
Abstract
Purpose
Breast-cancer-related lymphedema (BCRL) can be a transient or persistent condition. The aims of this study were to (1) identify and weigh the risk factors for persistent lymphedema (PLE) among all patients with BCRL and (2) establish a prediction model for the occurrence of PLE.
Methods
A cohort of 342 patients with BCRL with a median follow-up of 5 years after the onset of swelling was analyzed. PLE was defined as a hardening of the subcutaneous tissue, the persistence of the circumferential difference (CD) between arms, or a flare-up of swelling during follow-up. Multiple logistic regression was used to identify risk factors for PLE, including tumors, treatments, and patient-related factors. The prediction accuracy of the model was assessed using the area under the receiver operating characteristic curve (AUC).
Results
Of the 342 patients with BCRL, 229 (67%) had PLE. Multiple logistic regression analysis revealed that the number of lymph node metastases (p = 0.012), the maximal CD between arms at the first occurrence of swelling (p < 0.001), and the largest difference during follow-up (p < 0.001) were significant predictors for PLE. The corresponding AUC was 0.908. Although inclusion of body weight gains (p = 0.008) and maximal CD at the latest follow-up (p = 0.002) increased the analytical accuracy (AUC = 0.920), the resulting AUC values (p = 0.113) were not significantly different.
Conclusions
BCRL is persistent in two thirds of patients. Patients with more lymph node metastases, weight gain, and larger CD since the onset of swelling and during follow-up have an increased likelihood of developing PLE.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Lymphedema is a distressing side effect of breast cancer and can have a devastating effect on a patient’s quality of life [1, 2]. Although lymphedema is defined as a chronic progressive disorder, most cases of breast-cancer-related lymphedema (BCRL) are mild or vanish spontaneously [3,4,5]. By contrast, in some cases, the condition may fluctuate or increase in severity [4, 6, 7]. Because no cure exists for lymphedema, identifying the underlying risk factors for persistent lymphedema (PLE) is necessary for the development of more efficient surveillance programs [5, 6, 8].
Individual studies have reported that 3–42% of women develop lymphedema after breast cancer treatment [3,4,5,6,7, 9,10,11,12]. This broad range of results may be because (a) lymphedema can be defined and measured in different ways [4, 5, 11, 13], (b) some studies contained a small sample size [3, 10], or (c) the periods of follow-up were different [4, 5, 7,8,9, 11, 12]. A comprehensive meta-analysis revealed that patients receiving axillary lymph node dissection (ALND) were four times more prone to have lymphedema than those who underwent sentinel lymph node dissection (SLNB) [11]. Additionally, tumors spreading to the axillary lymph nodes, higher body mass index (BMI), chemotherapy (CT), and radiotherapy (RT) have all been reported as risk factors for BCRL [6,7,8,9, 14,15,16,17]. Despite these findings, several vital issues must be highlighted: (1) the time between surgery and the onset of BCRL is crucial because it reflects the individual’s functional reserve of their lymphatic system after treatment; (2) taxane-based regimens are currently the first line of CT for node-positive breast cancers; however, whether taxanes induce lymphedema remains inconclusive; and (3) RT can cause fibrosis in the treated area and impair collateral lymphatic pathways, leading to varying degrees of lymphedema.
We report here a retrospective longitudinal cohort study that demonstrates risk factors associated with PLE development. Specifically, we focused on three crucial aspects: (1) tumor factors, including the stage of cancer, tumor stage, lymph node (N) stage, presence of supraclavicular (SC) or internal mammary (IM) node metastasis (diagnosed by positron emission tomography–computed tomography or magnetic resonance imaging, or confirmed via pathology), and locally advanced breast cancer; (2) treatment factors, such as the type of surgery, CT with paclitaxel, docetaxel, or other regimens, and RT to different locations; and (3) patient factors, namely age, changes in body weight and BMI, the circumferential difference (CD) of both arms during serial follow-ups, the severity of swelling, and comorbidities.
Materials and methods
Recruitment of patients
All patients with BCRL recruited in this study were diagnosed, treated, and followed up at Koo Foundation Sun Yat-Sen Cancer Center, Taiwan. The follow-up protocols were developed by the breast cancer treatment team: all patients with breast cancer visited the oncologist every 3 months in the first 2 years after surgery, every 6 months in the third to fifth years, and once per year after that. Patients were routinely asked whether they noticed arm swelling, indentations, heaviness, or firm skin by a case manager; they were also examined by an oncologist for arm swelling and skin texture during each follow-up. In the follow-up clinic, patients with either subjective or objective arm swelling were referred to a physiatrist experienced in lymphedema diagnosis and management. Patients could also visit the physiatrist directly any time during the follow-up period if they noticed arm swelling.
The initial screening of the database between January 1, 2005, and December 31, 2015, identified 488 patients with BCRL. The inclusion criteria were as follows: (1) patients who exhibited CD in both arms of > 1 cm as measured by the physiatrist and (2) CD in both arms of < 1 cm, but manifesting as pitting edema or subcutaneous tissue hardening, or having symptoms of arm swelling, heaviness, or tight clothes. Among these patients, 146 were excluded from the study. The exclusion criteria were as follows: (1) stage IV cancer (n = 53), (2) having chest wall or axillary local recurrence (n = 37), (3) bilateral breast cancer (n = 34), (4) incomplete lymphedema treatment or being lost to follow-up (n = 7), (5) having cellulitis-induced swelling (n = 7), (6) having swelling before breast cancer surgery (n = 3), (7) having considerable heart or renal diseases (n = 3), or (8) having edema caused by deep vein thrombosis (n = 2). The resulting study population was 342 patients with breast cancer with unilateral arm swelling. This study was approved by internal review board of the hospital (IRB: 20170418A).
Diagnosis and measurements of lymphedema
The texture of skin and subcutaneous tissue of the whole arm was palpated, and circumferential measurement of both arms was performed. The physiatrist measured the circumference of the bilateral upper limbs at the metacarpophalangeal joint, the wrist, 10 cm distal to the antecubital fossa of the elbow, the elbow, and 10 and 20 cm proximal to the elbow [18]. Patients exhibiting CDs between both arms ≥ 1 cm, or those showing CD < 1 cm but with evident pitting edema or subcutaneous tissue hardening were defined as having lymphedema. The degrees of lymphedema were classified as mild, moderate, or severe if the CDs of any measured site were ≦ 2 (n = 190), 2.1–3 (n = 88), or > 3 cm (n = 64), respectively [7]. Patients with BCRL were treated and followed up in surveillance clinics.
Definition of transient and persistent lymphedema
Transient lymphedema was defined as cases that fulfill all three of the following conditions: (1) decreasing CD of both arms after the onset of arm swelling, (2) no subcutaneous tissue fibrosis or pitting edema, and (3) no subjective symptoms of arm swelling. Persistent lymphedema was defined through the following symptoms: (1) having increasing CD or maintaining the same CD between both arms and (2) having any one of the following conditions: texture hardening of the subcutaneous tissue, subjective feeling of arm swelling or discomfort even after edema treatment, and experiencing flare-up of swelling during follow-ups [19, 20].
Lymphedema treatment
Complete decongestive therapy (CDT) [6, 19,20,21] was the standard treatment for all patients with BCRL. For those who could not tolerate short-stretch bandages, pressure garments were applied. For patients with a lymphedema flare-up, another course of CDT was performed depending on the severity.
Breast cancer treatment
Surgery involved modified radical mastectomy (MRM, i.e., simple mastectomy + ALND), simple mastectomy (SM) with SLNB, and breast-conserving surgery (wide excision of the tumor) with either ALND or SLNB.
Adjuvant CT was suggested for patients who were node-positive or high-risk node-negative. A dose-dense paclitaxel-containing regimen was prescribed for N3 patients. A regimen containing docetaxel was administrated to N1 and N2 patients and high-risk N0 patients. Patients who were node-negative with moderate risk received nontaxane regimens. For patients with locally advanced tumors, neoadjuvant CT with a docetaxel-based regimen was prescribed before surgery, followed by another two courses after surgery if complete remission was achieved. If residual cancer cells persisted, CT regimens were prescribed following the criteria for adjuvant CT.
RT was delivered using computed-tomography-based treatment to all patients receiving breast-conserving surgeries, as well as patients who underwent mastectomy and were axillary-node-positive. The principle RT was administered at a dose of 45–50 Gy in 23–25 fractions to the breast or chest wall with tangential fields and a median 10-Gy boost to the tumor bed. SC and IM node RT were administered to patients with positive axillary lymph nodes [22]. Axillary node RT was delivered to some of the pN3 patients according to the judgment of the radiation oncologist.
Statistical analysis
All statistical analyses were performed using SPSS software version 24 (SPSS for Windows, SPSS Inc., Chicago, IL, USA). Descriptive statistics were expressed as mean ± standard deviation for continuous variables and number of patients (%) for categorical variables. The between-group comparisons were conducted using the Mann–Whitney U and Fisher’s exact tests. Univariate logistic regression was used to assess the potential risk factors of PLE, ignoring the effects of other factors. For the risk factors with p < 0.05 denoting statistical significance in the univariate analysis, multiple logistic regression was used to identify those that were significantly associated with PLE after adjusting for the effects of other factors in the model. Multiple logistic regression analyses with variable selection in a stepwise fashion were used to develop the multivariate models for predicting PLE. When constructing the most parsimonious model to explain the data, we sought one with optimal prediction accuracy that minimized the number of variables. We based our model choice not only on likelihood ratio and Akaike information criterion but also on the basis of clinical availability, statistical significance, and prediction accuracy. The preliminary prediction model was based on the final results of the multiple logistic regression. The area under the receiver operating characteristic (ROC) curve (AUC) was the index of prediction accuracy. Comparisons of prediction accuracy or the equivalent AUCs were assessed using STATA/SE V 13.0 (Stata Corporation, College Station, TX). All statistical tests were two-tailed, and a p value of < 0.05 was considered statistically significant.
Results
This study involved 342 patients with breast cancer with unilateral arm swelling and a mean age of 52.31 ± 11.25 years. Among them, 229 (67%) were patients with PLE. The comparison of demographics and disease, treatment, and swelling characteristics between PLE and transient lymphedema (TLE) are presented in Tables 1, 2, and 3, respectively. As shown in Table 1, the average age at surgery or onset of swelling was significantly higher for patients with PLE than those with TLE (p = 0.017 and p = 0.011, respectively). The risk of PLE for patients with breast cancer (after the onset of swelling) significantly increased with respect to the severity of the AJCC (American Joint Commission on Cancer) cancer stage (p = 0.001). A similar phenomenon was observed for the AJCC node stage (p = 0.004), but not the AJCC tumor stage (p = 0.169). As shown in Table 2, patients treated with MRM had the highest risk of PLE among the four types of surgery. The average number of lymph node metastases was significantly higher for patients with PLE than for those with TLE (p < 0.001). The risks of PLE were significantly associated with RT (p = 0.004) and RT to regional lymph nodes (SC-RT, IM-RT, and axillary-RT; p = 0.002, p < 0.001, and p = 0.002, respectively). The results in Table 3 indicate that, among the various swelling characteristics, significant differences existed between the two types of lymphedema in the following variables: weight changes from presurgery to onset of swelling (p = 0.012), the maximal CD of both arms (p < 0.001), the initial severity of lymphedema (p < 0.001), the onset time of swelling associated with CT and RT (p = 0.008 and 0.005, respectively), and cellulitis after swelling (p < 0.001).
One of the aims of this study was to establish a predictive model. The results of the univariate logistic regression shown in Table 4 reveal that (1) higher age at the onset of swelling significantly increased the risk of PLE, and the odds of PLE increased 2.3% per year of age at the onset of swelling (p = 0.034). (2) The odds ratio (OR) of PLE significantly increased with respect to the AJCC cancer stage (OR = 3.247, 3.189, and 5.429 for stages 2B, 3A, and 3B or 3C, respectively, versus stages 0 or 1; p = 0.005, p = 0.009, and p < 0.001, respectively), with a similar phenomenon observed for the AJCC node stage. (3) The odds of PLE increased by 8% for each one-unit increase in the number of lymph node metastases (p = 0.001). (4) The OR of PLE for RT (yes vs. no) was 2.834 with a 95% confidence interval of 1.451–5.536. (5) The ORs of PLE for SC-RT, IM-RT, and axillary-RT (yes vs. no) were 2.601, 2.651, and 6.773, respectively (p = 0.001, p < 0.001, and p = 0.010, respectively). (6) The odds of PLE increased by 5.8% for each 1-kg increase in weight from presurgery to the onset of swelling (p = 0.038). (7) The ORs of PLE for the maximal CDs of both arms at the onset of swelling, the highest CDs during follow-up, and the CDs at the latest follow-up were 1.699, 3.559, and 5.042, respectively (all p < 0.001). (8) The ORs of PLE for the initial severity of lymphedema (moderate and severe vs. mild) were 1.982 and 5.202, respectively (p = 0.015 and p < 0.001, respectively).
Multiple logistic regression revealed that five risk factors were significantly associated with PLE after mutually adjusting for the effects of other factors in the model (Tables 5 and 6). To demonstrate the accuracy of the prediction model using those five predictors’ multiple logistic regressions, the predicted value of this model was used as the test variable, with the corresponding ROC curve illustrated in Fig. 1. The corresponding AUC was 0.920. To establish a parsimonious model, we attempted to reduce the number of predictors in the model without sacrificing accuracy. The final prediction model is presented in Table 6, and the corresponding ROC curve is shown in Fig. 1. Its corresponding AUC was 0.908. The results of chi-square testing (with one degree of freedom) indicated no significant difference between the two AUC values (χ2 = 2.54, p = 0.1113).

ROC curves based on the multiple logistic regression prediction models
Discussion
Lymphedema is considered a progressive disease without curative treatment; however, through proper intervention, stage I lymphedema can be reversed [19, 20]. It is unclear if and how patients with stage I lymphedema progress to more severe, chronic, or persistent conditions. Our data indicated that most patients with BCRL (78.9%) started to experience swelling within 3 years after surgery. One third of patients with BCRL did not progress further, or even resolve without any flare-up, whereas two thirds of patients with BCRL were diagnosed with PLE during follow-up [6]. The goal of this study was to identify underlying risk factors of PLE that may lead to more effective prevention and treatment strategies.
We revealed that the number of metastatic lymph nodes and body weight changes from presurgery to the onset of swelling, the maximal CD of both arms at the onset of swelling, and the largest CD during follow-up were strongly associated with PLE development. This study employed a cohort of 342 patients with BCRL and comprehensive records regarding the patients, treatments, and swelling characteristics, as well as potential confounding factors such as bilateral breast cancer, local recurrence, stage IV disease, and swelling after infection. The median 7- and 5-year follow-ups after surgery and after the onset of swelling, respectively, were longer than those in most related studies. The diagnosis of BCRL was reliably performed through patients’ perceptions of arm swelling, observations by case managers and oncologists, and examination and repeated measurements by physiatrists.
Our result revealed that axillary lymph node metastasis and advanced cancer stages were related to the development of PLE. The increment of one instance of lymph node metastasis increased the risk of PLE by 8%. Lymphatic function could be impaired by tumor growth and further damaged by the surgical removal of the lymph nodes. Abnormal accumulation of water and proteins in the subcutaneous tissue, subsequent tissue proliferation, and fibrosis development gradually result in PLE [19, 20, 23].
Progression of mild arm lymphedema has been shown to be associated with morbid obesity [7], defined as a BMI of 35 kg/m2 or greater. McLaughlin et al. reported that lymphedema was associated with greater body weight, higher BMI, and infection or injury in the ipsilateral arm after surgery [12]. Our results indicated that obesity could not only be a contributor to the initial lymphatic overload responsible for the onset of lymphedema [17] but also contribute to the pathophysiologic changes responsible for its progression [7, 24]. Notably, change of body weight measured before surgery and at the onset of swelling was even more significantly related to PLE [25]. This finding is consistent with the theory of lymphatic overload [7, 17, 26].
We utilized the number of metastatic lymph nodes, the CD at the first visit, and the largest CD during follow-up to construct a prediction model for PLE. The accuracy of this predictor is denoted by an AUC of 0.908. The purpose of this prediction model was to not only explore the potential risk factors of PLE but also to provide a corresponding reference index of the accuracy of the prediction. In contrast to related studies [6,7,8,9, 12, 14, 15, 27, 28], investigating the risk factors for BCRL, AJCC cancer stage, node stage, ALND, and RT were not identified as risk factors of PLE in the final prediction model; however, they were significantly associated with PLE in the univariate logistic regression model.
Although not identified as a significant risk factor for PLE, RT is considered a major factor leading to BCRL [9, 14]. Regional lymph node irradiation (e.g., SC-RT and axillary-RT) has been found to increase the risk of BCRL by 2–5 times [6, 7, 9, 14, 29]. However, little attention has been given to IM-RT. SC-RT and IM-RT were associated with improved overall survival and are recommended for patients who are node-positive or high-risk node-negative patients [22]. Using univariate logistic regression analysis, we revealed that women receiving IM-RT or SC-RT had a 2.6-fold higher risk of developing PLE.
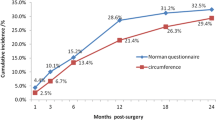
The role of CT in BCRL remains controversial. Studies have indicated that CT—especially with taxanes—is a risk factor for the development of lymphedema [6, 8, 16]. However, only limited analyses for types of taxane (e.g., docetaxel and paclitaxel) are available. A large prospective cohort study by Swaroop et al. [30] concluded that neither docetaxel or paclitaxel increased the risk of lymphedema. In this report, the cumulative incidence of lymphedema over 2 years was only 5.27%, which was much lower than in other studies [4, 6, 7]. Our data showed that patients treated with taxane-based CT were more prone to develop PLE, and patients who did not receive CT or underwent CT without taxane tended to exhibit TLE. In addition, patients receiving paclitaxel were at a higher risk of developing PLE than those who underwent treatment with docetaxel or other types of taxane. The mechanisms for such differences remain unclear [31, 32].
The limitations of this study were as follows: (1) we did not measure the circumference of both arms before surgery; a preexisting difference, though usually small [33], between dominant and nondominant arms might mask the effects of CD reported here [12]. (2) Patients without lymphedema were not included in this study, so the patients investigated were generally in more advanced stages and received more adjuvant therapies after surgery than in other reports. Most reports in the literature have described risk factors associated with the development of lymphedema in breast cancer survivors [9, 11, 12, 14,15,16,17, 28,29,30,31]. In the present study, we focused on the risk of developing persistent lymphedema in patients with already established arm edema. The topic of this investigation reflected the primary concern of the breast cancer survivors, that is, “whether the complication would go away.”The strength of our study was that we used a large sample size combined with a median 5-year follow-up.
In conclusion, we demonstrated a prediction model for PLE using three risk factors: more lymph node metastases, more weight gain from surgery to the onset of swelling, and larger CD between arms. On the basis of these results, we encourage the early diagnosis of breast cancers, appropriate body weight control for postoperative patients, and early education on manual lymph drainage for high-risk patients [8, 34].
References
Ahmed RL, Prizment A, Lazovich D, Schmitz KH, Folsom AR (2008) Lymphedema and quality of life in breast Cancer survivors: the Iowa Women’s Health Study. J Clin Oncol 26(35):5689–5696
Velanovich V, Szymanski W (1999) Quality of life of breast cancer patients with lymphedema. Am J Surg 177(3):184–188
Kilbreath SL, Lee M-J, Refshauge KM, Beith JM, Ward LC, Simpson J, Black D (2013) Transient swelling versus lymphoedema in the first year following surgery for breast cancer. Support Care Cancer 21(8):2207–2215
Norman SA, Localio AR, Potashnik SL, Simoes Torpey HA, Kallan MJ, Weber AL, Miller LT, DeMichele A, Solin LJ (2009) Lymphedema in breast cancer survivors: incidence, degree, time course, treatment, and symptoms. J Clin Oncol 27(3):390–397
Hayes SC, Johansson K, Stout NL, Prosnitz R, Armer JM, Gabram S, Schmitz KH (2012) Upper-body morbidity after breast cancer. Cancer 118(S8):2237–2249
Kim M, Shin KH, Jung S-Y, Lee S, Kang H-S, Lee ES, Chung SH, Kim Y-J, Kim TH, Cho KH (2016) Identification of prognostic risk factors for transient and persistent lymphedema after multimodal treatment for breast cancer. Cancer Res Treat 48(4):1330–1337
Ad VB, Cheville A, Solin LJ, Dutta P, Both S, Harris EE (2010) Time course of mild arm lymphedema after breast conservation treatment for early-stage breast cancer. Int J Radiat Oncol Biol Phys 76(1):85–90
Shah C, Arthur DW, Wazer D, Khan A, Ridner S, Vicini F (2016) The impact of early detection and intervention of breast cancer- related lymphedema: a systematic review. Cancer Med 5(6):1154–1162
Pereira ACPR, Koifman RJ, Anke Bergmann A (2017) Incidence and risk factors of lymphedema after breast cancer treatment: 10 years of follow-up. Breast 36:67–73
Soyder A, Taştaban E, Özbaş S, Boylu S, Özgün H (2014) Frequency of early-stage lymphedema and risk factors in postoperative patients with breast Cancer. J Breast Health 10(2):92–97
DiSipio T, Rye S, Newman B, Hayes S (2013) Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol 14(6):500–515
McLaughlin SA, Wright MJ, Morris KT, Giron GL, Sampson MR, Brockway JP, Hurley KE, Riedel ER, Van Zee KJ (2008) Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurements. J Clin Oncol 26(32):5213–5219
Czerniec S, Ward L, Refshauge K, Beith J, Lee M, York S, Kilbreath S (2010) Assessment of breast cancer-related arm lymphedema—comparison of physical measurement methods and self-report. Cancer Investig 28(1):54–62
Shaitelman SF, Chiang YJ, Griffin KD, DeSnyder SM, Smith BD, Schaverien MV, Woodward WA, Cormier JN (2017) Radiation therapy targets and the risk of breast cancer-related lymphedema: a systematic review and network meta-analysis. Breast Cancer Res Treat 162(2):201–215
Kilbreath S, Refshauge K, Beith J, Ward L, Ung O, Dylke E, French J, Yee J, Koelmeyer L, Gaitatzis K (2016) Risk factors for lymphoedema in women with breast cancer: a large prospective cohort. Breast 28:29–36
Cariati M, Bains SK, Grootendorst MR, Suyo A, Peters AM, Mortimer P, Ellis P, Harries M, Van Hemelrijck M, Purushotham AD (2015) Adjuvant taxanes and the development of breast cancer-related arm lymphoedema. Br J Surg 102(9):1071–1078
Soran A, D'Angelo G, Begovic M, Ardic F, Harlak A, Samuel Wieand H, Vogel VG, Johnson RR (2006) Breast cancer-related lymphedema—what are the significant predictors and how they affect the severity of lymphedema? Breast Journal 12(6):536–543
Yoo J-N, Cheong Y-S, Min Y-S, Lee S-W, Park HY, Jung T-D (2015) Validity of quantitative lymphoscintigraphy as a lymphedema assessment tool for patients with breast cancer. Ann Rehabil Med 39(6):931–940
Földi M, Földi E, Strößenreuther R, Kubik S (2012) Földi's textbook of lymphology: for physicians and lymphedema therapists. Elsevier Health Sciences
Joachim EZ, Norton S (2009) Lymphedema management: the comprehensive guide for practitioners
Lasinski BB, Thrift K, Squire D, Austin MK, Smith KM, Wanchai A, Green JM, Stewart BR, Cormier JN, Armer JM (2012) A systematic review of the evidence for complete decongestive therapy in the treatment of lymphedema from 2004 to 2011. Phys Med Rehabil 4:580–601
Poortmans PM, Collette S, Kirkove C, Van Limbergen E, Budach V, Struikmans H, Collette L, Fourquet A, Maingon P, Valli M (2015) Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med 373(4):317–327
Casley-Smith JR (1995) Alterations of untreated lymphedema and it's grades over time. Lymphology 28(4):174–185
Mehrara BJ, Greene AK (2014) Lymphedema and obesity: is there a link? Plast Reconstr Surg 134(1):154–160
Petrek JA, Senie RT, Peters M, Rosen PP (2001) Lymphedema in a cohort of breast carcinoma survivors 20 years after diagnosis. Cancer 92:1368–1377
Eyigör S, Cinar E, Caramat I, Unlu BK (2015) Factors influencing response to lymphedema treatment in patients with breast cancer-related lymphedema. Support Care Cancer 23(9):2705–2710
Vieira RA, da Costa AM, de Souza JL, Coelho RR, de Oliveira CZ, Sarri AJ, Junior RJ, Zucca-Matthes G (2016) Risk factors for arm lymphedema in a cohort of breast cancer patients followed up for 10 years. Breast Care (Basel) 11(1):45–50
Shah C, Wilkinson JB, Baschnagel A, Ghilezan M, Riutta J, Dekhne N, Balaraman S, Mitchell C, Wallace M, Vicini F (2012) Factors associated with the development of breast cancer-related lymphedema after whole-breast irradiation. Int J Radiat Oncol Biol Phys 83(4):1095–1100
Kim M, Kim SW, Lee SU, Lee NK, Jung S-Y, Kim TH, Lee ES, Kang H-S, Shin KH (2013) A model to estimate the risk of breast cancer-related lymphedema: combinations of treatment-related factors of the number of dissected axillary nodes, adjuvant chemotherapy, and radiation therapy. Int J Radiat Oncol Biol Phys 86(3):498–503
Swaroop MN, Ferguson CM, Horick NK, Skolny MN, Miller CL, Jammallo LS, Brunelle CL, O’Toole JA, Isakoff SJ, Specht MC (2015) Impact of adjuvant taxane-based chemotherapy on development of breast cancer-related lymphedema: results from a large prospective cohort. Breast Cancer Res Treat 151(2):393–403
Brønstad A, Berg A, Reed RK (2004) Effects of the taxanes paclitaxel and docetaxel on edema formation and interstitial fluid pressure. Am J Phys Heart Circ Phys 287(2):H963–H968
Behar A, Pujade-Lauraine E, Maurel A, Brun M, Lagrue G, Feuilhade De Chauvin F, Oulid-Aissa D, Hille D (1997) The pathophysiological mechanism of fluid retention in advanced cancer patients treated with docetaxel, but not receiving corticosteroid comedication. Br J Clin Pharmacol 43(6):653–658
Kissin M, Della Rovere GQ, Easton D, Westbury G (1986) Risk of lymphoedema following the treatment of breast cancer. Br J Surg 73(7):580–584
Lacomba MT, Sánchez MJY, Goñi AZ, Merino DP, del Moral OM, Téllez EC, Mogollón EM (2010) Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. Br Med J 340:b5396
Acknowledgments
The author wishes to acknowledge the Koo-Foundation Sun Yat-Sen Cancer Center.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Penn, IW., Chang, YC., Chuang, E. et al. Risk factors and prediction model for persistent breast-cancer-related lymphedema: a 5-year cohort study. Support Care Cancer 27, 991–1000 (2019). https://doi.org/10.1007/s00520-018-4388-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-018-4388-6