
Summary
Background
In a retrospective analysis of a prospective single center registry we compared the use of bivalirudin, unfractionated heparin (UFH) monotherapy, UFH + abciximab in 1240 consecutive patients with acute coronary syndrome (ACS) undergoing stent implantation.
Results
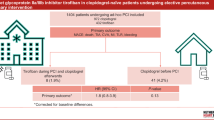
Bivalirudin was associated with tendentially reduced in-hospital minor or major bleeding rates compared to UFH monotherapy (5.9 % vs. 9.4 % adjusted odds ratio (OR) 0.82, 95 % confidence interval CI 0.45–1.51, p = 0.53) and compared to the pooled UFH group (5.9 % vs. 11.9 %, adjusted OR 0.62, 95 % CI 0.36–1.08, p = 0.09) but with significantly lower bleeding hazards compared to UFH + abciximab (5.9 % vs. 16 %, adjusted OR 0.41, 95 % CI 0.22–0.78, p < 0.01). After 3 years of follow-up, adjusted cardiovascular mortality rates were similar between all groups, particularly between bivalirudin vs. UFH monotherapy (hazard ratio HR 1.12, 95 % CI 0.58–2.16, p = 0.73) and vs. UFH + abciximab (HR 0.91, 95 % CI 0.40–2.10, p = 0.83). Acute or subacute stent thrombosis occurred at a rate of 0.8 % with no significant differences between the groups.
Conclusions
This retrospective analysis in a real world situation of medium to high-risk ACS patients undergoing invasive revascularization confirmed the results of most large-scale randomized trials by demonstrating reduced bleeding rates in favor of bivalirudin vs. UFH + GPI but with no significant differences between treatment strategies for long-term all-cause and cardiovascular mortality.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Invasive revascularization with stent implantation is the standard of care for the majority of patients presenting with acute coronary syndrome (ACS) and improves clinical outcomes compared to a more conservative approach [1]. Recent studies have suggested that novel antithrombotic and antiplatelet strategies, namely fondaparinux [2], bivalirudin [3, 4], ticagrelor [5] and rivaroxaban in combination with dual antiplatelet therapy [6] may reduce mortality in ACS patients. In recent large-scale prospective randomized trials, the favorable pharmacological action of bivalirudin translated into lower 30-day major bleeding rates compared to unfractionated heparin (UFH) plus a glycoprotein IIb/IIIa inhibitor (GPI) and also vs. UFH monotherapy but exhibited similar or even worse rates in ischemic events depending on study design, patient selection and concomitant therapy [4, 7–9]. While previous guidelines have led to an increased use of bivalirudin in the USA, bivalirudin is infrequently used in ACS patients undergoing percutaneous coronary interventions (PCI) in western Europe (approximately 10 % of patients) with the exception of some highly specialized centers. Of note, international trials have mainly compared bivalirudin (monotherapy) with UFH + GPI in ACS patients and real world observations vs. UFH monotherapy are scarce [3, 9–11]. Accordingly, we investigated the efficacy and safety of bivalirudin compared to heparin-based strategies in patients with ST-elevation or non-ST-elevation myocardial infarction (STEMI and NSTEMI, respectively) referred for acute angiography who subsequently received PCI and stent implantation.
Patients and methods
Study population
In this post hoc analysis of a prospective registry, antithrombotic therapy (as used per the discretion of the interventional cardiologist), cardiovascular risk factors, comorbidities and coronary morphology were evaluated in 1240 consecutive patients with ACS who were referred for PCI with stent implantation between January 2004 and June 2012. We included STEMI patients presenting with ST-segment elevation of 1 mm or more in two or more contiguous leads, as well as NSTEMI patients with elevated troponin I, troponin T or creatine kinase MB levels (CK-MB) above the upper limit of normal and/or ST-segment depression of ≥1 mm. Patients lacking laboratory or electrocardiographic evidence suggestive of high-risk ACS were excluded from this analysis as were patients referred for rescue PCI after thrombolytic therapy, patient records with a missing cause of death (n = 4) or patients who were in cardiogenic shock at any time during index hospitalization. In contrast to current practice, PCI was performed by the femoral approach in the vast majority of patients included into the registry (93 %). The study was performed in accordance with the Declaration of Helsinki and approved by the local ethics committee (EK 10-046-VK_NZ).
Study treatment
As the institutional standard of care, all patients received aspirin and clopidogrel as a 600 mg loading dose (LD) followed by 75 mg maintenance dose (MD), prasugrel (60 mg LD followed by 10 mg MD except in patients >75 years or <60 kg who received 5 mg MD) or ticagrelor (180 mg LD followed by 180 mg MD). Prasugrel was used in most STEMI patients and in high-risk NSTEMI patients starting in 2010. All STEMI patients were pretreated with UFH (60 IU/kg i.v. bolus but maximum 5000 U) by emergency physicians. All NSTEMI patients received anticoagulation with enoxaparin, UFH or fondaparinux until diagnostic coronary angiography. In the case of fondaparinux being given prior to catheterization, UFH was exclusively added in the catheterization laboratory as i.v. bolus of 85 IU/kg body weight. The NSTEMI patients who were pretreated with enoxaparin or UFH and STEMI patients either received UFH in the catheterization laboratory or bivalirudin, which was administered as bolus and infusion only until the end of the intervention due to practical reasons (both STEMI and NSTEMI: 0.75 mg/kg bolus, 1.75 mg/kg/h infusion). If extended bed rest after PCI was indicated, enoxaparin was administered at a thrombosis prophylactic dose until full mobilization. Abciximab was used in the presence of increased thrombus load in the infarct-related artery or as bail-out therapy in patients with slow or no-reflow in the recommended dosage (bolus +infusion for 12 h). Moreover, patients received optimal secondary prevention, i. e. statin therapy with a target low-density lipoprotein (LDL) of less than 70 mg/dl (1.8 mmol/l) but also other guideline-recommended treatment, such as beta blockers, angiotensin converting enzyme (ACE) inhibitors and/or angiotensin receptor blockers. All ACS patients received parenteral anticoagulation, aspirin and an approved P2Y12 inhibitor, as early as possible, usually in the emergency room of the department but in the majority before the catheter laboratory. Decisions regarding the choice of P2Y12 inhibitor, bail-out use of abciximab, access site, performance of thrombus aspiration, stent type and duration of dual antiplatelet therapy were left to the physician’s discretion.
Study outcome
The primary efficacy endpoint was cardiovascular mortality after 3 years of follow-up. As secondary efficacy endpoints we evaluated all-cause mortality after 3 years of follow-up as well as acute and subacute stent thrombosis. Mortality data for all patients were obtained from Statistics Austria, an independent and non-profit-making federal institution under public law that supports scientific services. Cases of death occurring in Austria are centrally recorded by Statistics Austria and data are made available for authorized institutions on request. Cause of death is reported by means of the International Statistical Classification of Disease and Related Health Problems (ICD-10). A cardiovascular death was adjudicated when an ICD-10 chapter I00-I99 diagnosis was reported as the cause of death. Acute and subacute stent thrombosis was evaluated and reported according to the definition proposed by the Academic Research Consortium [12]. The primary safety endpoint was a composite of in-hospital minor or major bleeding events based on the Thrombolysis in Myocardial Infarction (TIMI) classification. As tertiary endpoint we registered days from PCI to hospital discharge. This tertiary endpoint was compared between patients with and without bleeding complications and between the different antithrombotic strategies. For the detection of in-hospital bleeding, levels of hemoglobin and hematocrit were measured before and daily after PCI until hospital discharge. For categorization of periprocedural bleeding events, we calculated the difference in hemoglobin concentrations between the most recent hemoglobin value before PCI and the hemoglobin nadir post-PCI. In accordance with the TIMI bleeding classification [13] the following cut-off levels were used: minor bleeding was defined as a drop in hemoglobin from ≥3 to <5 g/dl or a ≥10 % decrease in hematocrit and major bleeding was defined as a drop in hemoglobin ≥5 g/dl or a ≥15 % decrease in hematocrit.
Clinical outcome data were compared between the pooled bivalirudin group (with or without GPI use) vs. UFH monotherapy, vs. UFH + abciximab and vs. the pooled UFH group. As the group of patients receiving bivalirudin + abciximab represented only 1.1 % of the whole cohort (14 patients), a separate analysis for this subgroup was not performed.
Statistical methods
Descriptive statistics were performed on baseline variables and stratified by the different treatment groups. Discrete characteristics are expressed as frequency counts and percentages and differences were determined by the χ2-test. Continuous characteristics are expressed as means and standard deviations or medians (where appropriate), with differences examined with the Kruskal-Wallis test throughout all groups or the Mann-Whitney test for the comparison of two treatment arms. The level of significance used for all tests was a two-sided p-value of 0.05.
Univariate analysis in the Cox proportional hazards and the logistic regression model was performed to estimate mortality and bleeding hazards between different antithrombotic treatments. A 1:1 matched propensity score for the abovementioned two-group comparisons was obtained in order to account for confounding variables. Covariates were chosen based on significant differences between groups (Table 1) and well-established risk factors, e.g. age, gender, body mass index (BMI), estimated glomerular filtration rate (eGFR), baseline hemoglobin, hypertension, hyperlipidemia, smoking, diabetes, clinical presentation (STEMI or NSTEMI), type of stent, number of diseased vessels, previous MI, previous invasive revascularization, peripheral artery disease, prior stroke or transient ischemic attack (TIA), heart failure, history of malignancies, atrial fibrillation, vascular access site, year of index hospitalization, statin treatment and antiplatelet substance. The corresponding propensity scores were then included in the Cox regression (mortality) and logistic regression (in-hospital bleeding) analyses for the two-group comparisons.
Likewise, the impact of bleeding and antithrombotic therapy on the duration of hospitalization was analyzed in a linear regression model. The Software Package for Social Sciences version 22 (SPSS, Chicago, IL) was used for all statistical calculations.
Results
Study population
Registered baseline characteristics included cardiovascular risk factors, comorbidities, coronary morphology, medication at hospital discharge and laboratory findings (Table 1). From 1240 patients presenting with ACS and undergoing PCI plus stent implantation, 632 (51.4 %) patients presented with STEMI. Of the total cohort, 273 (22 %) received bivalirudin monotherapy in the catheterization laboratory, 14 (1.1 %) received bivalirudin + abciximab, 596 (48.1 %) received UFH alone and 357 (28.8 %) patients received UFH + abciximab. The NSTEMI patients more frequently received bivalirudin, while STEMI patients more frequently received UFH + abciximab (p < 0.01, Table 1). The utilization of the different antithrombotic strategies over time is presented in Fig. 3. There was a steep increase in bivalirudin use, starting from 2009 (p for trend <0.01).
Similarities as well as significant differences regarding baseline characteristics were detected between the study groups. While patients receiving UFH monotherapy, as compared to the pooled bivalirudin group were similar with respect to age, diabetes, hypertension, previous stroke, myocardial infarction or PCI, heart failure, coronary morphology and other characteristics (Table 1), these patients had lower levels of hemoglobin at admission (median 14.1 g/dl vs. 13.8 g/dl, p < 0.01) and lower levels of estimated glomerular filtration rate (eGFR, median 91.6 ml/min vs. 82.7 ml/min, p = 0.01). Patients receiving UFH + abciximab were younger (median age 63 years vs. 59 years, p < 0.01), had higher levels of baseline hemoglobin (median 14.1 mg/dl vs. 14.5 mg/dl, p < 0.01) and had a higher eGFR than patients of the pooled bivalirudin cohort (median eGFR 91.6 ml/min vs. 96.5 ml/min, p < 0.01). Risk factors and comorbidities, such as diabetes, hypertension, prior stroke, TIA or a history for malignant tumors were more prevalent in the pooled bivalirudin group, as opposed to UFH + abciximab. Discharge medications including ACE inhibitors, ARBs and beta blockers were similar between groups, while patients treated with UFH monotherapy received adequate statin therapy at hospital discharge less frequently than patients treated with bivalirudin or with UFH + abciximab (Table 1, p < 0.001). Moreover, bivalirudin treated patients received one of the novel P2Y12-receptor inhibitors twice as frequently compared to UFH-treated patients. In total, 88.9 % of patients with drug-eluting stent (DES) implantation received dual antiplatelet therapy for 12 months, while 8.7 % were treated for 6–9 months only. Therapy durations that were either shorter or longer were observed in 2.4 % of patients.
Mortality outcome
Patients were followed for up to 3 years after the index hospitalization. In total, 113 (9.1 %) events occurred. Rates of all-cause death were 8.7 %, 10.2 % and 7.6 % in the pooled bivalirudin, UFH monotherapy and UFH + abciximab groups, respectively. Corresponding rates of cardiovascular death were 4.9 %, 6.4 % and 4.8 % after 3 years of follow-up, respectively. Univariate analysis revealed non-significant different rates of all-cause or cardiovascular death for bivalirudin vs. UFH monotherapy, vs. UFH + abciximab and the pooled UFH group as well as for UFH monotherapy vs. UFH + abciximab (Table 2).
After adjustment for confounders, similar mortality rates were observed for all comparisons. Univariate and multivariate analyses are presented in Table 2. Kaplan-Meier survival curves are shown in Fig. 1.

Kaplan-Meier plots for all-cause death (a) and cardiovascular death (b) after 3 years, stratified for antithrombotic treatment strategy. On propensity score adjusted Cox regression modelling, there were no significant differences between groups for both endpoints (Table 2)
Stent thrombosis
Acute or subacute stent thrombosis occurred in 10 (0.8 %) patients. In the pooled bivalirudin group 1 (0.4 %) definite, subacute event occurred. In the UFH monotherapy group, three definite and two probable events occurred (0.8 %) of which two were acute and three subacute. In the UFH + abciximab group, we observed two definite and two probable stent thromboses (1.1 %) of which one event was acute. The differences between groups were not statistically significant (p = 0.748) (Table 2).
Bleeding outcome
As shown in Fig. 2 composite rates of in-hospital TIMI minor or major bleeding were 5.9 % for the pooled bivalirudin group, whereas these bleeding rates were 9.4 % for the UFH monotherapy, 16 % for the UFH + abciximab group and 11.9 % for the pooled UFH group.

Rates of in-hospital bleeding stratified by anticoagulant treatment groups. Combined minor or major bleeding events were significantly lower comparing pooled bivalirudin vs. UFH + abciximab (OR 0.41, 95 % CI 0.22–0.78, p = 0.01), whereas bleeding rates were similar between bivalirudin vs. UFH alone (OR 0.82, 95 % CI 0.45–1.51, p = 0.53)
Univariate and multivariate analyses in the logistic regression model are presented in Table 3.
After adjustment for confounding baseline variables bivalirudin use was associated with significantly lower rates in the composite endpoint of TIMI minor or major bleeding as compared to UFH + abciximab (5.9 % vs. 16 %, OR 0.41, 95 % CI 0.22–0.78, p = 0.01). Adjusted rates of bleeding were non-significantly lower for pooled bivalirudin vs. UFH monotherapy (5.9 % vs. 9.4 %, OR 0.82, 95 % CI 0.45–1.51, p = 0.53), and were reduced by 35 % comparing UFH alone to UFH + abciximab (9.4 % vs. 16 %, OR 0.65, 95 % CI 0.43–0.99, p = 0.047). Comparing the pooled bivalirudin vs. the pooled UFH group, there was a non-significant trend towards reduced bleeding rates (5.9 % vs. 11.9 %, OR 0.62, 95 % 0.36–1.08, p = 0.09). The year of treatment was accounted for in all adjusted analyses and the utilization of anticoagulants over time is presented in Fig. 3.

Utilization of the different antithrombotic strategies over time. Timely linked to the publication of the HORIZONS-AMI trial, there was a significant increase in bivalirudin utilization, whereas strategies including abciximab were less frequently used thereafter
Duration of hospitalization
Median days from PCI to hospital discharge are presented in Fig. 4. After adjustment for confounding baseline variables major and minor bleeding prolonged post-PCI hospital stay by 6.5 (95%CI 4.5–8.5, p < 0.01) and 3.2 (95 % CI 2.0–4.3, p < 0.01) days, respectively, as compared to patients without an in-hospital bleeding episode.

Median days from PCI to hospital discharge for the overall cohort and stratified by clinical presentation and bleeding severity. On adjustment for confounders, major and minor bleeding prolonged post-PCI hospital stay by 6.5 (95% CI 4.5–8.5, p < 0.01) and 3.2 (95 % CI 2.0–4.3, p < 0.01) days, respectively, compared to patients not experiencing a bleeding episode
Median days from PCI to hospital discharge were 5 (Interquartile range [IQR] 2;7), 5 (IQR 2; 7) and 7 (IQR 5; 8) in the pooled bivalirudin, UFH monotherapy and UFH + abciximab groups, respectively. After adjustment for confounders days from PCI to discharge were similar between the pooled bivalirudin and UFH monotherapy groups (−0.8, 95 % CI −1.7 to −0.06, p = 0.07) but reduced by 1.5 (95 % CI −2.2 to −0.7, p < 0.01) days compared to UFH + abciximab.
Discussion
In this retrospective analysis of a prospective registry, reflecting a real world situation, we were able to confirm the results of most randomized controlled trials in ACS patients undergoing invasive revascularization. Bivalirudin use was associated with a 59 % relative risk reduction in periprocedural combined TIMI minor or major bleeding rates compared to UFH +GPI, along with a reduced hospital stay after PCI. Bleeding rates were numerically but not statistically significantly lower comparing pooled bivalirudin vs. UFH alone or the pooled UFH group, whereas the rates of stent thrombosis, all-cause death and cardiovascular death were not statistically different between groups. Abciximab use increased significantly between 2006 and 2009 probably because of the recommendations issued by the American College of Cardiology/American Heart Association (ACC/AHA) guidelines on STEMI (2004) and NSTEMI (2007) as well as by the European Society of Cardiology (ESC) guidelines on the use of antiplatelet agents (2004) [14–16]. Moreover, timely linked to the publication of the HORIZONS-AMI trial in 2008, there was a significant increase in bivalirudin utilization, whereas strategies including abciximab were less recommended and also used thereafter [3]. This underlines the adherence to international guidelines at our center.
Mortality outcome
Several earlier randomized trials conducted in the setting of moderate to high-risk NSTEMI (ACUITY and ISAR REACT 4) and STEMI (HORIZONS-AMI) revealed a positive net clinical benefit in favor of bivalirudin vs. UFH + GPI, primarily through the reduction of major bleeding events [3, 10, 11, 17]. The more recent EUROMAX trial investigated bivalirudin (with 12 % GPI use) vs. UFH (with 69 % GPI use) in a modern treatment setting for STEMI (50 % novel P2Y12 inhibitors) and also demonstrated a positive net clinical benefit in favor of bivalirudin. This benefit was mainly achieved through the reduction of major bleeding events, whereas cardiac death was not affected by the choice of the anticoagulant [7]. As the use of GPIs is usually low in a contemporary clinical setting, while radial access and novel P2Y12 receptor inhibitors are increasingly being used, the comparison vs. UFH monotherapy is particularly desirable [18]. The BRIGHT trial randomly assigned 2194 STEMI patients to bivalirudin with a 3‑h postprocedural infusion, UFH alone or UFH + tirofiban and reported no significant differences regarding major adverse cardiac or cerebral events at 30 days [8]. The recent MATRIX trial randomized 7213 ACS patients to either bivalirudin or UFH alone (only 0.2 % GPI use) and did not show a net improvement in adverse clinical events. Although cardiac death was reduced by 32 % (likely through reduction of major bleeding), this was counterbalanced by an excess in definite stent thrombosis [4]. In the single center HEAT-PPCI trial, also conducted in a modern setting (15 % GPI bail-out use, 90 % novel P2Y12 receptor inhibitors and over 80 % radial access) major adverse cardiovascular events were significantly increased by 52 % in the bivalirudin arm, with a fourfold risk of stent thrombosis and also an increase in bleeding hazards [9]. Meta-analyses provided conflicting results depending on the selection of these trials regarding reinfarction but showed no differences in mortality despite an increase in acute stent thrombosis in bivalirudin treated patients [19, 20]. In line with these findings we did not observe a mortality difference between groups, keeping in mind that statistical power was limited due to low sample size.
Stent thrombosis
The rate of stent thrombosis was in the range of previously published data, also considering that 51 % of patients received bare metal stents [21]. We did not observe significant differences between groups; however, event rates were too low for statistical adjustment for confounders. In this setting there was no excess in acute stent thrombosis in patients treated with bivalirudin, opposed to data from previous large-scale trials [4, 7, 9].
Bleeding outcomes
Our data are similar to the findings from the HORIZONS-AMI, EUROMAX, ACUITY, ISAR-REACT 4, and REPLACE-2 trials regarding significantly reduced bleeding hazards for bivalirudin vs. UFH + GPI [3, 7, 10, 11, 22]. As expected, we also observed lower bleeding rates when UFH monotherapy was compared to UFH + abciximab. It has to be noted that from a clinical point of view, comparisons against UFH + GPI are less relevant as recent guidelines recommend to restrict GPI use to bail-out situations [18, 23].
Data from prospective, randomized trials comparing bivalirudin and UFH monotherapies with respect to bleeding rates pointed in the same direction in both stable and ACS patients: [4, 8, 24]. In the recent BRIGHT and MATRIX trials, bleeding rates were significantly lower in favor of bivalirudin vs. UFH alone even when bivalirudin was continued following the procedure [4, 8]. Interestingly, no differences in major bleeding could be observed in the HEAT-PPCI trial [9] conducted in a modern setting with respect to antiplatelet agents, access site and GPI use. A potential explanation could be the prominent use of new P2Y12 receptor inhibitors that are known to be associated with significantly higher spontaneous bleeding rates [5, 25]. This was further confirmed by a post hoc analysis of EUROMAX demonstrating similar clinical outcome but higher per protocol major bleeding rates in patients treated with prasugrel or ticagrelor as compared to clopidogrel [26]. Although in-hospital bleeding rates in ACS patients undergoing PCI might also depend on the vascular access site and the majority of femoral access in our study might have influenced bleeding rates, a recent analysis has shown benefits for bivalirudin over UFH monotherapy and over UFH +GPI for both access sites [7].
Hospital stay
The occurrence of TIMI minor and major bleeding had a substantial impact on post-PCI hospital stay in our analysis. As also described by others, major bleeding hazards accounted for an almost twofold prolongation of hospitalization in ACS patients [27]. Thus, preventing bleeding is important to preserve healthcare resource consumption, in addition to optimizing clinical outcomes.
Limitations
The data from the present study were collected from a single center and in a non-randomized fashion as the treatment strategy was at the discretion of the treating interventional cardiologist; however, the 100 % follow-up rate strengthens the quality of data collection in this registry. Moreover, the number of patients in the bivalirudin arm was relatively low. This is mainly due to the fact that the majority of patients were included before publication of the recent NSTEMI and STEMI guidelines recommending bivalirudin monotherapy over UFH and UFH + GPI [28, 29]. Potential differences between treatment groups were existent but were accounted for in propensity score-adjusted models. Finally, additional safety and efficacy endpoints such as stroke, reinfarction, stent thrombosis, repeat revascularization, transfusion and thrombocytopenia, which may vary between the study regimens, are not available. Our findings might not apply to patients treated via a radial approach.
Conclusion
This real world experience in patients presenting with ACS and undergoing PCI and stent implantation indicates that bivalirudin is clinically similar to UFH monotherapy but superior to UFH + abciximab with respect to the reduction of bleeding events, which in turn was associated with a shorter hospital stay. The rate of stent thrombosis as well as long-term clinical outcomes in terms of all-cause and cardiovascular mortality were statistically similar between groups.
References
Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T, et al. Guidelines on myocardial revascularization. Eur Heart J. 2010;31(20):2501–55.
Anderson JA, Hirsh J, Yusuf S, Johnston M, Afzal R, Mehta SR, et al. Comparison of the anticoagulant intensities of fondaparinux and enoxaparin in the Organization to Assess Strategies in Acute Ischemic Syndromes (OASIS)-5 trial. J Thromb Haemost. 2010;8(2):243–9.
Stone GW, Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med. 2008;358(21):2218–30.
Valgimigli M, Frigoli E, Leonardi S, Rothenbuhler M, Gagnor A, Calabro P, et al. Bivalirudin or unfractionated heparin in acute coronary syndromes. N Engl J Med. 2015;373(11):997–1009.
Cannon CP, Harrington RA, James S, Ardissino D, Becker RC, Emanuelsson H, et al. Comparison of ticagrelor with clopidogrel in patients with a planned invasive strategy for acute coronary syndromes (PLATO): a randomised double-blind study. Lancet. 2010;375(9711):283–93.
Mega JL, Braunwald E, Wiviott SD, Bassand JP, Bhatt DL, Bode C, et al. Rivaroxaban in patients with a recent acute coronary syndrome. N Engl J Med. 2012;366(1):9–19.
Steg PG, van’t Hof A, Hamm CW, Clemmensen P, Lapostolle F, Coste P, et al. Bivalirudin started during emergency transport for primary PCI. N Engl J Med. 2013;369(23):2207–17.
Han Y, Guo J, Zheng Y, Zang H, Su X, Wang Y, et al. Bivalirudin vs heparin with or without tirofiban during primary percutaneous coronary intervention in acute myocardial infarction: the BRIGHT randomized clinical trial. JAMA. 2015;313(13):1336–46.
Shahzad A, Kemp I, Mars C, Wilson K, Roome C, Cooper R, et al. Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI): an open-label, single centre, randomised controlled trial. Lancet. 2014;384(9957):1849–58.
Kastrati A, Neumann FJ, Schulz S, Massberg S, Byrne RA, Ferenc M, et al. Abciximab and heparin versus bivalirudin for non-ST-elevation myocardial infarction. N Engl J Med. 2011;365(21):1980–9.
Stone GW, McLaurin BT, Cox DA, Bertrand ME, Lincoff AM, Moses JW, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med. 2006;355(21):2203–16.
Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, Es GA van, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115(17):2344–51.
Bovill EG, Terrin ML, Stump DC, Berke AD, Frederick M, Collen D, et al. Hemorrhagic events during therapy with recombinant tissue-type plasminogen activator, heparin, and aspirin for acute myocardial infarction. Results of the Thrombolysis in Myocardial Infarction (TIMI), phase II trial. Ann Intern Med. 1991;115(4):256–65.
Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (writing committee to revise the 1999 guidelines for the management of patients with acute myocardial infarction). Circulation. 2004;110(5):588–636.
Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr., et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (writing committee to revise the 2002 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction): developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons: endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. Circulation. 2007;116(7):e148–e304.
Patrono C, Bachmann F, Baigent C, Bode C, De Caterina R, Charbonnier B, et al. Expert consensus document on the use of antiplatelet agents. The task force on the use of antiplatelet agents in patients with atherosclerotic cardiovascular disease of the European Society of Cardiology. Eur Heart J. 2004;25(2):166–81.
Stone GW, Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, et al. Heparin plus a glycoprotein IIb/IIIa inhibitor versus bivalirudin monotherapy and paclitaxel-eluting stents versus bare-metal stents in acute myocardial infarction (HORIZONS-AMI): final 3‑year results from a multicentre, randomised controlled trial. Lancet. 2011;377(9784):2193–204.
Capodanno D, De Caterina R. Bivalirudin for acute coronary syndromes: premises, promises and doubts. Thromb Haemost. 2015;113(4):698–707.
Capodanno D, Gargiulo G, Capranzano P, Mehran R, Tamburino C, Stone GW. Bivalirudin versus heparin with or without glycoprotein IIb/IIIa inhibitors in patients with STEMI undergoing primary PCI: an updated meta-analysis of 10,350 patients from five randomized clinical trials. Eur Heart J Acute Cardiovasc Care. 2015;5(3):253–62. doi:10.1177/2048872615572599.
Cavender MA, Sabatine MS. Bivalirudin versus heparin in patients planned for percutaneous coronary intervention: a meta-analysis of randomised controlled trials. Lancet. 2014;384(9943):599–606.
Byrne RA, Joner M, Kastrati A. Stent thrombosis and restenosis: what have we learned and where are we going? The Andreas Gruntzig Lecture ESC 2014. Eur Heart J. 2015;36(47):3320–31.
Lincoff AM, Bittl JA, Harrington RA, Feit F, Kleiman NS, Jackman JD, et al. Bivalirudin and provisional glycoprotein IIb/IIIa blockade compared with heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary intervention: REPLACE-2 randomized trial. JAMA. 2003;289(7):853–63.
Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541–619.
Kastrati A, Neumann FJ, Mehilli J, Byrne RA, Iijima R, Buttner HJ, et al. Bivalirudin versus unfractionated heparin during percutaneous coronary intervention. N Engl J Med. 2008;359(7):688–96.
Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357(20):2001–15.
Huber K, Hamm C, Van’t Hof A, Lapostolle F, Coste P, Thicoipe M, et al. Impact of P2Y12 inhibitor choice on 30-day outcomes after primary PCI: an analysis from the EUROMAX trial. J Am Coll Cardiol. 2014;63(12):A100. doi:10.1016/s0735-1097(14)60100-5.
Happe LE, Rao SV, Horblyuk R, Franklin M, Lunacsek OE, Menditto L. Consequences of major bleeding in hospitalized patients with non-ST segment elevation acute coronary syndromes receiving injectable anticoagulants. Curr Med Res Opin. 2009;25(2):413–20.
Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011;32(23):2999–3054.
Steg PG, James SK, Atar D, Badano LP, Lundqvist CB, Borger MA, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Eur Heart J. 2012;33(20):2569–619.
Open access funding provided by Medical University of Vienna.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. Rohla, I. Tentzeris, M.K. Freynhofer, S. Farhan, R. Jarai, F. Egger, J. Wojta, A. Geppert declare that they have no conflict of interests. T. W. Weiss received lecturing fees and advisory honoraria from AstraZeneca, Daiichi Sankyo and Sanofi-Aventis. A. Kastrati received lecturing fees and advisory honoraria from The Medicines Company. G. W. Stone received lecturing fees and advisory honoraria from The Medicines Company. Kurt Huber received lecturing fees and advisory honoraria from The Medicines Company, AstraZeneca, Eli Lilly, Daiichi Sankyo and Sanofi-Aventis.
Ethical standards
All studies described in this manuscript were carried out with the approval of the responsible ethics committee and in accordance with national law and the Helsinki Declaration of 1975 (in its current revised form). Informed consent was obtained from all patients included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Rohla, M., Tentzeris, I., Freynhofer, M.K. et al. Impact of bivalirudin on mortality and bleeding complications in acute coronary syndrome patients undergoing invasive revascularization. Wien Klin Wochenschr 128, 906–915 (2016). https://doi.org/10.1007/s00508-016-1078-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-016-1078-6