
Abstract
Purpose
To evaluate the evidence from randomized clinical trials (RCTs) about the effect of music intervention in reducing patients’ anxiety during breast biopsy.
Methods
Electronic databases including PubMed, Cochrane Library, Scopus, and Web of Science were searched using the relevant MeSH terms. The inclusion criteria were all RCTs assessing the effect of music therapy versus no music in reducing anxiety during breast biopsy. The extracted outcomes were anxiety and pain during breast biopsy. They were pooled as mean difference (MD) with a 95% confidence interval (CI) in a fixed-effects model, using Review Manager 5.3 software for windows. The quality of included studies was assessed with the Cochrane risk of bias assessment tool (RoB 1.0). Then, the outcomes of our meta-analyses were independently evaluated by the Grading of Recommendations Assessment, Development and Evaluation (GRADE) to know the grade of their evidence.
Results
The final analysis included five RCTs. We found a positive effect of music therapy in reducing anxiety levels compared with control group (MD = − 2.11; 95% CI (− 4.16 to − 0.06); p = 0.04). No difference between music and control groups regarding pain associated with breast biopsy (MD = 0.22; 95% CI (− 0.81 to 1.25); p = 0.68). The GRADE rating of our outcomes was low for anxiety levels and very low for pain during the biopsy.
Conclusions
Music therapy could be an effective, simple, non-pharmacological option in relieving anxiety during breast biopsy; however, it had no effect on procedure-associated pain. More large and high-quality studies are needed to confirm our results.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A breast biopsy is a procedure in which a sample of breast tissue is extracted and prepared to be sent to further laboratory testing [1]. The most frequent indication for breast biopsy is the suspicion of malignant lesions by screening mammography [2].
Breast cancer is the second most commonly diagnosed cancer worldwide, including low- and middle-income countries [3]. The incidence rates are highest in North America, Australia/New Zealand, and western and northern Europe and lowest in Asia and sub-Saharan Africa [4]. Notably, it became a significant public health issue due to its associated high morbidity, mortality, and massive health costs. Managing the psychological health of women is of extreme importance in all the stages of the disease, starting from the first suspicion to the different treatment modalities. Anxiety, cognitive defense, and emotion-focused coping are usually witnessed among patients with suspected breast cancer awaiting diagnosis [5]. In particular, prior to breast biopsy, patients experience general anxiety and specific worry about both the procedure itself and the biopsy results (i.e., the diagnosis) [6]. Such anticipatory emotional distress has been related to poorer biopsy-related outcomes, including increased pain and physical discomfort [7].
At present, tissue biopsy is a very useful clinical tool that can assist with critical clinical decision-making in patients with suspicious lesions. In the USA, 1.7 million women undergo breast biopsies each year [8]. Breast biopsy methods include core needle biopsy (CNB), fine needle aspiration (FNA), surgical biopsy, and skin punch biopsy [9]. The difference between CNB and FNA is the size of the needle. Both procedures do not require incisions, unlike the open (surgical) biopsy in which a cut is made in the breast. These techniques are usually done with the help of guided tools such as vacuum-assisted or ultrasound-guided biopsies [9, 10].
Although the biopsy is a simple technique that can only induce slight damage, its adverse biopsy-related outcomes cannot be neglected. Breast biopsy patients typically have substantial levels of anticipatory emotional distress [11]. Moreover, a painful feeling after the biopsy is another chief complaint of patients [12]. Several studies reported that pain perception ranges from 2.0 to 5.8 out of 10 during imaging-guided breast biopsy and 3.3 to 4.6 out of 10 for vacuum-assisted (VA) biopsies [13,14,15]. Therefore, emotional distress and pain have been the most challenging problems of the biopsy, which need to be urgently resolved. Effectively managing the perception of pain is important for the good sake of the patients and could eventually affect patient satisfaction and the practice revenues.
Pain is a subjective and complex phenomenon, and its perception could be influenced by genetic, developmental, familial, psychological, social, and cultural variables [16]. Several pharmacological and non-pharmacological interventions could help minimize the sensation of pain, including listening to music [17]. Music therapy is an easily accessible and inexpensive method used by many people to regulate moods and emotions in their daily lives [18]. To date, music interventions have been widely used in health care. Cochrane reviews have demonstrated beneficial effects of listening to music on anxiety in patients with cancer, coronary heart disease, or preoperative anxiety [19,20,21].
There is controversy regarding the role of music in patients undergoing breast biopsy. While music had promising results in reducing pain and anxiety during breast biopsy [22], other recent RCTs concluded that music intervention has no impact on pain perception [23, 24]. Therefore, we aimed to synthesize evidence on the role of music therapy in reducing anxiety and pain of patients undergoing breast biopsy.
Methods
Study design
This is a systematic review and meta-analysis study for all RCTs showing the effect of music on reducing pain and anxiety in women undergoing breast biopsy. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in this study [25]. Because the study was a systematic review, it was exempt from ethics approval and obligate protocol registration. Therefore, the study’s protocol was not online registered.
Search strategy
We performed a comprehensive and systematic search of four electronic databases, PubMed, Cochrane CENTRAL Library, Scopus, and Web of Science, from their inception till September 2021, without language restrictions. The following keywords were used: ((Breast OR breasts) AND (biopsy OR “Fine needle aspiration” OR FNA OR “Core needle biopsy”)) AND (pain OR pains OR Suffering OR Ache OR Aches OR Anxiety OR Angst OR Nervousness OR Hypervigilance OR Anxiousness OR Anxieties) AND (music OR Symphony OR Rhythm OR Orchestra OR Song OR (Vocal AND (Melodies OR Melody))). In addition, we searched the references of relevant articles for potentially relevant studies.
Eligibility criteria
The inclusion criteria were as follows: (1) studies including women undergoing breast biopsy; (2) studies in which music interventions such as music, song, or any equivalent were applied during breast biopsy; (3) studies including a control group without music interventions; (4) studies reporting anxiety and pain as their primary outcome; and (5) RCTs. We excluded from our study all non-English studies, non-randomized clinical trials, editorials and animal studies, case reports, case series, notes, letters, posters, thesis, books, conference proceedings. We excluded any paper not reporting enough data to report our included outcomes.
Outcomes
Anxiety and pain outcomes as evaluated by the State anxiety scale (SAS) and visual analogue scale (VAS), respectively. The anxiety change score is the difference in pre-biopsy and post-biopsy anxiety levels.
Study selection and data extraction
We followed a two-stage process for screening and selection of eligible studies after the removal of duplicates. Two reviewers independently screened the titles and abstracts of retrieved search records that agree with the selection criteria in the first stage. In the second stage, the full texts of potentially eligible studies were screened for a final decision about eligibility. If a disagreement occurred, another author was included in the discussion to achieve consensus.
Three authors independently reviewed each included article and extracted the following data using a standardized Microsoft Excel sheet: first author, year of publication, number of enrolled participants, characteristics of participants, details of intervention, and main findings (Table 1). In case of incomplete data, we contacted the original study’s authors to request the missing details.
Quality assessment
We assessed the risk of bias using the Cochrane risk of bias assessment tool (RoB 1.0) described in the Cochrane Handbook for Systematic Reviews of Interventions [26]. Seven domains were evaluated: random sequence generation (selection bias), allocation sequence concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias), and other potential sources of bias. Each domain was judged as having a low, high, or unclear risk of bias. All assessments were independently fulfilled by the same two authors and discrepancies were resolved through discussion. Then, the outcomes of our meta-analyses were independently evaluated by the Grading of Recommendations Assessment, Development and Evaluation (GRADE) to know their grade of the evidence [27].
Publication bias
According to Egger and colleagues, the estimation of publication bias utilizing funnel plot and Egger’s test is unpredictable for less than ten pooled studies. Therefore, in the current study, we could not assess for publication bias by Egger’s test due to the limited number of the studies which met our inclusion criteria [28].
Statistical analysis
Continuous outcomes were pooled as weighted mean difference (WMD) using the Mantel-Hansel method with 95% confidence intervals (CI). Review Manager 5.3 software (Cochrane Information Management System) was used to perform the calculations. Heterogeneity was evaluated graphically using forest plots and statistically using the Cochrane Q test and I2 statistics [29]. In the Q-tests, p < 0.1 and I2 ≥ 50% were considered indicative of statistically significant heterogeneity. Statistically significant results were considered when the p-value was < 0.05.
If there was any heterogeneity between studies, we used the random-effects model; otherwise, the fixed-effects model was utilized. We did the sensitivity analysis to consider the contribution of each included study to the pooled estimation of the reported heterogeneity by removing one trial at a time and reanalyzing the pooled mean difference estimation for the remaining studies.
Results
Search results and characteristics of included studies
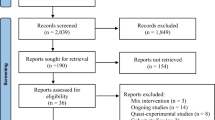
Initially, the search results yielded 121 records. After removing the duplicates, we performed title and abstract screening for 95 studies; only 11 were eligible for full-text screening. Of them, five RCTs (401 patients) were included in the meta-analysis as shown in the PRISMA flow diagram (Fig. 1). The baseline characteristics of patients and a summary of included studies are shown in Table 1.

Study flow diagram (PRISMA)
Risk of bias assessment
Using the risk of bias tool of Cochrane described in Cochrane Handbook for Systematic Reviews of Interventions, we found that the quality of included studies was unclear in selection bias because most of the included studies did not mention the methods of randomization or allocation concealment. There was low quality regarding the performance and detection bias criteria because it was not possible to blind participants, physicians, and the outcomes assessors due to the nature of intervention. There was no attrition or reporting bias except for Benett et al. [30] study which had high risk of bias as there were no data for some patients who had the procedure performed. We considered all included studies as having high risk of other sources of bias due to unavailability of their protocols. The summary of quality assessment domains of included studies is shown in Fig. 2.

Risk of bias summary of the included studies
Outcomes
-
1.
State anxiety score
Pooled data from five studies [22,23,24, 30, 31] (N = 401 patients) showed a lower anxiety score in music group compared with control group (no music) (MD = − 2.11; 95% CI (− 4.16 to − 0.06); p = 0.04; Fig. 3). Pooled studies were homogenous (p = 0.35).
Fig. 3 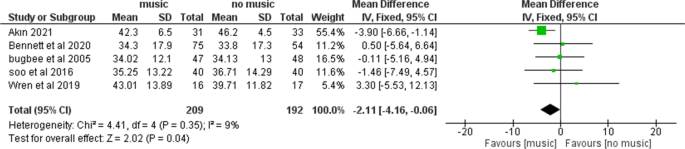
State anxiety score comparing a group of patients who listened to music and another group who did not listen to music during a breast biopsy
-
2.
Anxiety decrease
Anxiety decrease was reported in four studies (178 participants in music group and 159 in control group). The overall effect showed that music significantly reduced anxiety level compared to control (MD = 3.37; 95% CI (0.17 to 6.57); p = 0.04; Fig. 4). Pooled studies were homogenous (p = 0.84).
Fig. 4 
Decrease in state anxiety score comparing a group of patients who listened to music and another group who did not listen to music during a breast biopsy
-
3.
Pain during breast biopsy


Pain levels during the procedure were reported in three studies (87 participants in music group and 90 participants in control group). The pooled MD showed no significant differences in pain scores between both groups (MD = 0.22; 95% CI (− 0.81 to 1.25); p = 0.68; Fig. 5). Pooled studies were heterogeneous under a random effect model (P = 0.04; I2 = 69%).

Visual analogue scale score for pain comparing a group of patients who listened to music and another group who did not listen to music during a breast biopsy
Summary of the findings and GRADE evaluation of the outcomes (Table 2)
All outcomes were evaluated by GRADE criteria. The state anxiety score and decrease in anxiety score showed low quality which indicated that the confidence about the results was limited and the difference between the actual effect and our result could exist. This was because of the increased risk of bias in the included studies and imprecision. In the pain during the breast biopsy, the GRADE rating was very low which indicated that the confidence about the results was very little and the difference between the actual effect and our result was more probably to present. This was because of the increased risk of bias in included studies, imprecision, and heterogeneity.
Discussion
Summary of the results
To our knowledge, there are no other systematic reviews or meta-analyses of RCTs that investigated music intervention for reducing anxiety and pain caused by the biopsy. However, several RCTs with different results have been reported. For this meta-analysis, data across all the included studies were evaluated to verify the role of music intervention with more precision than any single study. Our meta-analysis showed that Music intervention is readily effective in reducing anxiety during the breast biopsy. However, there is no significant difference between both groups regarding pain during the breast biopsy procedure.
Significance of the results
The experience of anxiety before and during the insertion of the biopsy needle is particularly common. Dealing with the fear of needles and anxiety is important to control pain perception since lower levels of anxiety, and anticipated pain is closely related to lower levels of procedure-related pain [32]. Various factors could potentially affect and mediate the perception of stressful events, including coping style, social support, personality type, and gender [33].
For many reasons, non-pharmacological interventions have gained considerable attention in reducing pain and anxiety due to the absence of side effects, lower costs, and ease and comfortable atmosphere they create. Remarkable results have been reported on the use of music intervention as a modality to reduce anxiety. Paskin and Baker’s works showed that relaxing music reduces subjective anxiety in patients compared to those who waited in silence in the surgery waiting room [34]. Several RCTs yielded similar results when applying this intervention during the biopsy procedure, and our results agreed with those deduced from different interventional procedures [35, 36]. Additionally, music intervention showed a potential impact in reducing anxiety during a breast biopsy, as described in our meta-analysis.
Explanation of the results
The anxiolytic effect of music might be due to the modulation of nervous and endocrine systems and its effect on neurotransmitters, hormones, cytokines, and immunoglobulins, as well as a psychological response [37]. Listening to music may suppress the sympathetic system, decreasing the cortisol levels and triggering activity in brain regions linked to emotional experiences and modulating anxiety levels [38]. Music leads to distraction which may mitigate pain by modulating connectivity between pain centers in the brain [39] or simply by making time pass more quickly while waiting for the vacuum-assisted biopsy to finish [30].
A previous systematic review and meta-analysis by Lin et al. [18] showed that music interventions during pregnancy may decrease maternal anxiety. A similar review concluded that music was beneficial in reducing anxiety scores and physiological indexes related to anxiety (e.g., heart rate) in pregnant women undergoing cesarean section or labor process [40].
As for pain perception, our analysis showed no significant effect on pain perception during breast biopsy, and the result is comparable with other meta-analyses performed on biopsies from different body regions [41, 42] despite without controversy [43]. Our results clearly show that pain was not affected with music intervention in breast biopsy. Our results agreed with the results of Abdelhakim et al. [44] systematic review and meta-analysis which concluded that music therapy was ineffective in lowering pain scores during colposcopy procedures.
A recent meta-analysis by Song et al. [36] aimed to evaluate the efficacy of music therapy for reducing the anxiety and pain of patients who underwent a biopsy. Nine RCTs were included. Music was successful in decreasing systolic blood pressure before the biopsy, State-Trait Anxiety Inventory scores after the biopsy, diastolic blood pressure after the biopsy, and heart rate after the biopsy. Similarly, music also tended to be more effective for controlling pain after the biopsy.
It is important to note that individual music preference is important to the effect of a music intervention [30] which was not the case in most of our included RCTs since the music was already chosen by the experimenters [23, 31]. Our pooled results from all the included data support the usefulness of listening to music in reducing patient anxiety during a biopsy to soothe and relieve patients’ feelings, compared with the standard care conditions. Unfortunately, there is no clinical significance in reducing pain perception on VAS score. Furthermore, future studies are warranted to establish more objective pain assessment methods and more ideal techniques for RCTs.
Clinical implications
Music interventions are inexpensive and practical. In addition, they are safer and have no significant side effects compared with pharmacological treatment. Thus, their application in daily care may be advisable for women.
Strengths of the study
The strength of the present study is that we performed comprehensive search of multiple databases without language restrictions. We included five RCTs in the quantitative analysis constituting a strong evidence level.
Study limitations
The main limitations of our study are the relatively small sample size in some trials and the deficiency of blinding and allocation concealment in the risk of bias assessment which is attributed to the difficulty to blind the relevant parties. However, the nature of music interventions makes it difficult to apply double-blinded studies. Although we excluded non-English studies, recent evidence realized that excluding non-English studies does not cause any bias to the meta-analysis results [45]. Another limitation is evaluating pain with a VAS score which is not an objective method and can be influenced by several factors, such as social and cultural status. Another limitation was the lack of a good standard of music intervention, such as playing type, timing, and musical style since diverse music interventions can have different physical, neurological, and psychological states. Also, the GRADE rating of our outcomes was low with state anxiety score and decrease in state anxiety score while it was very low with pain during a breast biopsy. This could be explained by the limited published number of studies related to this topic and the nature of the intervention (music) and control (no music) which made it difficult to blind the study’s personnel, participants, and assessors which increased the risk of bias. Therefore, we recommend performing more studies with a larger population and of high quality.
Conclusion
This systematic review suggests that music therapy has a great positive effect in reducing anxiety levels when compared with control groups during the breast biopsy procedure. However, it has no effect in reducing pain during breast biopsy. The estimate of music intervention effect might be exaggerated because no blinding or allocation concealment was applied in included trials, preventing the analysis of a subjective outcome.
References
Bilous M (2010) Breast core needle biopsy: issues and controversies. Mod Pathol Suppl 2:S36–45. https://doi.org/10.1038/modpathol.2010.34.
Dahabreh IJ, Wieland LS, Adam GP, et al (2014) Core needle and open surgical biopsy for diagnosis of breast lesions: an update to the 2009 report [Internet]. Agency for Healthcare Research and Quality (US). Comparative Effectiveness Reviews, No. 139, Rockville. Available from https://www.ncbi.nlm.nih.gov/books/NBK246878/.
Anderson BO, Yip Ch Fau - Smith RA, Smith Ra Fau - Shyyan R, Shyyan R Fau - Sener SF, Sener Sf Fau - Eniu A, Eniu A Fau - Carlson RW, et al. Guideline implementation for breast healthcare in low-income and middle-income countries: overview of the Breast Health Global Initiative Global Summit 2007. (1097–0142 (Electronic))
Sung HA-O, Ferlay J, Siegel RA-O, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. (1542–4863 (Electronic))
Drageset S, Lindstrøm TC. The mental health of women with suspected breast cancer: the relationship between social support, anxiety, coping and defence in maintaining mental health. (1351–0126 (Print))
Schnur JB, Montgomery Gh Fau - Hallquist MN, Hallquist Mn Fau - Goldfarb AB, Goldfarb Ab Fau - Silverstein JH, Silverstein Jh Fau - Weltz CR, Weltz Cr Fau - Kowalski AV, et al. Anticipatory psychological distress in women scheduled for diagnostic and curative breast cancer surgery. (1070–5503 (Print))
Montgomery GH, Bovbjerg DH. Presurgery distress and specific response expectancies predict postsurgery outcomes in surgery patients confronting breast cancer. (0278–6133 (Print))
Silverstein MJ, Lagios Md Fau - Recht A, Recht A Fau - Allred DC, Allred Dc Fau - Harms SE, Harms Se Fau - Holland R, Holland R Fau - Holmes DR, et al. Image-detected breast cancer: state of the art diagnosis and treatment. (1072–7515 (Print))
Versaggi SL, De Leucio A. Breast Biopsy. BTI - StatPearls
Park HL, Hong J. Vacuum-assisted breast biopsy for breast cancer. (2227–684X (Print))
Lebel S, Jakubovits G Fau - Rosberger Z, Rosberger Z Fau - Loiselle C, Loiselle C Fau - Seguin C, Seguin C Fau - Cornaz C, Cornaz C Fau - Ingram J, et al. Waiting for a breast biopsy. Psychosocial consequences and coping strategies. (0022–3999 (Print))
Tanasale B, Kits J, Kluin PM, Trip A, Kluin-Nelemans HC. Pain and anxiety during bone marrow biopsy. (1532–8635 (Electronic))
Zagouri F, Sergentanis Tn Fau - Gounaris A, Gounaris A Fau - Koulocheri D, Koulocheri D Fau - Nonni A, Nonni A Fau - Domeyer P, Domeyer P Fau - Fotiadis C, et al. Pain in different methods of breast biopsy: emphasis on vacuum-assisted breast biopsy. (0960–9776 (Print))
Zografos GC, Zagouri F Fau - Sergentanis TN, Sergentanis Tn Fau - Nonni A, Nonni A Fau - Domeyer P, Domeyer P Fau - Koulocheri D, Koulocheri D Fau - Flessas I, et al. Pain during vacuum-assisted breast biopsy: are there any predictors? (1532–3080 (Electronic))
Satchithananda K, Fernando Ra Fau - Ralleigh G, Ralleigh G Fau - Evans DR, Evans Dr Fau - Wasan RK, Wasan Rk Fau - Bose S, Bose S Fau - Donaldson N, et al. An audit of pain/discomfort experienced during image-guided breast biopsy procedures. (1075–122X (Print))
McGrath PA. Psychological aspects of pain perception. (0003–9969 (Print))
Deng G. Integrative medicine therapies for pain management in cancer patients. (1540–336X (Electronic))
Lin CA-OX, Chang YC, Chang YH, Hsiao YH, Lin HA-O, Liu SJ, et al. Music interventions for anxiety in pregnant women: a systematic review and meta-analysis of randomized controlled trials. LID - https://doi.org/10.3390/jcm8111884 [doi] LID - 1884. (2077–0383 (Print))
Bradt J, Dileo C Fau - Potvin N, Potvin N. Music for stress and anxiety reduction in coronary heart disease patients. (1469–493X (Electronic))
Bradt J, Dileo C Fau - Magill L, Magill L Fau - Teague A, Teague A. Music interventions for improving psychological and physical outcomes in cancer patients. (1469–493X (Electronic))
Bradt J, Dileo C Fau - Shim M, Shim M. Music interventions for preoperative anxiety. (1469–493X (Electronic))
Wren AA, Shelby RA, Soo MS, Huysmans Z, Jarosz JA, Keefe FJ. Preliminary efficacy of a loving kindness meditation intervention for patients undergoing biopsy and breast cancer surgery: a randomized controlled pilot study. (1433–7339 (Electronic))
Akın ME. Effect of music on anxiety and pain during ultrasound-guided core needle breast biopsy: a randomized controlled trial. (1305–3612 (Electronic))
Soo MS, Jarosz JA, Wren AA, Soo AE, Mowery YM, Johnson KS, et al. Imaging-guided core-needle breast biopsy: impact of meditation and music interventions on patient anxiety, pain, and fatigue. (1558–349X (Electronic))
Page MA-O, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. (1756–1833 (Electronic))
Higgins JP, Altman Dg Fau - Gøtzsche PC, Gøtzsche Pc Fau - Jüni P, Jüni P Fau - Moher D, Moher D Fau - Oxman AD, Oxman Ad Fau - Savovic J, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. (1756–1833 (Electronic))
Zhang YA-O, Akl EA, Schünemann HJ. Using systematic reviews in guideline development: the GRADE approach. LID - https://doi.org/10.1002/jrsm.1313 [doi]. (1759–2887 (Electronic))
Egger M, Davey Smith G Fau - Schneider M, Schneider M Fau - Minder C, Minder C. Bias in meta-analysis detected by a simple, graphical test. (0959–8138 (Print))
Higgins JP, Thompson Sg Fau - Deeks JJ, Deeks Jj Fau - Altman DG, Altman DG. Measuring inconsistency in meta-analyses. (1756–1833 (Electronic))
Bennett DL, Swan JS, Gazelle GS, Saksena M. Music during image-guided breast biopsy reduces patient anxiety levels. (1873–4499 (Electronic))
Bugbee ME, Wellisch DK, Arnott IM, Maxwell JR, Kirsch DL, Sayre JW, Bassett LW (2005) Breast core-needle biopsy: clinical trial of relaxation technique versus medication versus no intervention for anxiety reduction. Radiology 234(1):73–78. https://doi.org/10.1148/radiol.2341030163.
Maimone S, Morozov AP, Wilhelm A, Robrahn I, Whitcomb TD, Lin KY et al (2020) Understanding patient anxiety and pain during initial image-guided breast biopsy. J Breast Imaging 2(6):583–589
Knight WE, Rickard PhD NS (2001)Relaxing music prevents stress-induced increases in subjective anxiety, systolic blood pressure, and heart rate in healthy males and females. J Music Ther 38(4):254–272. https://doi.org/10.1093/jmt/38.4.254.
Winter Mj Fau - Paskin S, Paskin S Fau - Baker T, Baker T. Music reduces stress and anxiety of patients in the surgical holding area. (0883–9433 (Print))
Kühlmann AA-O, de Rooij AA-O, Kroese LA-O, van Dijk MA-O, Hunink MA-O, Jeekel J. Meta-analysis evaluating music interventions for anxiety and pain in surgery. (1365–2168 (Electronic))
Song M, Li N, Zhang X, Shang Y, Yan L, Chu J, et al. Music for reducing the anxiety and pain of patients undergoing a biopsy: A meta-analysis. (1365–2648 (Electronic))
Fancourt D, Ockelford A, Belai A. The psychoneuroimmunological effects of music: a systematic review and a new model. (1090–2139 (Electronic))
Thoma MV, La Marca R Fau - Brönnimann R, Brönnimann R Fau - Finkel L, Finkel L Fau - Ehlert U, Ehlert U Fau - Nater UM, Nater UM. The effect of music on the human stress response. (1932–6203 (Electronic))
Valet M, Sprenger T Fau - Boecker H, Boecker H Fau - Willoch F, Willoch F Fau - Rummeny E, Rummeny E Fau - Conrad B, Conrad B Fau - Erhard P, et al. Distraction modulates connectivity of the cingulo-frontal cortex and the midbrain during pain--an fMRI analysis. (0304–3959 (Print))
Lin HA-O, Chang YC, Chou HH, Chang CP, Huang MY, Liu SA-O, et al. Effect of music interventions on anxiety during labor: a systematic review and meta-analysis of randomized controlled trials. (2167–8359 (Print))
Packiam VT, Nottingham CU, Cohen AJ, Eggener SE, Gerber GS. No effect of music on anxiety and pain during transrectal prostate biopsies: a randomized trial. (1527–9995 (Electronic))
Danhauer SC, Vishnevsky T, Campbell CR, McCoy TP, Tooze JA, Kanipe KN, et al. Music for patients with hematological malignancies undergoing bone marrow biopsy: a randomized controlled study of anxiety, perceived pain, and patient satisfaction. (1715–894X (Print))
Shabanloei R, Golchin M Fau - Esfahani A, Esfahani A Fau - Dolatkhah R, Dolatkhah R Fau - Rasoulian M, Rasoulian M. Effects of music therapy on pain and anxiety in patients undergoing bone marrow biopsy and aspiration. (1878–0369 (Electronic))
Abdelhakim AM, Samy A, Abbas AM. Effect of music in reducing patient anxiety during colposcopy: a systematic review and meta-analysis of randomized controlled trials. (2468–7847 (Electronic))
Moher D, Pham B, Klassen TP, Schulz KF, Berlin JA, Jadad AR, Liberati A (2000) What contributions do languages other than English make on the results of meta-analyses?. J Clin Epidemiol 53(9):964–972. https://doi.org/10.1016/s0895-4356(00)00188-8.
Acknowledgements
The authors would like to thank Mrs. Yasmin Negm (Helwan, Egypt) for her invaluable efforts in recording and organizing study data and computer works.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Ahmed SA Ashour, Hany Saad, Mariam Yohanna, Mostafa El-Nagar, Yassamine Ouerdane, Ahmed Nasser Fadl, Mona Fouad, Iman Ezahaby, and Noura El-Nassery. The first draft of the manuscript was written by Mohamed Abdelmonem Kamel, Mohamed Abd-ElGawad, and Gehad Mohammed Goda. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
This is a systematic review and meta-analysis and no ethical approval was required.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Synopsis: Music therapy could be an effective, simple, non-pharmacological intervention for relieving anxiety during breast biopsy; however, it has no effect on procedure-associated pain.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ashour, A.S.A., Abd-ElGawad, M., Yohanna, M. et al. Is music intervention effective in reducing anxiety and pain during breast biopsy procedure? A systematic review and meta-analysis of randomized controlled trials. Support Care Cancer 30, 10379–10389 (2022). https://doi.org/10.1007/s00520-022-07414-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-022-07414-7