
Abstract
Background
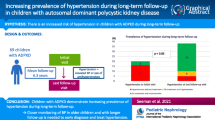
Early detection of hypertension in children with autosomal polycystic kidney disease (ADPKD) may be beneficial, but screening children at risk of ADPKD remains controversial. We investigated determinants of hypertension in children with ADPKD to help identify a subgroup of children at risk of ADPKD for whom screening for the disease and/or its complications would be more relevant.
Methods
In a retrospective study including consecutive children with ADPKD aged 5–18 years and followed at Saint-Luc Hospital Brussels between 2006 and 2020, we investigated the potential association between genotype, clinical characteristics and parental phenotype, and presence of hypertension. Hypertension was defined as blood pressure > P95 during 24-h ambulatory monitoring or anti-hypertensive therapy use. Parental phenotype was considered severe based on age at kidney failure, Mayo Clinic Imaging Classification and rate of eGFR decline.
Results
The study enrolled 55 children with ADPKD (mean age 9.9 ± 2.2 years, 45% male), including 44 with a PKD1 mutation and 5 with no mutation identified. Nine (16%) children had hypertension. Hypertension in children was associated with parental phenotype severity (8/27 (30%) children with severe parental phenotype vs. 1/23 (4%) children with non-severe parental phenotype (p = 0.03)) and height-adjusted bilateral nephromegaly (6/9 (67%) children with bilateral nephromegaly vs. 3/44 (7%) children without bilateral nephromegaly (p < 0.001)).
Conclusions
Severe parental phenotype is associated with higher prevalence of hypertension in children with ADPKD. Hence, children of parents with severe ADPKD phenotype may be those who will most benefit from screening of the disease and/or yearly BP measures.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information


Similar content being viewed by others


References
Torres VE, Harris PC, Pirson Y (2007) Autosomal dominant polycystic kidney disease. Lancet 369:1287–1301. https://doi.org/10.1016/S0140-6736(07)60601-1
Chebib FT, Torres VE (2016) Autosomal dominant polycystic kidney disease: Core Curriculum 2016. Am J Kidney Dis 67:792–810. https://doi.org/10.1053/j.ajkd.2015.07.037
Cornec-Le Gall E, Torres VE, Harris PC (2018) Genetic complexity of autosomal dominant polycystic kidney and liver diseases. J Am Soc Nephrol 29:13–23. https://doi.org/10.1681/ASN.2017050483
Cornec-Le Gall E, Alam A, Perrone RD (2019) Autosomal dominant polycystic kidney disease. Lancet 393:919–935. https://doi.org/10.1016/S0140-6736(18)32782-X
Besse W, Chang AR, Luo JZ, Triffo WJ et al (2019) ALG9 mutation carriers develop kidney and liver cysts. J Am Soc Nephrol 30:2091–2102. https://doi.org/10.1681/ASN.2019030298
Senum SR, Li YSM, Benson KA, Joli G et al (2022) Monoallelic IFT140 pathogenic variants are an important cause of the autosomal dominant polycystic kidney-spectrum phenotype. Am J Hum Genet 109:136–156. https://doi.org/10.1016/j.ajhg.2021.11.016
Cornec-Le Gall E, Audrézet MP, Chen JM, Hourmant M et al (2013) Type of PKD1 mutation influences renal outcome in ADPKD. J Am Soc Nephrol 24:1006–1013. https://doi.org/10.1681/ASN.2012070650
Ho TA, Godefroid N, Gruzon D, Haymann JP et al (2012) Autosomal dominant polycystic kidney disease is associated with central and nephrogenic defects in osmoregulation. Kidney Int 82:1121–1129. https://doi.org/10.1038/ki.2012.225
Selistre L, de Souza V, Ranchin B, Hadj-Aissa A, Cochat P, Dubourg L (2012) Early renal abnormalities in children with postnatally diagnosed autosomal dominant polycystic kidney disease. Pediatr Nephrol 27:1589–1593. https://doi.org/10.1007/s00467-012-2192-y
Cadnapaphornchai MA (2015) Autosomal dominant polycystic kidney disease in children. Curr Opin Pediatr 27:193–200. https://doi.org/10.1097/MOP.0000000000000195
Marlais M, Cuthell O, Langan D, Dudley J, Sinha MD, Winyard PJ (2016) Hypertension in autosomal dominant polycystic kidney disease: a meta-analysis. Arch Dis Child 101:1142–1147. https://doi.org/10.1136/archdischild-2015-310221
Reddy BV, Chapman AB (2017) The spectrum of autosomal dominant polycystic kidney disease in children and adolescents. Pediatr Nephrol 32:31–42. https://doi.org/10.1007/s00467-016-3364-y
Gimpel C, Bergmann C, Mekahli D (2021) The wind of change in the management of autosomal dominant polycystic kidney disease in childhood. Pediatr Nephrol 37:473–487. https://doi.org/10.1007/s00467-021-04974-4
Massella L, Mekahli D, Paripović D, Prikhodina L et al (2018) Prevalence of hypertension in children with early-stage ADPKD. Clin J Am Soc Nephrol 13:874–883. https://doi.org/10.2215/CJN.11401017
Marlais M, Rajalingam S, Gu H, Savis A, Sinha MD, Winyard PJ (2019) Central blood pressure and measures of early vascular disease in children with ADPKD. Pediatr Nephrol 34:1791–1797. https://doi.org/10.1007/s00467-019-04287-7
Fick-Brosnahan GM, Tran ZV, Johnson AM, Strain JD, Gabow PA (2001) Progression of autosomal-dominant polycystic kidney disease in children. Kidney Int 59:1654–1662. https://doi.org/10.1046/j.1523-1755.2001.0590051654
Cadnapaphornchai MA, McFann K, Strain JD, Masoumi A, Schrier RW (2008) Increased left ventricular mass in children with autosomal dominant polycystic kidney disease and borderline hypertension. Kidney Int 74:1192–1196. https://doi.org/10.1038/ki.2008.397
Cadnapaphornchai MA, McFann K, Strain JD, Masoumi A, Schrier RW (2009) Prospective change in renal volume and function in children with ADPKD. Clin J Am Soc Nephrol 4:820–829. https://doi.org/10.2215/CJN.02810608
Cadnapaphornchai MA, Masoumi A, Strain JD, McFann K, Schrier RW (2011) Magnetic resonance imaging of kidney and cyst volume in children with ADPKD. Clin J Am Soc Nephrol 6:369–376. https://doi.org/10.2215/CJN.03780410
Chapman AB, Guay-Woodford LM (2009) Renal volume in children with ADPKD: size matters. Clin J Am Soc Nephrol 4:698–699. https://doi.org/10.2215/CJN.01410209
Gimpel C, Bergmann C, Bockenhauer D, Breysem L et al (2019) International consensus statement on the diagnosis and management of autosomal dominant polycystic kidney disease in children and young people. Nat Rev Nephrol 15:713–726. https://doi.org/10.1038/s41581-019-0155-2
Chapman AB, Devuyst O, Eckardt KU, Gansevoort RT et al (2015) Autosomal-dominant polycystic kidney disease (ADPKD): executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 88:17–27. https://doi.org/10.1038/ki.2015.59
Lurbe E, Agabiti-Rosei E, Cruickshank JK, Dominiczak A et al (2016) European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens 34:1887–1920. https://doi.org/10.1097/HJH.0000000000001039
Gao A, Cachat F, Faouzi M, Bardy D, Mosig D, Meyrat BJ, Girardin E, Chehade H (2013) Comparison of the glomerular filtration rate in children by the new revised Schwartz formula and a new generalized formula. Kidney Int 83:524–530. https://doi.org/10.1038/ki.2012.388
Obrycki L, Sarnecki J, Lichosik M, Sopińska M et al (2022) Kidney length normative values in children aged 0–19 years – a multicenter study. Pediatr Nephrol 37:1075–1085. https://doi.org/10.1007/s00467-021-05303-5
Richards S, Aziz N, Bale S, Bick D et al (2015) Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med 17:405–424. https://doi.org/10.1038/gim.2015.30
Irazabal MV, Rangel LJ, Bergstralh EJ, Osborn SL et al (2015) Imaging classification of autosomal dominant polycystic kidney disease: a simple model for selecting patients for clinical trials. J Am Soc Nephrol 26:160–172. https://doi.org/10.1681/ASN.2013101138
Lanktree MB, Guiard E, Li W, Akbari P et al (2019) Intrafamilial variability of ADPKD. Kidney Int Rep 4:995–1003. https://doi.org/10.1016/j.ekir.2019.04.018
Barua M, Cil O, Paterson AD, Wang K, He N, Dicks E, Parfrey P, Pei Y (2009) Family history of renal disease severity predicts the mutated gene in ADPKD. J Am Soc Nephrol 20:1833–1838. https://doi.org/10.1681/ASN.2009020162
Schrier RW, Brosnahan G, Cadnapaphornchai MA, Chonchol M, Friend K, Gitomer B, Rossetti S (2014) Predictors of autosomal polycystic kidney disease progression. J Am Soc Nephrol 25:2399–2418. https://doi.org/10.1681/ASN.2013111184
Song P, Zhang Y, Yu J, Zha M, Zhu Y, Rahimi K, Rudan I (2019) Global prevalence of hypertension in children: a systematic review and meta-analysis. JAMA Pediatr 173:1154–1163. https://doi.org/10.1001/jamapediatrics.2019.3310
De Rechter S, Bammens B, Schaefer F, Liebau MC, Mekahli D (2018) Unmet needs and challenges for follow-up and treatment of autosomal dominant polycystic kidney disease: the paediatric perspective. Clin Kidney J 11(Suppl 1):i14–i26. https://doi.org/10.1093/ckj/sfy088
Breysem L, De Rechter S, De Keyzer F, Smet MH et al (2018) 3DUS as an alternative to MRI for measuring renal volume in children with autosomal dominant polycystic kidney disease. Pediatr Nephrol 33:827–835. https://doi.org/10.1007/s00467-017-3862-6
Heyer CM, Sundsbak JL, Abebe KZ, Chapman AB et al (2016) Predicted mutation strength of nontruncating PKD1 mutations aids genotype-phenotype correlations in autosomal dominant polycystic kidney disease. J Am Soc Nephrol 27:2872–2884. https://doi.org/10.1681/ASN.2015050583
Levin A, Stevens PE, Bilous RW, Coresh J et al (2013) KDIGO 2012 Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 3:1–150. https://doi.org/10.1038/kisup.2012.73
Pottel H, Björk J, Delanaye P, Nyman U (2022) Evaluation of the creatinine-based chronic kidney disease in children (under 25 years) equation in healthy children and adolescents. Pediatr Nephrol 37:2213–2216. https://doi.org/10.1007/s00467-022-05429-0
Acknowledgements
We wish to thank O. Devuyst and Y. Pirson for their constructive advice and review of the manuscript, as well as P. Harris and SR Senum for their help in the categorization of the PKD1 variants.
Six of the authors of this publication are members of the European Reference Network for Rare Kidney Diseases (ERKNet).
Funding
This study was supported by a private grant (“Prix Marlène et Philippe Cloës”), and an unrestricted educational grant from Otsuka Pharmaceuticals (Nathalie Demoulin).
Author information
Authors and Affiliations
Contributions
All the authors contributed to the design of the study and review of the manuscript. ND, EVR, and NG wrote the manuscript. JM performed the statistical analysis.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Demoulin, N., Van Regemorter, E., Dahan, K. et al. Severe parental phenotype associates with hypertension in children with ADPKD. Pediatr Nephrol 38, 2733–2740 (2023). https://doi.org/10.1007/s00467-022-05870-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05870-1