
Abstract
Introduction
Twenty percent of breast cancer survivors have co-occurring diabetes and face a 50% greater risk of 10-year mortality compared to survivors without diabetes. Individuals with cancer are often overwhelmed during cancer treatment and have less time for their diabetes, contributing to worse outcomes. We elicited perspectives of breast cancer survivors with diabetes regarding their specific needs for diabetes and cancer co-management.
Methods
We conducted semi-structured interviews with women with breast cancer aged 40 + years at three New York City hospitals from May 2021 to March 2022. Eligible participants had type 2 diabetes or pre-diabetes. Interviews were audio-recorded, professionally transcribed, and coded by two independent reviewers.
Results
We conducted interviews with 15 females with breast cancer of mean age 61.5 years (SD 7.2); 70% were Black, Hispanic, or Asian/Pacific Islander, and 20% had only a high school education. Most (73%) patients were insured by Medicaid or Medicare, and 73% underwent chemotherapy as part of their cancer care. Of the 15 participants, 60% reported that their glucose levels were of control during cancer treatment and nearly 50% reported glucose levels > 200 mg/dL. We identified distinct themes that reflect patient-reported challenges (worse glucose control after initiation of cancer treatment, lack of information on co-managing diabetes, negative psychosocial effects, burden of diabetes management during cancer care) and needs/priorities (designated provider to help, educational resources specific to diabetes and cancer, and individualized care plans).
Conclusions
Patients co-managing diabetes and cancer face challenges and have unmet needs that should be addressed to improve diabetes control during cancer treatment. Our findings can directly inform interventions aimed at improving glucose control in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the USA, 20% of the 3.5 million breast cancer survivors had diabetes at the time of their cancer diagnosis [1,2,3]. Patients with breast cancer and diabetes have a 50% increased risk of 10-year all-cause and breast cancer-related mortality compared to breast cancer patients without diabetes [4, 5]. The poor outcomes observed among patients with cancer and diabetes are hypothesized to be partially due to diabetes management receiving less attention than usual (e.g., fewer primary care provider [PCP] or endocrinology visits and less diabetes self-care) during active cancer care [6]. Self-care for diabetes is already challenging without cancer [7], and adding a cancer diagnosis often overwhelms patients and makes diabetes self-care even more difficult [8, 9].
Prior work has shown that patients with cancer have difficulty finding time for diabetes management during cancer treatment, which they say demands their full attention [8, 10]. We have also heard from oncologists that diabetes management is not their clinical priority or expertise [9, 11, 12]. Furthermore, as patients need to see oncologists frequently during active cancer care, they have less time and energy to see their PCPs, limiting the PCP’s ability to manage diabetes during this acute phase of cancer care [13]. Finally, PCPs have limited knowledge of rapidly changing chemotherapeutic agents [14] and may not feel confident about how to manage diabetes during chemotherapy [12].
The current study sought to elicit the perspectives of patients with breast cancer and diabetes regarding the specific challenges they faced and unmet needs in terms of diabetes and cancer co-management. By better understanding what exactly patients need to successfully co-manage these two burdensome conditions, interventions can be designed to directly respond to patient challenges, needs, and priorities. Because minorities with both breast cancer and diabetes are at especially high risk of poor outcomes [15], we aimed to recruit mostly minority women.
Methods
Study design
This qualitative study conducted semi-structured interviews with patients to elucidate patient-perceived needs and priorities for diabetes management during breast cancer treatment. This study was approved by the WCM Institutional Review Board (20–03,021,654).
Setting
To identify and recruit eligible participants, we collaborated with oncology providers from NewYork-Presbyterian (NYP)-Weill Cornell Medicine (WCM), NYP-Brooklyn Methodist Hospital, and NYP-Queens Hospital. All three hospitals are part of the NYP Healthcare System, which serves patients from all five boroughs of New York City. NYP-WCM is a large teaching hospital in the Upper East Side. Annually, there are more than three million patient visits, and the faculty provide care for over 200 inpatients on any given day at both the Upper East Side and Lower Manhattan NYP/WCM campuses. Located in Park Slope, NYP-Brooklyn is a large academic hospital that provides approximately 40,000 inpatient visits and 500,000 outpatient visits annually. NYP-Queens is a community teaching hospital in Flushing that provides approximately 162,000 ambulatory care visits and 124,000 emergency service visits annually. Additionally, to achieve greater patient diversity, we partnered with New York-based breast cancer patient advocacy organizations to disseminate an electronic flyer with a summary of the study. Interested and eligible patients contacted the research team via telephone or email; afterwards, a research assistant (JC) followed up with patients to confirm eligibility, further explain the study details, and answer potential questions.
Participant eligibility and recruitment
We employed purposive sampling to achieve a diverse sample of eligible participants. To be eligible, participants had to be 40 years of age or older, diagnosed with breast cancer, and have type 2 diabetes or pre-diabetes. In collaboration with providers from NYP-WCM, Brooklyn, and Queens, we received referrals of eligible patients. First, providers received permission from the patients to share their contact information with the research team. Afterwards, a research assistant (JC) used a standardized script to approach eligible patients via telephone to invite them to participate in the study. During this initial call, the research assistant explained the details of this study and answered potential questions. Due to the COVID-19 pandemic, we conducted all semi-structured interviews virtually using Zoom Video Conferencing software, a secure HIPAA-compliant platform. Participants provided verbal and electronic consent, which included permission to record the interviews and publish de-identified excerpts.
Data collection and interviews
Two researchers trained in qualitative methods conducted one-on-one semi-structured virtual interviews in English. Interviews were conducted virtually on Zoom. Interviews lasted 45–60 min.
A semi-structured topic guide was used to guide each patient interview. The topic guide was developed using insights from our group’s prior work [10, 16], as well as discussions with clinical experts in endocrinology, primary care, and oncology. First, patients were asked to describe their overall experiences co-managing diabetes and breast cancer. The interviewer probed patients about challenges, surprises, and what they wish they had known at the time. Patients were asked to share what went well in their experiences, what kind of unmet needs they had, and what they wish providers or clinical staff had done more or less of. Patients elaborated on specific examples and situations they encountered during their experience caring for diabetes and cancer. Lastly, patients were asked to provide their perspectives on a theoretical co-management program in which a nurse practitioner embedded in the oncology care team managed their diabetes during chemotherapy. The goal of this question was to obtain patient impressions and perspectives about an intervention that our team is currently developing.
Demographic survey
At the end of each interview, participants completed a demographic questionnaire that asked them to report: age, gender, race/ethnicity, highest level of education completed, insurance type, months/years since breast cancer diagnosis, months/years since diabetes diagnosis, cancer treatments received, type of diabetes management (e.g., diet/exercise, pills, insulin), if their glucose became out of control during cancer treatments, and the highest glucose they recall during cancer treatment. The two last questions focused on the short-term diabetes management experience. Participants then received a $50 gift cards.
Data analysis
All 15 interviews were audio-recorded and professionally transcribed by Ubiqus, a transcription service. Prior to data analysis, interview transcripts were de-identified to ensure confidentiality.
We used a thematic approach to analyze the patient interview data, which has been widely used in health services research [17]. First, an open coding system was used, wherein two team members (JC & MW) independently reviewed and coded four initial transcripts. Afterwards, discrepancies were reconciled by a senior team member (LCP) and codes were consolidated into a codebook. Then, two team members (JC & JR) independently coded the remaining 11 transcripts. All transcript data were then analyzed using a custom-built Python-visualization tool [18]. Finally, the team (JC, JR, LCP) reviewed the analyses as a group and came up with over-arching themes.
The qualitative study adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Supplemental Material 1).
Results
Participant characteristics
Between May 2021 and March 2022, we conducted 15 semi-structured, virtual interviews with patients who had breast cancer and type 2 diabetes. Of these interview participants, the mean age was 61.5 years (SD 7.2); 100% were female; 70% were either Black, Hispanic, or Asian/Pacific Islander; and 20% had only a high school education (Table 1). The mean number of years since their diabetes was first diagnosed was 15 (SD 6.8) years, and the median was 12 years. The mean time since their breast cancer was first diagnosed was 3.3 (SD 3.6) years. Most (73%) patients were insured by Medicaid or Medicare and 73% underwent chemotherapy as part of their cancer care. Almost all (87%) used diet, exercise, or oral diabetes medications to manage their glucose during cancer treatments. Of the participants, 60% reported having their glucose out of control during cancer treatments, and nearly 50% reported glucose levels > 200 mg/dL during that time.
Qualitative themes
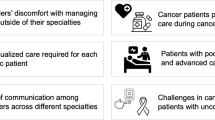
The analyses indicated that we reached thematic saturation after 13 interviews; two additional interviews were conducted to confirm saturation. Our team identified six distinct themes that reflect patient-reported challenges, needs, and priorities for diabetes and cancer co-management (Fig. 1).

Major themes and subthemes identified from patient interviews
-
Theme 1: Patients report that their diabetes was out of control after initiation of breast cancer treatment
Most patients reported a noticeable decline in their glucose control and self-management activities following initiation of breast cancer treatments. Patients struggled to get their diabetes under control in the short-term.
From the first time I started [cancer treatments], which this is now in round three, that’s when the numbers were going up. And now, I have to be perfectly honest with you. It’s kind of upsetting to me because I have worked so hard prior to that.
I had disclosed to them that I had the cancer diagnosis and how now my sugars are not being managed as a result of me getting the chemo…now that I’m starting to take the chemo and use steroids, the numbers [glucose levels] are very high.
I didn’t really know if I had full-blown diabetes or was I pre-diabetic, and if you’re pre-diabetic does that mean you have diabetes? I was really just focused on the cancer part of it also, so it [glucose] wasn’t being controlled really at all.
Patients also reported having side effects from chemotherapy which affected their diabetes management. For many patients, nausea and vomiting influenced how much and what they could eat. Patients attributed worse glucose control to these appetite changes.
Well, I think it usually gets low during my treatments because I didn’t--I wasn’t eating…With the treatments for the cancer and the diabetes I’m not eating. It usually gets low and makes me sick.
On the diabetes too, because there are certain things you can’t eat, and then with the cancer, both of them combined together, that’s certain things you can’t eat and you don’t have an appetite, and if you don’t eat you feel sick. Diabetes makes you nauseous, wobbly, and sometimes you break into sweats. At least I break into sweats. I get sweats. And then with cancer after the surgery they started chemo. You have no appetite. It was hard.
For other patients, the added burden of managing both diabetes and breast cancer therapy made it difficult for them to take care of their overall health.
It was real hard because when they told me I was diagnosed with cancer I like fell off - -. I took my medicine and stuff—talk about I wasn’t eating right and my sugar was all over the place.
-
Theme 2: Patients report lack of information on managing both their diabetes and breast cancer
Patients did not receive diabetes-cancer specific educational information or guidance to prepare them to manage the two conditions simultaneously.
Yeah, they talked a little bit but not much because they know that I’m probably just started out with cancer so they know my mind probably just on cancer.
My doctor was always just focused on the cancer, that was it.
I really didn’t think that my diabetes was an issue. It wasn’t until I was taking part of the chemotherapy toward the end that my sugar escalated to 479 one day. I found myself in the hospital and at that point my medication was increased, I found myself with the neuropathy in my feet and hands, and that feels like it’ll never go away, but that was really when I realized that the diabetes was even a factor.
Some patients were unaware that increased blood glucose levels were a potential side effect of receiving treatment for cancer.
I wish my doctors would have told me to expect possible changes in my blood sugar levels and maybe given me some help as to how to control it.
When I first started cancer treatment, I didn’t think I had diabetes…I don’t know if they were testing it, but I can say they never mentioned anything to me until like about a year now or so.
Specifically, patients wanted information about how to manage their diet so they can manage their diabetes on their own. Some expressed a desire for this advice to be tailored to their situation, and to be more involved in the discussions with their providers.
I think there has to be an educational component regarding nutrition and allowances when you have glucose, so it helps me be lowering it.
I have brain fog from chemo, chemo brain. Smoothie recipes…I can look it up. I’ve got books. I don’t need that. I’m not getting what I’m needing from nutritional counseling. Nobody’s talking about the anemia, the glucose, this is what’s going on. That’s what I expect from them.
-
Theme 3: Patients report actively taking ownership of their diabetes during breast cancer treatment
Patients reported feeling frustrated that no one was actively caring for their diabetes during cancer treatment or giving them guidance to do so, which led patients to feel that they had to take ownership themselves. This often resulted in seeking care from multiple different providers and searching for answers to their questions online.
I started getting baselines from cardiology, the memory specialist, gynecology. I started my own. My doctor never told me to do any of these things. But I did it myself to develop baselines
Even before I was diagnosed with the breast cancer, the primary care doctor had referred me to an endocrinologist. So I had started care for diabetes maintenance and management even before the breast cancer. When I heard about the breast cancer, the concern was even more of a concern. Because I do follow up on medical issues. It’s part of how I feel I must manage myself regardless of any diagnoses. It was a concern for me. It still is. But I’ve always taken strict measures as best as possible to manage the diabetes.
Every day I read on breast cancer. Every day I read on google about diets and exercise.
And I’ve even gone to the point where I look back at the same date last year or whatever to check to see what was the numbers then and what’s happened between last year and this year. I really advocate for myself and my own health.
-
Theme 4: Patients report experiencing negative psychosocial effects of managing both their diabetes and breast cancer
Patients reported feeling overwhelmed, anxious, and depressed as they experienced challenges in managing both diabetes and breast cancer. These patients felt their diabetes self-management was an added stress, which affected their mental well-being.
Very down, depressed, it’s something more to add on to cancer and it’s very stressful—testing strips, prick your finger when you’re disabled yourself on one side, more medication to add on to and I take chemo pills every day, it is very hard.
I’m afraid to because it could really screw up everything in my body. So I’m really afraid. That’s really the truth.
“I think that was traumatic for me, like pricking my finger was just, I don’t know, it somehow felt like self-mutilation. It was very hard for me to do it.
-
Theme 5: Patients report wanting a designated provider to co-manage their diabetes during cancer treatments
Patients were unsure of which provider they should go to for diabetes-related needs during cancer care and expressed a desire for a specific provider to be designated. Patients liked the possibility of a designated nurse practitioner to help manage their diabetes but wanted them to communicate with their oncologist.
Having a nurse practitioner as an advocate and an additional care provider, it makes things happen more regularly instead of my worrying, “Oh my gosh; my blood sugar was high this morning and my next visit is next week. Should I call the doctor? Should I go to the hospital?” But just knowing that there’s another caregiver who can help to just monitor things that cause stress and anxiety, I think that’s a great, wonderful initiative.
Interviewer: “How important is it for you for this nurse practitioner, this health coach for diabetes and breast cancer, how important is it for this person to talk to your oncologist directly?” Patient: “100% important”
Yeah and a conversation with the oncologist. Because again, the protocol is what’s keeping me alive.
-
Theme 6: Patients report the need for individualized glucose management during active breast cancer treatment
Patients report having complex, varying needs in relation to their glucose management during cancer care and want their providers to devise an individualized plan for them.
I’m not getting anything really in regard to glucose or anything else that’s a residual or symptom or could be a long-haul experience. That makes me worried.
Some counseling kind of talk, so to speak, might be helpful to a person who may potentially end up dealing with diabetes during the cancer treatment, what could happen.
Patients would like the option of either in-person or virtual individualized glycemic control.
Interviewer: “Would you prefer to see this person [individual responsible for glucose management] in person or telehealth?
Patient: “If they’re in the same building or the same place I’m getting the treatment, then I don’t mind in person. If it’s a matter of “I can’t see you on that day, but we can have a tele-visit the next day or another day during the week,” then I’m fine with that. But I actually like seeing people in person.”
Furthermore, patients would like more advice related to diet and nutrition which they believe is key to keeping their glucose levels under control.
I think they [oncologists] should be looking at what foods contradict chemotherapy, like I mentioned, because patients don’t know and they could be taking something that nobody knows about, whether it’s for a glucose study or not.
Just to make sure the person [individual responsible for glucose management] can explain about…how they numbers are and what they do—numbers to normal every day and eat the right proper diet, make sure I’m eating the right proper food to keep on with my diet.
Discussion
We report the perspectives of 15 patients with breast cancer and diabetes regarding their specific needs and priorities for effective management of both diabetes and cancer during active cancer treatment. We found that patients experienced worsening glucose control following initiation of cancer treatments, and the combination of the worsening glycemic control and burden of cancer treatments led to negative psychosocial consequences including anxiety and depression. To address these problems, patients reported wanting to be equipped with an individualized diabetes-cancer management plan and diabetes-cancer specific educational materials and guidance. Furthermore, they noticed that there was no single provider in charge of glucose management during the acute cancer care phase and expressed a desire to have a specific provider designated to them.
Our findings on the challenges that patients face managing both their diabetes and cancer during active cancer therapy are consistent with prior studies, which have reported that chemotherapy regimens that include corticosteroids [19] can elevate glucose levels in people with recognized diabetes and can cause steroid-induced diabetes in patients without previously recognized diabetes [20, 21]. In fact, steroids can worsen undiagnosed or pre-diabetes to clinically severe diabetes [22]. Hyperglycemia during chemotherapy has also been shown to increase the risk of chemotherapy-related toxicity and require chemotherapy-dose reductions [23, 24]. Uncertainty about which provider should be responsible for glucose management during cancer treatments has also been previously documented [12] and appears to be a prevalent barrier to effectively co-managing diabetes and cancer. Additionally, uncertainty about which provider to refer to combined with the lack of educational materials led patients to feel that they had to become extremely pro-active about finding help, information, and answers to their questions. Unfortunately, this contributed to patients feeling confused and overwhelmed. To the best of our knowledge, ours is the first study to describe the psychosocial effects of co-managing diabetes and cancer. There has been work done documenting the psychosocial effects of managing each condition, separately [25,26,27,28,29].This is especially true for cancer, where studies have reported that depression is three times more prevalent among patients with cancer than the general population [29].
Patients articulated several needs for managing their diabetes during cancer treatment that were important to them: (1) an individualized diabetes/cancer care plan, (2) a designated provider for diabetes management during cancer, and (3) cancer- and diabetes-specific education. Designating a specific provider to be responsible for managing diabetes during active cancer treatments may help overcome some of the patient-reported challenges in self-managing diabetes during active cancer treatment. In particular, nurse practitioners (NPs) have been shown to successfully manage diabetes in outpatient [30, 31], inpatient [32], and community [33] settings, and NPs have also been successfully integrated into oncology care teams to support general cancer care [34]. However, including an NP on an oncology care team to specifically manage diabetes for cancer patients receiving chemotherapy has not yet been reported. Our prior work has confirmed that this is an appealing solution for both PCPs and oncologists [35], and our current study clarified what should be included in this intervention from the patient perspective. To ensure that this proposed strategy of leveraging NPs is consistent with patient values and priorities, the intervention should provide an individualized management plan for each patient including diabetes medication management, especially when nausea limits dietary intake; nutrition counseling; frequent check-ins; and diabetes- and cancer-specific educational materials. Our study team will use this patient-generated information to refine an NP-led intervention, which is part of a larger study to improve diabetes care during cancer treatments. By engaging patient stakeholders in the intervention development process, we seek to make our solution to sub-optimal diabetes management during cancer care, patient-centered.
Limitations
This qualitative study included only 15 women with breast cancer and may not be generalizable to all breast cancer patients or individuals with other cancer types. However, it is worth noting that we reached saturation (no new themes emerged) [36] after 13 interviews and feel confident that our study represents a valid view of patient-reported challenges and needs for diabetic patients undergoing breast cancer chemotherapy. We did not ask participants about their diabetes management patterns before being diagnosed with cancer so we are unable to describe changes that occurred after cancer. Additionally, as we were focused on diabetes and breast cancer, we did not collect information about other comorbid conditions.
Strengths
The racial/ethnic diversity of our study sample (70% are Black, Hispanic/Latino or Asian/Pacific Islander) is an important strength, as we were able to capture challenges experienced and needs/priorities for this population, which is also at highest risk of complications of diabetes and breast cancer treatment. Additionally, these findings will directly inform the development of an intervention, which helps ensure the intervention will be patient-centered and responsive to patients needs/priorities.
Conclusion
We found that patients with diabetes undergoing breast cancer chemotherapy experience distress when their blood sugar becomes uncontrolled and feel that they have unmet educational and monitoring needs, which should be addressed. The next step in this line of scientific inquiry is to take these patient insights to develop strategies to better support diabetes management during cancer treatment for women with diabetes undergoing cancer chemotherapy. Oncology providers should consider these patient-reported challenges when caring for patients with cancer and comorbid diabetes, as they may benefit from additional support and guidance managing both conditions during chemotherapy.
Data Availability
Given the qualitative study design and relatively small sample (N=15), data are not available in order to ensure participant confidentiality.
References
Giovannucci E et al (2010) Diabetes and cancer: a consensus report. Diabetes Care 33(7):1674–1685
Edwards BK et al (2014) Annual Report to the Nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 120(9):1290–1314
Srokowski TP et al (2009) Impact of diabetes mellitus on complications and outcomes of adjuvant chemotherapy in older patients with breast cancer. J Clin Oncol 27(13):2170–2176
Gold HT et al (2014) Treatment and outcomes in diabetic breast cancer patients. Breast Cancer Res Treat 143(3):551–570
Barone BB et al (2010) Postoperative mortality in cancer patients with preexisting diabetes: systematic review and meta-analysis. Diabetes Care 33(4):931–939
Hershey DS (2017) Importance of glycemic control in cancer patients with diabetes: treatment through end of life. Asia Pac J Oncol Nurs 4(4):313–318
Safford MM et al (2005) How much time do patients with diabetes spend on self-care? J Am Board Fam Pract 18(4):262–270
Hershey DS et al (2012) Perceived impact of cancer treatment on diabetes self-management. Diabetes Educ 38(6):779–790
Ritchie CS, Kvale E, Fisch MJ (2011) Multimorbidity: an issue of growing importance for oncologists. J Oncol Pract 7(6):371–374
Pinheiro LC et al (2019) Determining the impact of a cancer diagnosis on diabetes management: a systematic literature review. Am J Clin Oncol 42(11):870–883
Goebel J, Valinski S, Hershey DS (2016) Improving coordination of care among healthcare professionals and patients with diabetes and cancer. Clin J Oncol Nurs 20(6):645–651
Cho J et al (2021) Eliciting primary care and oncology provider perspectives on diabetes management during active cancer treatment. Support Care Cancer 29(11):6881–6890
Earle CC, Neville BA (2004) Under use of necessary care among cancer survivors. Cancer 101(8):1712–1719
Potosky AL et al (2011) Differences between primary care physicians’ and oncologists’ knowledge, attitudes and practices regarding the care of cancer survivors. J Gen Intern Med 26(12):1403–1410
Charlot M et al (2017) Diabetes and breast cancer mortality in Black women. Cancer Causes Control 28(1):61–67
Pinheiro LC et al (2020) Diabetes care management patterns before and after a cancer diagnosis: a SEER-Medicare matched cohort study. Cancer 126(8):1727–1735
Guest G, Namey E, Chen M (2020) A simple method to assess and report thematic saturation in qualitative research. PLoS One 15(5):e0232076
GitHub, Inc. Qual-code visualizer. Available from: https://github.com/emtseng/qual-code-visualizer. Accessed 6 Jan 2022
Hesketh PJ (2008) Chemotherapy-induced nausea and vomiting. N Engl J Med 358(23):2482–2494
Vigneri P et al (2009) Diabetes and cancer. Endocr Relat Cancer 16(4):1103–1123
Poulson J (1997) The management of diabetes in patients with advanced cancer. J Pain Symptom Manage 13(6):339–346
Jeong Y et al (2016) A pilot study evaluating steroid-induced diabetes after antiemetic dexamethasone therapy in chemotherapy-treated cancer patients. Cancer Res Treat 48(4):1429–1437
Brunello A, Kapoor R, Extermann M (2011) Hyperglycemia during chemotherapy for hematologic and solid tumors is correlated with increased toxicity. Am J Clin Oncol 34(3):292–296
van de Poll-Franse LV et al (2007) Less aggressive treatment and worse overall survival in cancer patients with diabetes: a large population based analysis. Int J Cancer 120(9):1986–1992
Peyrot M et al (2005) Psychosocial problems and barriers to improved diabetes management: results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diabet Med 22(10):1379–1385
Smith HR (2015) Depression in cancer patients: pathogenesis, implications and treatment (Review). Oncol Lett 9(4):1509–1514
Brintzenhofe-Szoc KM et al (2009) Mixed anxiety/depression symptoms in a large cancer cohort: prevalence by cancer type. Psychosomatics 50(4):383–391
Pinquart M, Duberstein PR (2010) Depression and cancer mortality: a meta-analysis. Psychol Med 40(11):1797–1810
Linden W et al (2012) Anxiety and depression after cancer diagnosis: prevalence rates by cancer type, gender, and age. J Affect Disord 141(2–3):343–351
Richardson GC et al (2014) Nurse practitioner management of type 2 diabetes. Perm J 18(2):e134–e140
Li S et al (2017) The effect of nurse practitioner-led intervention in diabetes care for patients admitted to cardiology services. Can J Diabetes 41(1):10–16
New JP et al (2003) Specialist nurse-led intervention to treat and control hypertension and hyperlipidemia in diabetes (SPLINT): a randomized controlled trial. Diabetes Care 26(8):2250–2255
Nelson E et al (2018) Optimizing adult diabetes care in community health. J Am Assoc Nurse Pract 30(8):443–449
McCorkle R et al (2012) Transition to a new cancer care delivery system: opportunity for empowerment of the role of the advanced practice provider. J Adv Pract Oncol 3(1):34–42
Pinheiro LC et al (2022) Managing diabetes during treatment for breast cancer: oncology and primary care providers’ views on barriers and facilitators. Support Care Cancer 30(8):6901–6908
Guest G, Bunce A, Johnson L (2006) How many interviews are enough? An experiment with data saturation and variability. Field Methods 18(1):59–82
Funding
This work was supported by the National Cancer Institute at the National Institutes of Health (NCI) (K01 CA251645).
Author information
Authors and Affiliations
Contributions
Laura Pinheiro, Lisa Kern, and Monika Safford led the study conception and design. Material preparation, data collection, and analysis were performed by Jacklyn Cho, Micayla Wilson, Julia Rothman, Caroline Zeng, and Laura C. Pinheiro. The first draft of the manuscript was written by Laura C. Pinheiro, Jacklyn Cho, Julia Rothman, and Caroline Zeng. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study design and methodology for this study were approved by the Weill Cornell Institutional Review Board (20–03021654). Informed consent was obtained from all participants in the study. All participants provided written consent to participate in the study and publish de-identified excerpts from the interviews.
Conflict of interest
Dr. Safford, receives salary support for investigator-initiated research from Amgen, Inc. Dr. Pinheiro receives salary support for investigator-initiated research from Pfizer. The other co-authors have no conflicts of interest to disclose.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Pinheiro, L.C., Cho, J., Rothman, J. et al. Diabetes and cancer co-management: patient-reported challenges, needs, and priorities. Support Care Cancer 31, 145 (2023). https://doi.org/10.1007/s00520-023-07604-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00520-023-07604-x