the Cancer Neuroscience Initiative Working Group. J Natl Cancer Inst 113(12):1625–1633. https://doi.org/10.1093/jnci/djab027
Bray VJ, Dhillon HM, Vardy JL (2018) Systematic review of self-reported cognitive function in cancer patients following chemotherapy treatment. J Cancer Surviv 12(4):537–559
Lange M, Licaj I, Clarisse B, Humbert X, Grellard JM, Tron L et al (2019) Cognitive complaints in cancer survivors and expectations for support: results from a Web-based survey. Cancer Med 8(5):2654–2663
Boscher C, Joly F, Clarisse B, Humbert X, Grellard J-M, Binarelli G et al (2020) Perceived cognitive impairment in breast cancer survivors and its relationships with psychological factors. Cancers 12(10):3000
Carreira H, Williams R, Müller M, Harewood R, Stanway S, Bhaskaran K (2018) Associations between breast cancer survivorship and adverse mental health outcomes: a systematic review. J Natl Cancer Inst 110(12):1311–1327
Walker J, Hansen CH, Martin P, Symeonides S, Ramessur R, Murray G et al (2014) Prevalence, associations, and adequacy of treatment of major depression in patients with cancer: a cross-sectional analysis of routinely collected clinical data. Lancet Psych 1(5):343–350
Götze H, Friedrich M, Taubenheim S, Dietz A, Lordick F, Mehnert A (2020) Depression and anxiety in long-term survivors 5 and 10 years after cancer diagnosis. Support Care Cancer 28(1):211–220
Mandelblatt J, Small B, Luta G, Hurria A, Jim H, McDonald B et al (2018) Cancer-related cognitive outcomes among older breast cancer survivors in the thinking and living with cancer study. J Clin Oncol 36(32):3211–3222
Mitchell AJ, Ferguson DW, Gill J, Paul J, Symonds P (2013) Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncol 14(8):721–732
Williams A, Janelsins MC, van Wijngaarden E (2016) Cognitive function in cancer survivors: analysis of the 1999–2002 National Health and Nutrition Examination Survey. Support Care Cancer 24(5):2155–2162
Chapman B, Helmrath S, Derakshan N (2019) Perceived cognitive functioning and its influence on emotional vulnerability in breast cancer. Health Psychol Open 6(2):2055102919871661
Kim HJ, Jung SO, Kim H, Abraham I (2020) Systematic review of longitudinal studies on chemotherapy-associated subjective cognitive impairment in cancer patients. Psychooncology 29(4):617–631
George MA, Lustberg MB, Orchard TS (2020) Psychoneurological symptom cluster in breast cancer: the role of inflammation and diet. Breast Cancer Res Treatm 184(1):1–9
Akinbami LJ, Chen TC, Davy O, Ogden CL, Fink S, Clark J, et al (2022) National Health and Nutrition Examination Survey, 2017–March 2020 prepandemic file: Sample design, estimation, and analytic guidelines. National Center for Health Statistics. Vital Health Stat 2(190). https://doi.org/10.15620/cdc:115434
Austin PC (2011) An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar Behav Res 46(3):399–424
Dugoff EH, Schuler M, Stuart EA (2014) Generalizing observational study results: applying propensity score methods to complex surveys. Health Serv Res 49(1):284–303
Ahn S, Jung H, Kim S, Shin SJ, Park CG, Chu SH (2017) Quality of life among Korean gastrointestinal cancer survivors. Eur J Oncol Nurs 30:15–21
Soares JDP, Gomes TLN, Siqueira JM, Oliveira ICL, Mota JF, Laviano A et al (2019) Muscle function loss is associated with anxiety in patients with gastrointestinal cancer. Clin Nutr ESPEN 29:149–153
Hu L-Y, Liu C-J, Yeh C-M, Lu T, Hu Y-W, Chen T-J et al (2018) Depressive disorders among patients with gastric cancer in Taiwan: a nationwide population-based study. BMC psych 18(1):1–8
Jean-Pierre P, Winters PC, Ahles TA, Antoni M, Armstrong FD, Penedo F et al (2011) Prevalence of self-reported memory problems in adult cancer survivors: a national cross-sectional study. J Oncol Pract 8(1):30–34
Boyes AW, Girgis A, D’Este CA, Zucca AC, Lecathelinais C, Carey ML (2013) Prevalence and predictors of the short-term trajectory of anxiety and depression in the first year after a cancer diagnosis: a population-based longitudinal study. J Clin Oncol 31(21):2724–2729
Mols F, Schoormans D, de Hingh I, Oerlemans S, Husson O (2018) Symptoms of anxiety and depression among colorectal cancer survivors from the population-based, longitudinal PROFILES registry: prevalence, predictors, and impact on quality of life. Cancer 124(12):2621–2628
Maass SW, Roorda C, Berendsen AJ, Verhaak PF, de Bock GH (2015) The prevalence of long-term symptoms of depression and anxiety after breast cancer treatment: a systematic review. Maturitas 82(1):100–108
Muzzatti B, Cattaruzza N, Piccinin M, Flaiban C, Agostinelli G, Berretta M et al (2021) Cognitive function in long-term lymphoma survivors: relationship between subjective reports and objective assessments and with quality of life. Psychol Health Med 26(8):968–979
Chapman B, Derakshan N, Grunfeld EA (2022) Exploring primary breast cancer survivors' self-management of sustained cancer-related cognitive impairment in the workplace. Psycho-Oncology 31(4):606–613.https://doi.org/10.1002/pon.5844
Gutenkunst SL, Vardy JL, Dhillon HM, Bell ML (2021) Correlates of cognitive impairment in adult cancer survivors who have received chemotherapy and report cognitive problems. Support Care Cancer 29(3):1377–1386
Henneghan A, Stuifbergen A, Becker H, Kesler S, King E (2018) Modifiable correlates of perceived cognitive function in breast cancer survivors up to 10 years after chemotherapy completion. J Cancer Surviv 12(2):224–233
Hsu YH, Chen VCH, Hsieh CC, Weng YP, Hsu YT, Hsiao HP et al (2021) Subjective and objective cognitive functioning among patients with breast cancer: effects of chemotherapy and mood symptoms. Breast Cancer 28(1):236–245
Levkovich I, Cohen M, Alon S, Kuchuk I, Nissenbaum B, Evron E et al (2018) Symptom cluster of emotional distress, fatigue and cognitive difficulties among young and older breast cancer survivors: The mediating role of subjective stress. J Geriatr Oncol 9(5):469–475
Fardell J, Vardy J, Johnston I, Winocur G (2011) Chemotherapy and cognitive impairment: treatment options. Clin Pharmacol Therapeutics 90(3):366–376
Li M, Caeyenberghs K (2018) Longitudinal assessment of chemotherapy-induced changes in brain and cognitive functioning: A systematic review. Neurosci Biobehav Rev 92:304–317
Fardell JE, Bray V, Bell ML, Rabe B, Dhillon H, Vardy JL (2022) Screening for cognitive symptoms among cancer patients during chemotherapy: sensitivity and specificity of a single item self report cognitive change score. Psycho Oncology 31(8):1294–1301. https://doi.org/10.1002/pon.5928.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions Dr Melanie Bell was supported by the National Cancer Institute of the National Institutes of Health under award number P30 CA023074.
Dr Janette Vardy is supported by a National Health Medical Research Council Investigator Grant (grant number APP1176221).
Author information
Authors and Affiliations
Contributions
All the authors contributed to the conceptualization, methodology, writing-draft and writing-review, and editing. Melanie Bell and Chase Irwin conducted all data curation, formal analysis, and visualization. Melanie Bell conducted project administration and validation. The first draft of the manuscript was written by Joanna Fardell and all the authors commented on previous versions of the manuscript. All the authors read and approved the final manuscript. Melanie Bell and Janette Vardy provided supervision.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants gave informed consent and ethical approval was granted by the National Center for Health Statistics Research Ethics Review Board Protocol #2011–17.
Consent for publication
Not applicable, no individual data or images are presented in this manuscript.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fardell, J.E., Irwin, C.M., Vardy, J.L. et al. Anxiety, depression, and concentration in cancer survivors: National Health and Nutrition Examination Survey results. Support Care Cancer 31, 272 (2023). https://doi.org/10.1007/s00520-023-07710-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00520-023-07710-w