
Summary
Background
The prevalence of chronic kidney disease (CKD) is rising at an alarming rate, thus presenting a substantial burden for the patient as an individual and—because of the enormous treatment costs—for society as a whole. Early diagnosis and therapy could slow disease progression and reduce the prevalence of cost-intensive end stage renal disease. The aim of this study was to determine the accuracy of diagnosis of CKD in acute patients presenting at an internal ward.
Methods
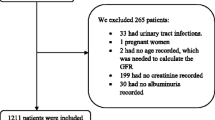
Routine laboratory parameters of kidney function of 238 inpatients were retrospectively evaluated to determine the prevalence of CKD, defined as estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2. Those results were compared with the actual documentation of the ICD-10 diagnosis CKD in the discharge reports of the respective patients.
Results
Of 238 patients, 228 patients were included in the analysis. The overall median (range) eGFR was 60.7 (10.4–171.9) mL/min/1.73 m2, with no gender-specific difference. Of patients, 49.6 % (n = 113) were retrospectively diagnosed with CKD stage 3 or higher. However, the review of the discharge reports found correct diagnosis of CKD in only 38.1 % (n = 43) of these patients.
Conclusions
The present analysis shows that CKD remains frequently unrecognized, even in a hospital setting. This could have dramatic implications on the care, treatment and prevention of CKD and associated complications.
Zusammenfassung
Hintergrund
Die chronische Niereninsuffizienz ist eine Erkrankung mit stetig zunehmender Prävalenz. Neben erhöhter Morbidität und Mortalität ist die Belastung für das Gesundheitsbudget durch die chronische Niereninsuffizienz enorm. Die frühzeitige Diagnose und Therapie kann das kostenintensive Endstadium der Krankheit verhindern bzw. zeitlich verzögern. In der aktuellen Studie wurde untersucht, zu welchem Prozentsatz eine vorhandene chronische Niereninsuffizienz bei stationären Patienten korrekt erkannt wurde.
Methodik
In einer retrospektiven Analyse wurden die Daten von 238 allgemein internistischen Akutpatienten an der Universitätsklinik für Innere Medizin Graz evaluiert und die Prävalenz der chronischen Niereninsuffizienz, definiert als geschätzte glomeruläre Filtrationsrate < 60 mL/min/1,73 m2, bestimmt. Diese Daten wurden in Hinblick auf Erfassung der Erkrankung im Entlassungsarztbrief verglichen.
Ergebnisse
Von 238 Patienten wurden 228 analysiert. Die mediane (Bereich) geschätzte glomeruläre Filtrationsrate betrug 60,7 (10,4–171,9) mL/min/1,73 m2, wobei keine geschlechtsspezifischen Unterschiede gefunden wurden. Eine chronische Niereninsuffizienz im Stadium 3 oder höher wurde bei 49,6 % der Patienten (n = 113) nachgewiesen. Die Erhebung der Diagnosen in den Entlassungsarztbriefen ergab, dass die Erkrankung bei lediglich 38,1 % der betroffenen Patienten in der ICD-10 Codierung als Solche erfasst wurde.
Schlussfolgerungen
Diese Analyse zeigt eine deutliche „Unterdiagnose“ der chronischen Niereninsuffizienz, sogar in einem stationären allgemein internistischen Setting. Das könnte dramatische Folgen für die Behandlung und Prävention der chronischen Niereninsuffizienz und ihrer assoziierten Komplikationen haben.

Similar content being viewed by others

References
Levey AS, Atkins R, Coresh J, et al. Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from kidney disease improving global outcomes. Kidney Int. 2007;72(3):247–59.
White SL, Polkinghorne KR, Atkins RC, et al. Comparison of the prevalence and mortality risk of CKD in Australia using the CKD Epidemiology Collaboration (CKD-EPI) and modification of diet in renal disease (MDRD) Study GFR estimating equations: the AusDiab (Australian diabetes, obesity and lifestyle) Study. Am J Kidney Dis. 2010;55(4):660–70.
Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–47.
OʼHare AM, Kaufman JS, Covinsky KE, et al. Current guidelines for using angiotensin-converting enzyme inhibitors and angiotensin II-receptor antagonists in chronic kidney disease: is the evidence base relevant to older adults? Ann Internal Med. 2009;150(10):717–24.
Weiner DE, Tighiouart H, Stark PC, et al. Kidney disease as a risk factor for recurrent cardiovascular disease and mortality. Am J Kidney Dis. 2004;44(2):198–206.
Keith DS, Nichols GA, Gullion CM, et al. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Internal Med. 2004;164(6):659–63.
Tonelli M, Wiebe N, Culleton B, et al. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006;17(7):2034–47.
Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305.
Anandarajah S, Tai T, de Lusignan S, et al. The validity of searching routinely collected general practice computer data to identify patients with chronic kidney disease (CKD): a manual review of 500 medical records. Nephrol Dial Transplant. 2005;20(10):2089–96.
Middleton RJ, Foley RN, Hegarty J, et al. The unrecognized prevalence of chronic kidney disease in diabetes. Nephrol Dial Transplant. 2006;21(1):88–92.
Gilbertson DT, Liu J, Xue JL, et al. Projecting the number of patients with end-stage renal disease in the United States to the year 2015. J Am Soc Nephrol. 2005;16(12):3736–41.
Foley RN, Murray AM, Li S, et al. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998–1999. J Am Soc Nephrol. 2005;16(2):489–95.
Kerr M, Bray B, Medcalf J, et al. Estimating the financial cost of chronic kidney disease to the NHS in England. Nephrol Dial Transplant. 2012;27(Suppl 3):iii73–iii80.
Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. modification of diet in renal disease study group. Ann Internal Med. 1999;130(6):461–70.
Ferris M, Shoham DA, Pierre-Louis M, et al. High prevalence of unlabeled chronic kidney disease among inpatients at a tertiary-care hospital. Am J Med Sci. 2009;337(2):93–7.
Gentile G, Postorino M, Mooring RD, et al. Estimated GFR reporting is not sufficient to allow detection of chronic kidney disease in an Italian regional hospital. BMC Nephrol. 2009;10:24.
Minutolo R, De Nicola L, Mazzaglia G, et al. Detection and awareness of moderate to advanced CKD by primary care practitioners: a cross-sectional study from Italy. Am J Kidney Dis. 2008;52(3):444–53.
Zhou XJ, Rakheja D, Yu X, et al. The aging kidney. Kidney Int. 2008;74(6):710–20.
Black C, Sharma P, Scotland G, et al. Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis. Health Technol Assess. 2010;14(21):1–184.
Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int. 2007;71(1):31–8.
KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2012;3(Suppl 1):1–150.
Kramar R, Oberbauer R. Austrian Dialysis and Transplantation Registry (OEDTR), Annual Report 2011. Austrian Society of Nephrology; 2011.
Grassmann A, Gioberge S, Moeller S, et al. ESRD patients in 2004: global overview of patient numbers, treatment modalities and associated trends. Nephrol Dial Transplant. 2005;20(12):2587–93.
Lysaght MJ. Maintenance dialysis population dynamics: current trends and long-term implications. J Am Soc Nephrol. 2002;13(Suppl 1):S37–40.
Matzke GR, Aronoff GR, Atkinson AJ Jr., et al. Drug dosing consideration in patients with acute and chronic kidney disease—a clinical update from kidney disease: improving global outcomes (KDIGO). Kidney Int. 2011;80(11):1122–37.
Hug BL, Witkowski DJ, Sox CM, et al. Occurrence of adverse, often preventable, events in community hospitals involving nephrotoxic drugs or those excreted by the kidney. Kidney Int. 2009;76(11):1192–8.
Akbari A, Grimshaw J, Stacey D, et al. Change in appropriate referrals to nephrologists after the introduction of automatic reporting of the estimated glomerular filtration rate. CMAJ. 2012;184(5):E269–E76.
Hobbs H, Stevens P, Klebe B, et al. Referral patterns to renal services: what has changed in the past 4 years? Nephrol Dial Transplant. 2009;24(11):3411–9.
National Kidney F. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–266.
Poggio ED, Nef PC, Wang X, et al. Performance of the Cockcroft—Gault and modification of diet in renal disease equations in estimating GFR in ill hospitalized patients. Am J Kidney Dis. 2005;46(2):242–52.
Newhouse JH, Kho D, Rao QA, et al. Frequency of serum creatinine changes in the absence of iodinated contrast material: implications for studies of contrast nephrotoxicity. AJR. 2008;191(2):376–82.
Kurtal H, Schwenger V, Azzaro M, et al. Clinical value of automatic reporting of estimated glomerular filtration rate in geriatrics. Gerontology. 2009;55(3):288–95.
Conflict of interest
All authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Friedl, C., Hemetsberger, M., Mader, J. et al. Awareness of chronic kidney disease in Austria: a frequently under-recognized clinical picture. Wien Klin Wochenschr 125, 362–367 (2013). https://doi.org/10.1007/s00508-013-0374-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-013-0374-7