
Abstract
Air pollution is considered the most prominent public health. Economically, air pollution imposes additional costs on governments. This study aimed to quantify health effects and associated economic values of reducing PM2.5 air pollution using BenMAP-CE in Qom in 2019. The air quality data were acquired from Qom Province Environmental Protection Agency, and the population data were collected from Qom Province Management and Planning Organization website. The number of deaths due to Stroke, Chronic Obstructive Pulmonary Disease, Lung Cancer, and Ischemic Heart Disease attributable to PM2.5 were estimated using BenMAP-CE based on two control scenarios, 2.4 and 10 μg/m3, known as scenarios I and II, respectively. The associated economic effect of premature deaths was assessed by value of a statistical life (VSL) approach. The annual average of PM2.5 concentration was found to be 16.32 μg/m3 (SD: 9.93). A total of 4694.5 and 2475.94 premature deaths in scenarios I and II were found to be attributable to PM2.5 in overall, respectively. The total associated cost was calculated to be 855.91 and 451.40 million USD in scenarios I and II, respectively. The total years of life lost due to PM2.5 exposure in 2019 was 158,657.06 and 78,351.51 in scenarios I and II, respectively. The results of both health and economic assessment indicate the importance of solving the air pollution problem in Qom, as well as other big cities in Iran. The elimination of limitations, such as insufficient local data, should be regarded in future studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Environmental pollution is a global concern with enormous potential to negatively influence the population. Over the last decades, there have been increasing concerns over the public health effects attributable to environmental pollution, especially in developing countries like Iran (Khan and Ghouri 2011; Mojarrad et al. 2020). Air pollution is considered one of the most prominent public health (WHO 2021) and environmental hazard in the world (Ansari and Ehrampoush 2019), primarily arising from traffic as well as industrial and residential activities (Tohid et al. 2019). The range of the adverse effects of air pollution is wide, exerted in direct and indirect ways (Fouladi-Fard et al. 2018a; Ansari and Ehrampoush 2019; WHO 2021). Exposure to air pollution increases the risk of death and hospitalization due to cardiovascular and respiratory diseases, type 2 diabetes, hypertension, and various types of cancer (Yousefi et al. 2019; Tainio et al. 2021; Zhao 2022); in addition to effects of air pollution on physical health; recent studies have shown the possibility of negative effects of air pollutants on brain and mental health, such as cognitive decline, neurodegenerative disease, and Alzheimer’s disease (AD), (Alemany et al. 2021; Balboni et al. 2022). Also; some recent studies on the association between air pollution and COVID-19 have shown long-term exposure to air pollution did not increase the number of cases, but the amount of antibodies was higher in infected and exposed individuals. This means that body was facing a severe disease or infection (Kogevinas et al. 2021) and one study found a relationship between increase of COVID-19 cases and NO2 pollution in Italy (Filippini et al. 2021); of note, 90% of the world’s population live in areas where air pollution exceeds World Health Organization’s (WHO) guidelines (Tainio et al. 2021).
The major sources of emissions from human interventions regarding suspended particles are road traffic (10–25%), fuel combustion (55–40%), and industrial activities (15–30%) (Wark k, Warner CF, Wayne D, 1981). The WHO reported seven million deaths from outdoor and indoor air pollution in 2016 worldwide (World Health Organization, 2018), and 4.2 million deaths occur each year because of exposure to ambient air pollution (Yousefi et al. 2019). Research shows that among air pollutants, particles in the form of total suspended particles (TSP), PM2.5, and PM10 (particulate matter with aerodynamic diameters less than 2.5 and 10 μm) can lead to the most harmful consequences among other air pollutants (Kan and Chen 2004; Fard et al. 2016, 2021; Rezaali et al. 2021).
Economically, air pollution imposes additional costs on governments. The annual costs of health insurance, treatment of diseases, and rehabilitation are just some of the negative economic effects of air pollution (Ansari and Ehrampoush 2019). Low- and middle-income countries incur high costs each year due to non-communicable diseases such as cardiovascular and respiratory diseases (Kalantari et al. 2018). The results of a study in Chile showed that air pollution has a negative impact on welfare, and Chileans are willing to pay a monthly fee to reduce 1 μg/m3 PM2.5 pollution (Ahumada and Iturra 2021). On the other hand, economic growth is known as one of the causes of air pollution (Chen and Chen 2021).
Various methods have been used to estimate the concentration of ambient air pollution and health consequences such as concentration–response functions (C-R), linear and logistic. There are several pieces of software for estimating the health and economic effects associated with air quality changes, such as AirQ, BenMAP-CE, EBD, GMAPS, SIM-AIR, and IOMLIFET (Anenberg et al. 2016; Bayat et al. 2019). BenMAP-CE (Environmental Benefits Mapping and Analysis Program-Community Edition) programmed by the US Environmental Protection Agency can be considered one of the most comprehensive software and can be used to calculate both mortality and costs associated with changes in air quality (Bayat et al. 2019; Kim et al. 2019a, b). Since the release of this software, various studies have employed the software to assess the health and economic effects of air pollutants (Ding et al. 2016; Sacks et al. 2018, 2020; Bayat et al. 2019; Meng et al. 2019; Mirzaei et al. 2021).
The quantification of the effects of air pollution clearly defines the public health implications of poor air quality. Informing people and governments on the effects of air pollution on human health and convincing authorities to implement policies to reduce air pollution to reduce morbidity, mortality, and economic costs are among the benefits of such studies. Iran is facing rapid industrial growth, having a large number of old vehicles and confronting environmental crises such as the Middle East dust storm. The Environmental Protection Agency has developed programs and measures to control air pollution including the replacement of fuels in mobile sources and power plants, replacing worn-out cars, and using dual-fuel and smokeless cars. Monitoring and conducting health effects of air pollutants can be an effective measure to evaluate the implemented interventions (Hopke et al. 2018). Although some research has been conducted on air pollution and its negative effects in other cities of Iran, to the best of the authors’ knowledge, no study has been carried out in this regard in Qom thus far. Consequently, this study aimed at quantifying health effects and associated economic values of the four major health endpoints attributable to PM2.5 air pollution including Stroke, chronic obstructive pulmonary disease (COPD), lung cancer (LC), and ischemic heart disease (IHD) using BenMAP-CE in Qom in 2019.
Materials and methods
Study area and data collection
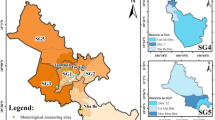
Qom is the capital of Qom Province with eight municipality districts and 26 sub-districts.(as shown in Fig. 1) (Safari et al. 2021); it is located in the central region of Iran, 130 km to the southwest of Tehran. It has a dry and semi-dry climate with an annual rainfall of 161 mm (Khazaei et al. 2013; Fahiminia et al. 2016; Fouladi-Fard et al. 2018b). Similar to some cities in Iran, Qom is facing the phenomenon of dust, which is due to having desert space (15.7% of the province) and wind erosion centers. Two of the most important centers of dust in the city are Masileh plain and Qom salt lake (Raoufi-fard and Ramouz 2017). Qom Province is one of those provinces that will be negatively influenced if global warming enhances (Basiri et al. 2021).

Study area and population distribution in Qom
The hourly PM2.5 was obtained from Qom Province Environmental Protection Agency for 2019. To reach the maximum amount of data for evaluation (above 75%), missing data were interpolated by linear method. The population data were collected from Qom Province Management and Planning Organization website (Qom Province Management and Planning Organization website 2021). As the latest census was done in 2016, the population for the year 2019 was estimated based on Eq. 1 (Mirzaei et al. 2021):
where Pn is the estimated population, P0 is the reference population, r is the population growth rate, and n is the number of years between reference and future (Karimi et al. 2019; Mirzaei et al. 2021). According to the purpose of this study, the population at risk included people more than 30 year-old.
Health and economic impact assessment
BenMAP-CE (version: 1.5.0.4) was utilized to conduct this study. BenMAP-CE is an EPA model to quantify premature mortality and morbidity related to air pollution (Kim et al. 2019a, b). This model employs concentration changes between control and baseline scenario and population and health concentration–response (C-R) functions to estimate the number of affected people. This tool is also capable of calculating the cost–benefit of concentration changes (Howard et al. 2019). It is a Geographic Information System (GIS)-based program (Chen et al. 2017) that estimates the effects of air pollutant concentration changes on human health and economic benefits of this change (Liang et al. 2019). To do so, in addition to the air pollutant concentration changes (baseline and control scenario), it needs population data, baseline incidence rates for the health endpoints, C-R functions, and valuation functions. A Monte Carlo approach which results in 95% confidence intervals around each mean health impact estimate is applicable in BenMAP-CE (Altieri and Keen 2019). Health benefits of reducing air pollutants (ΔY) in BenMAP-CE were investigated by Eq. 2:
where BI is baseline incidence rates, the ratio of number of deaths to the population size in a period of time (Farzad et al. 2021), and Pop is the given population exposed to the pollutant (Bayat et al. 2019). DELTAQ is the difference between the current pollutant concentration (baseline scenario) and the target concentration (control scenario) (Liang et al. 2019; Farzad et al. 2020; Mirzaei et al. 2021). β, the exposure–response coefficient (Zhu et al. 2019), is a statistical coefficient derived from epidemiological analysis calculating the relationship between health endpoint and air pollution concentration which varies for different health impact functions (Yang et al. 2019) and is calculated through Eq. 3:
where RR is the relative risk and ΔC is the change in pollutant concentration used to estimate the relative risk (Khaniabadi et al. 2017).
As shown in Table 1, the baseline incidences (BI) related to the four health outcomes were obtained from Global Burden of Disease (GBD) website (Global Burden of Disease, Institute for Health Metrics and Evaluation website 2021). The Relative Risks associated with Stroke and COPD were obtained from GBD website (Global Burden of Disease, Institute for Health Metrics and Evaluation website 2021) and Relative Risks associated with LC and IHD were obtained from an epidemiological study (Krewski et al. 2009).
In addition to mortality, the following Eq. was used to compute years of life lost (YLL) in each age group.
where YLL is the years of life lost attributable to PM2.5, \(\Delta Y\) is the avoidable mortality derived from Eq. 2, and L is the remaining life expectancy. In this study, we utilized life expectancy tables from GDB website for Iran (Bayat et al. 2019).
There are two approaches frequently used to calculate the economic cost of premature death including the value of a statistical life (VSL) and the value of a life year (VOLY). VSL is based on individual willingness to pay (WTP) to decrease the risk of death, while VOLY is based on individual willingness to pay to expand the life expectancy by one additional year (Chiabai et al. 2018; Bayat et al. 2019). WTP not only considers the intangible costs including the value of suffering and the value of leisure time lost but also demonstrates the tangible costs of medical treatment (Zhu et al. 2019). To assess the economic benefits in this study, the simplest approach was used, which is to multiply the predicted number of deaths by a locally valid estimate of VSL. In fact, local studies should be utilized to estimate the economic loss. Owing to the absence of such local studies, however, we used the benefit-transfer approach to transfer unit health costs from foreign studies to the local context by Eq. 5 (Narain and Sall 2016; Bayat et al. 2019):
where Y is GDP (gross domestic product) per capita and b is the income elasticity of VSL. For low- and middle-income countries, b differs from 1.0 to 1.4, with a central estimate of 1.2 (Bayat, et al. 2019). The detailed calculations of VSL are shown in Table 2.
Scenarios
The baseline scenario is identified as the environmental concentration of considered pollutant in the current situation. The baseline scenario in this study was the annual average concentration of PM2.5 in 2019. The control scenario is defined as the ideal or target condition. Two control scenarios, 2.4 μg/m3 and 10 μg/m3 (the WHO annual guideline) known as scenarios I and II, were designed to be surveyed. Two point four μg/m3 is the lowest measure in Global Burden of Disease calculations in AirQ+ by default, and it has been utilized in some studies (Bayat et al. 2019; Evangelopoulos et al. 2020). In BenMAP-CE, the health assessment and associated economic valuation are based on the difference between these two scenarios.
Sensitivity analysis
The following two alternative approaches were applied to check the sensitivity of the results in BenMAP-CE for both scenarios. (1) We used AirQ+ (version 2) with the same BI and RR to investigate premature death due the four outcomes. In order to check whether our evaluation and calculations by BenMAP-CE were correct (because BenMAP-CE settings and functions are set for USA by default, all the necessary functions and settings in BenMAP-CE were done manually in this study), AirQ+ was applied to this study which uses as same input function as BenMAP-CE (the function mentioned in “Scenarios”). 2) Because the sum of age group estimates is expected to be equal to the overall estimates, we estimated premature deaths for a single age category (30–99). It is noteworthy that the sensitivity analysis was taken from a similar study conducted in Tehran (Bayat et al. 2019).
Results
Descriptive results
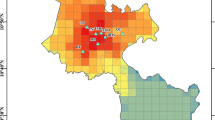
The annual average of PM2.5 concentration was found to be 16.39 μg/m3 with a standard deviation of 9.93. The mean concentration was about 1.6 times more than the WHO annual concentration guideline (10 μg/m3). Moreover, our analysis showed that daily PM2.5 concentrations were more than 35 μg/m3 (EPA daily concentration guideline) in 16 days and more than 25 μg/m3 (WHO daily concentration guideline) in 42 days in 2019. PM2.5 concentration statistics, including mean, SD, minimum, maximum, and 75 and 25 percentiles are demonstrated in Table 3. To study the process of decreasing or increasing PM2.5 concentration, PM2.5 concentration for 2 years before the study year was also reported. It should be noted that the data for 2017 and 2018 were calculated from hourly data and have not been interpolated. Detailed concentration of PM2.5 from April to March 2019 which is based on Iranian calendar is shown in Fig. 2. The highest concentration occurred in August, September, and October in 2019.

PM2.5 concentration distribution during study time
Health and economic impact assessment
The estimated number of premature deaths attributable to PM2.5 using BenMAP-CE by defined scenarios in 2019 is presented in Table 4. In addition, the total valuation results are given in Table 4 as well. According to Table 4, in scenario I (2.4 μg/m3), 1498.6, 711.57, 27.74, and 2456.59 deaths for stroke, COPD, LC, and IHD, respectively, attributable to PM2.5 were estimated using BenMAP-CE. The total cost associated with total mortality in each cause of death was 273,227,013, 129,732,870, 5,047,581.61, and 447,894,726 USD, respectively. In scenario II (10 μg/m3), 2475.94 premature deaths attributable to PM2.5 were estimated in overall. The total cost associated with total mortality calculated by BenMAP-CE was found to be 451,390,599.72 USD in overall. In fact, if the annual average concentration of PM2.5 were 10 or if the annual average concentration of PM2.5 had decreased to 10, 2,475.94 premature mortalities due to four defined health endpoints would not have occurred and the economic benefit of this reduction would have been 451,390,599.72 USD in 2019.
Figure 3 demonstrates the percentage share of each outcome in terms of health effects in both scenarios. Figures 4 and 5 show mortality and associated cost for each health outcome in municipality districts for scenario I and II, respectively. Bold colors indicate higher mortality or greater economic impact.

Percentage share of each outcome in terms of health effects

Total mortality (red range) and associated cost (purple range) (USD) in scenario I (2.4 μg/m.3) for stroke (a), COPD (b), LC (c), and IHD (d)

Total death (red range) and associated cost (purple range) (USD) in scenario II (10 μg/m.3) for stroke (a), COPD (b), LC (c), and IHD (d)
Table 5 demonstrates the results of YLL for each age group. 40,255.33, 26,362.32, 1027.12, and 91,012.29 years of life lost were estimated for scenario I (2.4 μg/m3) due to stroke, COPD, LC, and IHD mortality, respectively. In scenario II (10 μg/m3), years of life lost due to stroke, COPD, LC, and IHD mortality in adults were found to be 33,837.27, 13,617.77, 488.63, and 30,407.84, respectively.
Sensitivity of results
Table 6 shows the difference between main results and results of alternative approaches. Using AirQ+, − 0.07% and − 0.11% differences were observed in scenarios I (2.4 μg/m3) and II (10 μg/m3), respectively. A slight variation discovered in applying 30–99 age group estimation.
Discussion
This study was confirmed to discuss a serious public health issue, air pollution. It was limited to conduct health assessment of stroke, COPD, LC, and IHD mortality attributable to PM2.5 and evaluation of associated economic cost in 2019 in Qom.
An increase was observed in PM2.5 concentration during summer. The increase in this period may be due to the dry climate and the presence of dust centers (Raoufi-fard and Ramouz 2017). According to available data and statistical analysis; the PM2.5 mean concentration in 2017 was much higher than standard concentration. But this amount was close to each other in 2018 and 2019; with the difference that in 2019, PM2.5 mean concentration showed an upward trend. This indicates the variability of PM2.5 concentration in the city, which shows regular and accurate monitoring should be applied.
In the current study, the highest number of mortality was related to IHD as well as in a study in Abadan which the highest premature mortality calculated by AirQ+ was due to ischemic heart disease (Fanaei et al. 2020). In another study using BenMAP-CE, the first ranking for mortality was dedicated to IHD, as well (Bayat et al. 2019). These results are due to high risk of IHD attributed to PM2.5 derived from epidemiological studies in Iran. Since the highest number of deaths in this study occurred in IHD mortality, the highest associated cost was related to this outcome in both scenarios. This is due to the basis of BenMAP-CE and the monetary function used in this study that the higher the mortality, the higher the cost is. According to WTP, these costs include treatment and intangible costs. By saving it, the general material and spiritual well-being is achieved. The noticeable difference in both economic and health results was that PM2.5 reduction in the first scenario was more beneficial, because the difference between baseline and control scenario was greater.
According to the Figs. 4 and 5, in 2019, the southern and eastern areas have suffered lower mortality and associated cost. The central area has suffered the least damage in all figures. This may be due to the fact that most of the center area is made up of marketplaces and holly shrine and there are fewer residential areas. The northern regions and areas with bold color will be the areas that benefit the most from PM2.5 reduction. YLL results show the effect of PM2.5 on reducing life years. The higher the pollution, the higher the mortality and the greater the number of years lost.
As shown in Table 6, there was a very slight difference between applying the 5-year age group and single age group which means our expectation has been met. According to the results, there was a limited difference in results using AirQ+ and BenMAP-CE. This shows that if the input functions are the same, the results are not very different and both software can be used together or separately as a tool for health impact assessment (Sacks et al. 2020). A slight difference was observed in similar previous studies comparing results in BenMAP-CE and AirQ+ (Bayat et al. 2019; Sacks et al. 2020; Mirzaei et al. 2021). Given the differences and similarities between AirQ+ and BenMAP-CE, the main difference in BenMAP-CE that has made it superior is the possibility of calculating the associated economic value of reducing pollutants. It is also possible to perform assessments by age in BenMAP-CE. In addition, different functions can be inputted and the results can be checked based on different functions. It is also possible to pool health and monetary functions. The possibility of displaying the results on GIS map is another advantage of BenMAP-CE. BenMAP-CE is not friendly use while AirQ+ is a friendly use tool. AirQ+ is very simple and due to the lack of GIS program, the installation and application is faster and as the comparison showed, the results obtained from AirQ+ were equal to BenMAP-CE.
In a study conducted by Hadei (2020), it was observed that the annual concentration of PM2.5 was 1.5–6 times more than 10 μg/m3 in 25 Iranian cities in 2017. Qom was one of the aimed cities in this study. Health impact assessment was conducted using AirQ+, and associated economic values were estimated by VSL approach. VSLIran was estimated equal to 373,819.62 USD in 2017. The estimated number of COPD, LC, IHD, and stroke deaths attributable to long-term PM2.5 exposure exceeding WHO level in Qom was 532. The total associated economic value was estimated to be 5.8 billion USD in 25 Iranian cities. A study conducted by Bayat et al. investigated avoidable mortality burden attributable to PM2.5 using BenMAP-CE in Tehran in 2017. They utilized global exposure mortality model (GEMM) to estimate the health and economic burden of air pollution. Based on their results, 7146 deaths were related to PM2.5 in total, 3437 mortalities due to IHD, 886 due to stroke, and 531, 364, and 274 due to LRI, COPD, and LC, respectively. The estimated YLL due to ambient PM2.5 exposure in Tehran in 2017 was equal to 109,168. The total economic benefit of the control scenario to 2.4 μg/m3 was estimated to be 2.894 billion USD using VSL. In addition to VSL, they used another approach (VOLY) to calculate the economic benefits of morbidity. Through this approach, the economic benefit was calculated to be 0.591 billion USD in the same scenario (Bayat et al. 2019). We did not consider this approach in our analysis. In one study in the USA, BenMAP-CE was used to estimate the reduction in preterm birth (PTB) due to PM2.5 depletion. According to previous studies, one of the causes of PTB is air pollution. The results showed that a 10% reduction in PM2.5 concentration from 2008 equaled a reduction of 5016 PTB and 339 million USD in economic benefit in 2014 (Kim et al. 2019a, b). Similarly, a study in Tehran compared the two software. They analyzed PM2.5 changes to 10 μg/m3 and its effects on health in 2016–2018. The estimated number of deaths using both AirQ+ and BenMAP-CE were the same, and the number of mortalities was assessed to be 4383, 412, and 96 for all causes, IHD, and LC, respectively. The reason for exact results may be because of the same input functions and variables (Mirzaei et al. 2021).
Sacks et al. indicated that BenMAP-CE and AirQ+ well align in the calculation of health impacts. They utilized same input function and data to compare the results of all-cause mortality based on control scenario of 10 μg/m3 PM2.5. Based on their results, 965 and 966 all-cause mortality was estimated using BenMAP-CE and AirQ+, respectively (Sacks et al. 2020). In China, BenMAP-CE was used to assess health and economic benefits attributable to PM2.5 for reaching the annual concentration of 35 μg/m3 in 2014. The avoided deaths for cardiovascular disease, respiratory disease, and LC were found to be 89,000, 47,000, and 32,000, respectively. Total economic benefits for this control scenario were estimated to be 260 billion RMB using the WTP approach. Also, the mean concentration of PM2.5 was 51.69 μg/m3 (Chen et al. 2017). The high number of deaths is not unlikely due to the high PM2.5 concentration in a year as well as China’s large population.
Conclusions
The results highlight the importance of solving air pollution problems in Qom, as well as other big cities in Iran. Due to the fact that with development of industry and societies, air pollution will also increase; if a solution is not considered, it can turn into a disaster. Due to global warming and recent droughts, some dust centers around Qom are expected to intensify, which could locally exacerbate particulate air pollution. The economic effects of air pollution impose a burden on both societies and governments. Also, the reduction of spiritual costs makes people enjoy higher welfare. Performing assessments by age, entering different health and monetary functions, pooling health and monetary functions, and displaying the results on GIS map are the advantages of health and economic impact assessment using BenMAP-CE.
Limitations, strengths, and suggestions for future research
The lack of local studies for both health and valuation functions was the limitation. Future studies need to remove this limitation. On the other hand, the novelty of the subject is the greatest strength of the current study. To date, no study has been conducted to survey the health and economic effects of PM2.5 in Qom.
Data availability
Available data on VSL calculation:
https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=IR; https://fred.stlouisfed.org/series/NYGDPPCAPCDOED
References
Ahumada G, Iturra V (2021) If the air was cleaner, would we be happier? An economic assessment of the effects of air pollution on individual subjective well-being in Chile. J Clean Prod 289:125152. https://doi.org/10.1016/j.jclepro.2020.125152
Alemany S, Crous-Bou M, Vilor-Tejedor N, Milà-Alomà M, Suárez-Calvet M, Salvadó G et al (2021) Associations between air pollution and biomarkers of Alzheimer’s disease in cognitively unimpaired individuals. Environ Int 157:106864. https://doi.org/10.1016/j.envint.2021.106864
Altieri KE, Keen SL (2019) Public health benefits of reducing exposure to ambient fine particulate matter in South Africa. Sci Total Environ 684:610–620. https://doi.org/10.1016/j.scitotenv.2019.05.355
Anenberg SC, Belova A, Brandt J, Fann N, Greco S, Guttikunda S et al (2016) Survey of ambient air pollution health risk assessment tools. Risk Anal 36(9):1718–1736. https://doi.org/10.1111/risa.12540
Ansari M, Ehrampoush MH (2019) Meteorological correlates and AirQ+ health risk assessment of ambient fine particulate matter in Tehran. Iran Environ Res 170:141–150. https://doi.org/10.1016/j.envres.2018.11.046
Balboni E, Filippini T, Crous-Bou M, Guxens M, Erickson LD, Vinceti M (2022) The association between air pollutants and hippocampal volume from magnetic resonance imaging: a systematic review and meta-analysis. Environ Res 204(Pt A):111976. https://doi.org/10.1016/j.envres.2021.111976
Basiri SM, Akhbari M, Fr Abdolreza, Borna R (2021) Mapping the regions of the country of Iran based on geopolitical indicators of climate change impacts. Nat hazards 10(27):123–44. https://doi.org/10.22111/jneh.2020.33474.1629
Bayat R, Ashrafi K, Motlagh MS, Hassanvand MS, Daroudi R, Fink G et al (2019) Health impact and related cost of ambient air pollution in Tehran. Environ Res 176:108547. https://doi.org/10.1016/j.envres.2019.108547
Chen F, Chen Z (2021) Cost of economic growth: air pollution and health expenditure. Sci Total Environ 755:142543. https://doi.org/10.1016/j.scitotenv.2020.142543
Chen L, Shi M, Gao S, Li S, Mao J, Zhang H et al (2017) Assessment of population exposure to PM2. 5 for mortality in China and its public health benefit based on BenMAP. Environ Pollut 221:311–317. https://doi.org/10.1016/j.envpol.2016.11.080
Chiabai A, Spadaro JV, Neumann MB (2018) Valuing deaths or years of life lost? Economic benefits of avoided mortality from early heat warning systems. Mitig Adapt Strateg Glob Change 23(7):1159–1176. https://doi.org/10.1007/s11027-017-9778-4
Ding D, Zhu Y, Jang C, Lin C-J, Wang S, Fu J et al (2016) Evaluation of health benefit using BenMAP-CE with an integrated scheme of model and monitor data during Guangzhou Asian Games. J Environ Sci 42:9–18. https://doi.org/10.1016/j.jes.2015.06.003
Economic Research website (2021). https://fred.stlouisfed.org/series/NYGDPPCAPCDOED. Accessed 8 August 2021
Evangelopoulos D, Perez-Velasco R, Walton H, Gumy S, Williams M, Kelly FJ et al (2020) The role of burden of disease assessment in tracking progress towards achieving WHO global air quality guidelines. Int J Public Health 65(8):1455–1465. https://doi.org/10.1007/s00038-020-01479-z
Fahiminia M, Fard RF, Ardani R, Naddafi K, Hassanvand M, Mohammadbeigi A (2016) Indoor radon measurements in residential dwellings in Qom. Iran. Int. J. Radiat. Res 14(4):331. https://doi.org/10.18869/acadpub.ijrr.14.4.33
Fanaei F, Ghorbanian A, Shahsavani A, Jafari AJ, Abdolahnejad A, Kermani M (2020) Quantification of mortality and morbidity in general population of heavily-industrialized city of Abadan: Effect of long-term exposure. Journal of Air Pollution and Health 5(3):171–80. https://doi.org/10.18502/japh.v5i3.5390
Fard RF, Naddafi K, Yunesian M, Nodehi RN, Dehghani MH, Hassanvand MS (2016) The assessment of health impacts and external costs of natural gas-fired power plant of Qom. Environ Sci Pollut Res 23(20):20922–20936. https://doi.org/10.1007/s11356-016-7258-0
Fard RF, Torkamani FD, Mahvi AH, Fahiminia M, Koolivand A, Hosseini MR, et al (2021) Health effects from particulate air pollution in one of the industrial cities of Iran. Journal of Air Pollution and Health https://doi.org/10.18502/japh.v6i2.7955
Farzad K, Khorsandi B, Khorsandi M, Bouamra O, Maknoon R (2020) A study of cardiorespiratory related mortality as a result of exposure to black carbon. Sci Total Environ 725:138422. https://doi.org/10.1016/j.scitotenv.2020.138422
Farzad K, Khorsandi B, Khorsandi M, Bouamra O, Maknoon R (2021) Estimating short-term mortality benefits associated with a reduction in tropospheric ozone. Atmos Environ 252:118342. https://doi.org/10.1016/j.atmosenv.2021.118342
Filippini T, Rothman KJ, Cocchio S, Narne E, Mantoan D, Saia M et al (2021) Associations between mortality from COVID-19 in two Italian regions and outdoor air pollution as assessed through tropospheric nitrogen dioxide. Sci Total Environ 760:143355. https://doi.org/10.1016/j.scitotenv.2020.143355
Fouladi-Fard R, Naddafi K, Hassanvand MS, Khazaei M, Rahmani F (2018a) Trends of metals enrichment in deposited particulate matter at semi-arid area of Iran. Environ Sci Pollut Res 25(19):18737–18751. https://doi.org/10.1007/s11356-018-2033-z
Fouladi-Fard R, Hosseini M, Faraji M, Oskouei AO (2018b) Building characteristics and sick building syndrome among primary school students. Sri Lanka J Child Health 47(4):332–337. https://doi.org/10.4038/sljch.v47i4.8595
Hadei M, Shahsavani A, Krzyzanowski M, Querol X, Stafoggia M, Nazari SSH et al (2020) Burden of mortality attributed to PM2 5 exposure in cities of Iran; contribution of short-term pollution peaks. Atmos. Environ 224:117365. https://doi.org/10.1016/j.atmosenv.2020.117365
Hopke PK, Nazari SSH, Hadei M, Yarahmadi M, Kermani M, Yarahmadi E et al (2018) Spatial and temporal trends of short-term health impacts of PM2 5in Iranian cities: a modelling approach (2013â 2016). Aerosol Air Qual Res 18(2):497–504. https://doi.org/10.4209/aaqr.2017.09.0325
Howard DB, Thé J, Soria R, Fann N, Schaeffer R, Saphores J-DM (2019) Health benefits and control costs of tightening particulate matter emissions standards for coal power plants—the case of Northeast Brazil. Environ Int 124:420–430. https://doi.org/10.1016/j.envint.2019.01.029
Global Burden of Disease, Institute for Health Metrics and Evaluation website (2021). https://vizhub.healthdata.org/gbd-compare/arrow. Accessed 8 August 2021
Kalantari R R, Kermani M, Dolati M, Joneidi J A (2018) Evaluation of the number of deaths, chronic obstructive pulmonary disease and acute myocardial infarction due to exposure to sulfur dioxide in Tehran. Kumesh 20(1):34–42. http://umj.umsu.ac.ir/browse.php?a_code=A-10-2688-1&sid=1&slc_lang=en
Kan H, Chen B (2004) Particulate air pollution in urban areas of Shanghai, China: health-based economic assessment. Sci Total Environ 322(1):71–79. https://doi.org/10.1016/j.scitotenv.2003.09.010
Karimi A, Shirmardi M, Hadei M, Birgani YT, Neisi A, Takdastan A et al (2019) Concentrations and health effects of short-and long-term exposure to PM2.5, NO2, and O3 in ambient air of Ahvaz city, Iran (2014–2017). Ecotoxicol Environ Saf 180:542–548. https://doi.org/10.1016/j.ecoenv.2019.05.026
Khan MA, Ghouri AM (2011) Environmental pollution: its effects on life and its remedies. Res. world - j. arts sci 2(2):276–85. https://ssrn.com/abstract=1981242
Khaniabadi YO, Hopke PK, Goudarzi G, Daryanoosh SM, Jourvand M, Basiri H (2017) Cardiopulmonary mortality and COPD attributed to ambient ozone. Environ Res 152:336–341. https://doi.org/10.1016/j.envres.2016.10.008
Khazaei M, Mahvi AH, Fard RF, Izanloo H, Yavari Z, Tashayoei HR (2013) Dental caries prevalence among schoolchildren in urban and rural areas of Qom Province, Central part of Iran. Middle-East J Sci Res 18(5):584–591. https://doi.org/10.5829/idosi.mejsr.2013.18.5.81155
Kim D, Kim J, Jeong J, Choi M (2019) Estimation of health benefits from air quality improvement using the MODIS AOD dataset in Seoul. Korea. Environ. Res 173:452–61. https://doi.org/10.1016/j.envres.2019.03.042
Kim JJ, Axelrad DA, Dockins C (2019b) Preterm birth and economic benefits of reduced maternal exposure to fine particulate matter. Environ Res 170:178–186. https://doi.org/10.1016/j.envres.2018.12.013
Kogevinas M, Castaño-Vinyals G, Karachaliou M, Espinosa A, de Cid R, Garcia-Aymerich J et al (2021) Ambient air pollution in relation to SARS-CoV-2 infection, antibody response, and COVID-19 disease: a cohort study in Catalonia, Spain (COVICAT study). Environ Health Perspect 129(11):117003. https://doi.org/10.1289/ehp9726
Krewski D, Jerrett M, Burnett RT, Ma R, Hughes E, Shi Y, et al (2009) Extended follow-up and spatial analysis of the American Cancer Society study linking particulate air pollution and mortality: Health Effects Institute Boston, MA.
Liang S, Li X, Teng Y, Fu H, Chen L, Mao J et al (2019) Estimation of health and economic benefits based on ozone exposure level with high spatial-temporal resolution by fusing satellite and station observations. Environ Pollut 255:113267. https://doi.org/10.1016/j.envpol.2019.113267
Meng C, Liu J, Li Y, Han J, Xu D (2019) Application of BenMAP-CE software in health risk assessment of air pollution in China. Wei Sheng Yan Jiu 48(4):659–663 (PMID: 31601355)
Mirzaei A, Tahriri H, Khorsandi B (2021) Comparison between AirQ+ and BenMAP-CE in estimating the health benefits of PM 2.5 reduction. Air Qual Atmos Health 14(6):807–15. https://doi.org/10.1007/s11869-021-00980-5
Mojarrad H, FouladiFard R, Rezaali M, Heidari H, Izanloo H, Mohammadbeigi A et al (2020) Spatial trends, health risk assessment and ozone formation potential linked to BTEX. Hum Ecol Risk Assess 26(10):2836–2857. https://doi.org/10.1080/10807039.2019.1688640
Narain, U., Sall, C (2016) Methodology for valuing the health impacts of air pollution: discussion of challenges and proposed solutions. World Bank. http://hdl.handle.net/10986/24440
Qom Province Management and Planning Organization (2021). https://www.mporg.ir/Portal/View/Page.aspx?PageId=7576ef2e-e50f-4cb2-b423-b52886bc48ae. Accessed 8 August 2021
Raoufi-fard M, Ramouz M (2017) Statistical and descriptive study of the occurrence of dust phenomenon in Qom province. The first conference on the salt lake crisis and the dust phenomenon in the central basin of Iran; Qom. https://civilica.com/doc/635872/
Rezaali M, Fouladi-Fard R, Mojarad H, Sorooshian A, Mahdinia M, Mirzaei N (2021) A wavelet-based random forest approach for indoor BTEX spatiotemporal modeling and health risk assessment. Environ Sci Pollut Res 28(18):22522–22535. https://doi.org/10.1007/s11356-020-12298-3
Sacks JD, Lloyd JM, Zhu Y, Anderton J, Jang CJ, Hubbell B et al (2018) The Environmental Benefits Mapping and Analysis Program-Community Edition (BenMAP–CE): a tool to estimate the health and economic benefits of reducing air pollution. Environ Model Softw 104:118–129. https://doi.org/10.1016/j.envsoft.2018.02.009
Sacks JD, Fann N, Gumy S, Kim I, Ruggeri G, Mudu P (2020) Quantifying the public health benefits of reducing air pollution: critically assessing the features and capabilities of WHO’s AirQ+ and US EPA’s environmental benefits mapping and analysis program—Community edition (BenMAP—CE). Atmosphere 11(5):516. https://doi.org/10.3390/atmos11050516
Safari Z, Fouladi-Fard R, Vahidmoghadam R, Hosseini MR, Mohammadbeigi A, OmidiOskouei A et al (2021) Awareness and Performance towards Proper Use of Disinfectants to Prevent COVID-19: The Case of Iran. Int J Environ Res Public Health 18(4):2099. https://doi.org/10.3390/ijerph18042099
Tainio M, Jovanovic Andersen Z, Nieuwenhuijsen MJ, Hu L, de Nazelle A, An R et al (2021) Air pollution, physical activity and health: A mapping review of the evidence. Environ Int 147:105954. https://doi.org/10.1016/j.envint.2020.105954
Tohid L, Sabeti Z, Sarbakhsh P, Benis KZ, Shakerkhatibi M, Rasoulzadeh Y et al (2019) Spatiotemporal variation, ozone formation potential and health risk assessment of ambient air VOCs in an industrialized city in Iran. Atmos Pollut Res 10(2):556–563. https://doi.org/10.1016/j.apr.2018.10.007
Wark k, Warner CF, Wayne D (1981) air pollution. its origin and control.
World Bank website (2021). https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=IR. Accessed 8 August 2021
World Health Organization (2018) Burden of disease from the joint effects of household and ambient air pollution for 2016. Social and Environmental Determinants of Health Departmen, Geneva
World Health Organization. Regional Office for Europe (2021). Review of evidence on health aspects of air pollution: REVIHAAP project: technical report. World Health Organization.Regional Office for Europe. https://apps.who.int/iris/handle/10665/341712
Yang P, Zhang Y, Wang K, Doraiswamy P, Cho S-H (2019) Health impacts and cost-benefit analyses of surface O3 and PM2 5 over the US under future climate and emission scenarios. Environ Res 178:108687. https://doi.org/10.1016/j.envres.2019.108687
Yousefi S, Shahsavani A, Hadei M (2019) Applying EPA’s instruction to calculate air quality index (AQI) in Tehran. Journal of Air Pollution and Health 4(2):81–6. https://doi.org/10.18502/japh.v4i2.1232
Zhao M, Xu Z, Guo Q et al (2022) Association between long-term exposure to PM2.5 and hypertension: a systematic review and meta-analysis of observational studies. Environ Res 204:112352
Zhu B, Pang R, Chevallier J, Wei Y-M, Vo D-T (2019) Including intangible costs into the cost-of-illness approach: a method refinement illustrated based on the PM 2.5 economic burden in China. Eur J Health Econ 20(4):501–11. https://doi.org/10.1007/s10198-018-1012-0
Acknowledgements
The results of this study come from a portion of results of a Master’s Thesis in Environmental Health Engineering at Qom University of Medical Sciences. The authors would like to appreciate the Qom Province Environmental Protection Organization for their cooperation throughout the study. The study was approved by the Ethics Committee of Qom University of Medical Sciences (ID: IR.MUQ.REC.1399.196).
Funding
This work was supported by the Deputy of Research and Technology of Qom University of Medical Sciences (grant number: 991265).
Author information
Authors and Affiliations
Contributions
Zahra Safari: data curation, formal analysis, investigation, methodology, resources, software, visualization, roles/writing — original draft. Reza Fouladi-Fard: conceptualization, formal analysis, funding acquisition, methodology, project administration, supervision, validation. Mostafa Vahedian: methodology, writing — review and editing. Mohammad Hasan Mahmoudian: methodology, writing — review and editing. Ahmad Rahbar: methodology, writing — review and editing. Maria Fiore: supervision, validation, writing — review and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the Ethics Committee of Qom University of Medical Sciences (ID: IR.MUQ.REC.1399.196).
Competing interests
The authors declare no competing interests.
Rights and permissions
About this article

Cite this article
Safari, Z., Fouladi-Fard, R., Vahedian, M. et al. Health impact assessment and evaluation of economic costs attributed to PM2.5 air pollution using BenMAP-CE. Int J Biometeorol 66, 1891–1902 (2022). https://doi.org/10.1007/s00484-022-02330-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-022-02330-1