
Abstract
Purpose
Evidence has shown that cancer-related fatigue (CRF) may be a treatment-limiting symptom and often impairs health-related quality of life. Accurate assessment of the multidimensional nature of CRF could help drive interventions to mitigate this debilitating symptom. Currently, there are no clinical tools to effectively and efficiently assess the multidimensionality of CRF. The purpose of this paper is to introduce a CRF-specific short form that can assess the multidimensional nature of CRF for use in the clinical setting.
Methods
The CRF-specific short form was developed using the 95-item PROMIS® fatigue bank. Bi-factor analysis was used to evaluate dimensionality of the alternative model using fatigue for the general factor and physical, cognitive, affective, global, and motivational for the local factors. After unidimensionality was confirmed (loading factor > 0.3), one item from each local factor was selected using discrimination power for inclusion in the CRF-specific short form.
Results
The Research Assessment and Clinical Tool-Fatigue (ReACT-F) was created from the 95-item PROMIS fatigue bank using established item parameters. The ReACT-F assesses five common dimensions of CRF as well as perceived burden of the fatigue dimensions.
Conclusions
The ReACT-F is a CRF-specific self-report short form that addresses the need for a brief, clinically useful tool to quickly assess the multidimensional nature of CRF. We anticipate that the ReACT-F can be completed in the clinical setting in approximately 3 minutes, providing clinicians with meaningful data to drive personalized interventions. Further validation of the ReACT-F is highly encouraged.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancer-related fatigue (CRF) is a highly prevalent, complex, multidimensional symptom that can greatly impair the health-related quality of life of cancer patients [1, 2]. Clinical guidelines have adopted a single-item, 0 to 10 numeric rating scale to initially screen for CRF due to its easily administered nature [3,4,5,6]. Several guidelines recommend a more comprehensive evaluation when patients rate their fatigue ≥ 4 (i.e., moderate fatigue) using a 0–10 numerical rating scale. This evaluation includes a focused history, assessment of treatable contributing factors (anemia, nutrition deficits, pathologic/physiologic abnormalities, etc.), and concurrent symptoms (pain, depression, sleep disturbance, etc.) and conditions (cardiac, renal, pulmonary, etc.) [3,4,5,6]. Moreover, inclusion of a measure of the multidimensional nature of CRF would be advantageous to understand the full fatigue experience of cancer patients.
The fatigue experienced by cancer patients is often reported to be multidimensional in nature including physical, emotional, and cognitive dimensions, although the exact terminology for each dimension can vary (i.e., affective, motivational, behavioral, functional, etc.) [7, 8]. Therefore, when conducting an in-depth evaluation of CRF, clinicians should consider the multidimensional nature of CRF to fully capture the CRF experience and optimize management. Consistent with the Precision Medicine Initiative of the National Institutes of Health (NIH), understanding the specific dimension of CRF that most affects the patient can help guide the clinician to develop a more tailored and personalized management strategy.
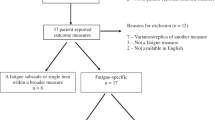
Though comprehensive multidimensional fatigue assessments are available (e.g., revised Piper Fatigue Scale, Multidimensional Fatigue Inventory, and the Fatigue Questionnaire), most of them were developed using classical test theory resulting in measures that may not be best suited for a clinical environment [9]. Applications from the PROMIS® (Patient-Reported Outcomes Measurement Information System, http://www.healthmeasures.net) fatigue item bank are expected to overcome these limitations [10]. As part of the NIH’s roadmap project, the PROMIS® was developed to offer a set of person-centered measures to evaluate symptoms of individuals with or without chronic conditions [11]. One of these measures is the PROMIS instrument that assesses fatigue and the impact of fatigue on daily living [10]. The PROMIS fatigue bank consists of 95 items generated from a comprehensive literature review, focus groups, and individual interviews which were then calibrated using item response theory (IRT) models [10, 12], allowing for brief-yet-precise fatigue estimation via tailored, individualized computer adaptive test (CAT), or short forms with fixed numbers of items. For the latter, multiple short forms can be created to meet users’ needs and scores from these short forms are comparable as long as scores are generated using item parameters established in the original calibrated item banks. Yet precision levels may vary as demonstrated in Lai et al. (2011) in which three short forms were developed targeting patients with mild fatigue, severe fatigue, and for fatigue across the whole severity continuum. Several short forms derived from the PROMIS fatigue item bank are available [13,14,15], yet none of them target fatigue content areas that are important to cancer patients. Therefore, to fill this void, a content-specific CRF short-form was developed that can be used in the clinical setting.
Methods
Fatigue dimensions
To determine the fatigue dimensions of interest, current multidimensional fatigue assessments were reviewed (Table 1) [16,17,18,19,20,21]. The most commonly assessed fatigue dimension was physical (20/20) followed by cognitive (16/20), affective (7/20), global (6/20), and motivational (5/20). Thus, these five dimensions were selected moving forward. The physical dimension of CRF was conceptualized as fatigue related to energy level. The cognitive dimension of CRF was conceptualized as fatigue related to thought processes, memory, and executive function. The affective dimension of CRF was conceptualized as fatigue related to emotions or feelings. The global dimension of CRF was conceptualized as encompassing the subjective experience of fatigue. Lastly, the motivational dimension of CRF was conceptualized as fatigue related to actions that maintain a meaningful or purposeful existence.
Assigning PROMIS fatigue items
All 95 items in the PROMIS fatigue item bank were reviewed by the primary author (KD), who then assigned them to one of the five dimensions. This classification was then reviewed by the second author (DLK) for consensus. If there was disagreement with any classification, a third reviewer (LS) was included to achieve consensus.
Statistical analysis
The current PROMIS fatigue item bank was modeled to have one general fatigue factor with two local factors (experiences and impacts), which was psychometrically proven to be sufficiently unidimensional [10]. For this paper, in order to develop a content-specific CRF short form that produces scores comparable to the PROMIS fatigue item bank and its short forms, we first evaluated the sufficient dimensionality of the alternative model as discussed above using bi-factor analysis.
Bi-factor analysis includes two classes of factors: a general factor, defined by loadings from all of the items in the scale, and local factors, defined by loadings from pre-specified groups of items related to that sub-domain [22,23,24,25]. Items are considered sufficiently unidimensional when standardized loadings are > 0.3 for all the items on the general factor. Similarly, if the loadings of all the items on a local factor are salient, this would indicate that the local factor is well defined even in the presence of the general factor, and it is more appropriate to report scores of local factors separately [22, 24, 26].
In the model used by the current study, the general factor was “fatigue” and the 5 local factors were physical, cognitive, affective, global, and motivational. Once sufficient unidimensionality was supported, we then created a content-specific CRF short form by selecting items from each local factor by reviewing item content, as well as using item parameter threshold values obtained from item response theory (IRT) estimation, particularly the discrimination parameter.
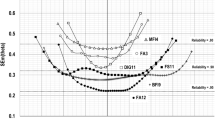
Discrimination power describes the strength of an item’s discrimination between people at different fatigue levels below and above the threshold, indicating the degree of association between item responses and the fatigue latent trait. Items with the highest discrimination parameters typically produce the highest information function (i.e., lowest measurement errors) were considered the best candidates to be included in the short form.
Results
The 95 items from the PROMIS fatigue bank were organized into the five fatigue dimensions (physical, cognitive, affective, global, and motivational) as listed in Table 2. After consensus was achieved, there were 12 items from the PROMIS fatigue bank that fit into the physical dimension, 13 in the cognitive dimension, 4 in the affective dimension, 32 for the global dimension, and 34 for the motivational dimension. Essential dimensionality of these items was supported with acceptable fit indices: RMSEA = 0.04, CFI = 0.985, TLI = 0.985. All items showed higher loading to the general factor than to their own local factor indicating the existing PROMIS item parameters are valid on this alternative model. See Table 3 for a summary of the PROMIS item selection information.
The PROMIS-based Research Assessment and Clinical Tool-Fatigue (ReACT-F) CRF-specific short form was created using established item parameters (Fig. 1). Each item was selected based upon the discriminative value and is considered representative to each fatigue dimension. We added a numeric rating scale at the beginning of the questionnaire per the current fatigue assessment guidelines and we added an additional item, “Which aspect of fatigue is most bothersome to you” to assess the overall burden of the CRF dimensions and inform treatment decisions to optimize CRF management.

Research Assessment and Clinical Tool-Fatigue (ReACT-F). To obtain permission to use, please contact the corresponding author© K. Dickinson, D. Lynch Kelly, J-S. Lai, L. Saligan
Scoring
This short form can be scored using similar approaches as used by other PROMIS fatigue short forms [27]. A 5-item questionnaire can only be scored when at least 4 of the items are completed. However, patients should be encouraged to complete all items to minimize measurement errors. Each question has a Likert scale with values ranging from one to five. A total raw score is calculated by summing the five items on the questionnaire and a prorated value will be used to replace missing value; therefore, the total score on the instrument ranges from 5 to 25. Higher scores indicate worse fatigue. A raw score can then be translated into a PROMIS based T-score to create the final score for a respondent (details are shown in www.healthmeasures.net/score-and-interpret/calculate-scores).
Discussion
The purpose of this paper was to develop a brief tool to capture the multidimensional nature of CRF. This was carried out by examining items included in the 95-item PROMIS fatigue bank to determine if specific items could be selected to measure different fatigue dimensions. The final CRF assessment tool, the ReACT-F, consists of five PROMIS items, where each item is expected to screen a specific dimension of CRF: physical, cognitive, affective, global, and motivational.
The ReACT-F is a self-report short form that addresses the previously identified gap in the literature, which is the lack of a brief, clinically useful tool to quickly assess the multidimensional nature of fatigue in the cancer population. This new content-specific short form requires further validation to determine its clinical and scientific relevance. In the clinic, it is expected that the ReACT-F can aid clinicians to quickly assess the specific fatigue experience of their patients to allow for a more focused evaluation and tailored management. For example, patients reporting physical fatigue may be further evaluated for deconditioning, cardiopulmonary status, or musculoskeletal impairment, so physical rehabilitative strategies can be planned. Individuals who report affective fatigue may be referred for comprehensive psychological evaluation, while those who report affective fatigue or cognitive fatigue may benefit from occupational psychotherapy for behavioral adaptive coaching and a neuropsychology consult for comprehensive cognitive function evaluation, respectively.
Scientifically, this evaluation tool will be useful to determine the phenotypic characteristics of each fatigue dimension within the global fatigue construct. The ReACT-F tool can assist in identifying clinical and demographic attributes, as well as the biologic profile of the specific fatigue experience, to advance our understanding of the etiology of CRF. Understanding the etiology of CRF is important for treatment development and generation of algorithms to identify individuals at risk to develop clinically meaningful fatigue related to the progression of their disease or as a side effect of their treatment.
Limitations
The five items have high discriminative value demonstrating the ability to allow for the assessment of multidimensions of fatigue; however, they did not have sufficient power when factor loading to be independent from the construct of fatigue, as assessed through comparison of factor loadings between the general factor (fatigue) and the local (subdomain) factors. Thus, the dimensions are not independent constructs, but components of a general fatigue construct.
Conclusions
In conclusion, the ReACT-F is a CRF-specific self-report short form that addresses the need for a brief, clinically useful tool to quickly assess the multidimensional nature of CRF. The ReACT-F assesses five common dimensions of CRF as well as perceived burden of the fatigue dimensions. This tool has clinical and scientific promise, to advance our understanding and management of CRF. We anticipate that the ReACT-F can be completed in the clinical setting in approximately 3 minutes, providing clinicians with meaningful data to drive personalized interventions. Further validation of the ReACT-F is highly encouraged to assess its psychometric properties and determine its clinical utility.
References
Berger AM, Mitchell SA, Jacobsen PB, Pirl WF (2015) Screening, evaluation, and management of cancer-related fatigue: ready for implementation to practice? CA Cancer J Clin 65:190–211. https://doi.org/10.3322/caac.21268
Filler K, Saligan LN (2016) Defining cancer-related for biomarker discovery. Support Care Cancer 24:5–7. https://doi.org/10.1007/s00520-015-2965-5
National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology (2018) Cancer-related fatigue, version 2.2018. Available from URL: https://www.nccn.org/professionals/physician_gls/pdf/fatigue.pdf. Accessed Jun 4, 2018
National Cancer Institute (2017) Fatigue (PDQ®)–health professional version. Available from URL: https://www.cancer.gov/about-cancer/treatment/side-effects/fatigue/fatigue-hp-pdq. Accessed Jun 4, 2018
Howell D, Keshavarz H, Broadfield L, et al. on behalf of the Cancer Journey Advisory Group of the Canadian Partnership Against Cancer. A Pan Canadian Practice Guideline for Screening, Assessment, and Management of Cancer-Related Fatigue in Adults Version 2-2015, Toronto: Canadian Partnership Against Cancer (Cancer Journey Advisory Group) and the Canadian Association of Psychosocial Oncology, April 2015. Available from URL: https://www.capo.ca/pdf/CRF_Guideline.pdf. Accessed Jun 4, 2018
Bower J, Bak K, Berger A et al (2014) Screening, assessment, and management of fatigue in adult survivors of cancer: an American Society of Clinical Oncology clinical practice guideline adaptation. J Clin Oncol 32:1840–1850. https://doi.org/10.1200/JCO.2013.53.4495
Jean-Pierre P, Figueroa-Moseley CD, Kohli S, Fiscella K, Palesh OG, Morrow GR (2007) Assessment of cancer-related fatigue: implications for clinical diagnosis and treatment. Oncologist 12(Suppl 1):11–21
Strasser F, Müller-Käser I, Dietrich D (2009) Evaluating cognitive, emotional, and physical fatigue domains in daily practice by single-item questions in patients with advanced cancer: a cross-sectional pragmatic study. J Pain Symptom Manag 38:505–514. https://doi.org/10.1016/j.jpainsymman.2008.12.009
Minton O, Stone P (2009) A systematic review of the scales used for the measurement of cancer-related fatigue (CRF). Ann Oncol 20:17–25. https://doi.org/10.1093/annonc/mdn537
Lai JS, Cella D, Choi S et al (2011) How item banks and their application can influence measurement practice in rehabilitation medicine: a PROMIS Fatigue item bank example. Arch Phys Med Rehabil 92(Suppl 10):S20–S27. https://doi.org/10.1016/j.apmr.2010.08.033
Cella D, Riley W, Stone AA, Rothrock N, Reeve B, Yount S, Amtmann D, Bode R, Buysse D, Choi S, Cook K, Devellis R, DeWalt D, Fries JF, Gershon R, Hahn EA, Lai JS, Pilkonis P, Revicki D, Rose M, Weinfurt K, Hays R, PROMIS Cooperative Group (2010) The Patient Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005-2008. J Clin Epidemiol 63:1179–1194. https://doi.org/10.1016/j.jclinepi.2010.04.011
Junghaenel DU, Christodoulou C, Lai JS, Stone AA (2011) Demographic correlates of fatigue in the US general population: results from the Patient-Reported Outcomes Measurement Information System (PROMIS) initiative. J Psychosom Res 71:117–123. https://doi.org/10.1016/j.jpsychores.2011.04.007
Garcia SF, Cella D, Clauser SB, Flynn KE, Lad T, Lai JS, Reeve BB, Wilder Smith A, Stone AA, Weinfurt K (2007) Standardizing patient-reported outcomes assessment in cancer clinical trials: a PROMIS initiative. J Clin Oncol 25:5106–5112
Ameringer S, Elswick RK Jr, Menzies V, Robins JL, Starkweather A, Walter J, Gentry AE, Jallo N (2016) Psychometric evaluation of the PROMIS Fatigue-short form across diverse populations. Nurs Res 65:279–289. https://doi.org/10.1097/NNR.0000000000000162
Cook KF, Bamer AM, Roddey TS, Kraft GH, Kim J, Amtmann D (2012) A PROMIS Fatigue short form for use by individuals who have multiple sclerosis. Qual Life Res 21:1021–1030. https://doi.org/10.1007/s11136-011-0011-8
Elbers RG, Rietberg MB, van Wegen EE et al (2012) Self-report fatigue questionnaires in multiple sclerosis, Parkinson’s disease and stroke: a systematic review of measurement properties. Qual Life Res 21:925–944. https://doi.org/10.1007/s11136-011-0009-2
Dittner AJ, Wessely SC, Brown RG (2004) The assessment of fatigue: a practical guide for clinicians and researchers. J Psychosom Res 56:157–170
Hewlett S, Dures E, Almeida C (2011) Measures of fatigue: Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire (BRAF MDQ), Bristol Rheumatoid Arthritis Fatigue Numerical Rating Scales (BRAF NRS) for severity, effect, and coping, Chalder Fatigue Questionnaire (CFQ), Checklist Individual Strength (CIS20R and CIS8R), Fatigue Severity Scale (FSS), Functional Assessment Chronic Illness Therapy (Fatigue) (FACIT-F), Multi-Dimensional Assessment of Fatigue (MAF), Multi-Dimensional Fatigue Inventory (MFI), Pediatric Quality Of Life (PedsQL) Multi-Dimensional Fatigue Scale, Profile of Fatigue (ProF), Short Form 36 Vitality Subscale (SF-36 VT), and visual analog scales (VAS). Arthritis Care Res (Hoboken) 63(suppl 11):S263–S286. https://doi.org/10.1002/acr.20579
Seyidova-Khoshknabi D, Davis MP, Walsh D (2011) A systematic review of cancer-related fatigue measurement questionnaires. Am J Hosp Palliat Care 28:119–129. https://doi.org/10.1177/1049909110381590
Shahid A, Shen J, Shapiro CM (2010) Measurements of sleepiness and fatigue. J Psychosom Res 69:81–89. https://doi.org/10.1016/j.jpsychores.2010.04.001
Whitehead L (2009) The measurement of fatigue in chronic illness: a systematic review of unidimensional and multidimensional fatigue measures. J Pain Symptom Manag 37:107–128. https://doi.org/10.1016/j.jpainsymman.2007.08.019
McDonald RP (1999) Test theory: a unified treatment. Lawrence Earlbaum Associates, Inc., Mahwah, NJ, pp 142–145
Gibbons R, Hedeker D (1992) Full-information item bi-factor analysis. Psychometrika 57:423–436
Lai JS, Crane PK, Cella D (2006) Factor analysis techniques for assessing sufficient unidimensionality of cancer related fatigue. Qual Life Res 15:1179–1190
Lai JS, Butt Z, Wagner L, Sweet JJ, Beaumont JL, Vardy J, Jacobsen PB, Shapiro PJ, Jacobs SR, Cella D (2009) Evaluating the dimensionality of perceived cognitive function. J Pain Symptom Manag 37:982–995. https://doi.org/10.1016/j.jpainsymman.2008.07.012
Lai JS, Cella D, Crane P (2005) Cancer related fatigue is sufficiently unidimensional for applications requiring unidimensionality. Qual Life Res 14:1990
Patient-Reported Outcomes Measurement Information System (PROMIS) (2018) Fatigue: a brief guide to the PROMIS® Fatigue instruments. Available from URL: http://www.healthmeasures.net/images/PROMIS/manuals/PROMIS_Fatigue_Scoring_Manual.pdf. Accessed Jun 10, 2018
Acknowledgements
This work is fully supported by the Division of Intramural Research of the National Institute of Nursing Research of the NIH, Bethesda, Maryland. Dr. Lai's efforts were supported by a grant from the National Cancer Institute (1U2CCA186878; PI: Cella)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The data used in this publication are publicly available on the “HealthMeasures Dataverse.” “HealthMeasures Dataverse” is a repository of data from self-reported patient assessments evaluating symptoms, well-being, and life satisfaction; physical, mental, and social health; as well as examiner-administered assessments measuring sensory, motor, and cognitive functions. Data from NIH-funded initiatives include PROMIS®, NIH Toolbox, Neuro-QoL, and ASCQ-Me.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Dickinson, K.A., Kelly, D.L., Lai, JS. et al. Development of the PROMIS-based Research Assessment and Clinical Tool-Fatigue (ReACT-F). Support Care Cancer 27, 3375–3383 (2019). https://doi.org/10.1007/s00520-018-4614-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-018-4614-2