
Abstract
Background
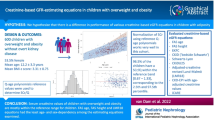
The current childhood obesity pandemic is likely to result in an increased risk of chronic kidney disease (CKD) later in life. Correlations between obesity-related comorbidities and kidney function can be found, but it is unclear to what extent this is caused by bias due to different mathematical forms of the estimated glomerular filtration rate (eGFR) equations. The present study aimed to analyze correlations between obesity-related comorbidities and different eGFR equations and to investigate whether rescaled serum creatinine (SCr/Q) for sex and age or height might be an alternative biomarker for kidney function estimation.
Methods
This cross-sectional cohort study included 600 children with overweight and obesity. Mean age was 12.20 ± 3.28 years, 53.5% were female, and mean BMI z-score was 3.31 ± 0.75. All children underwent a comprehensive assessment that included anthropometrical and blood pressure measurements, laboratory examination, air displacement plethysmography, and polysomnography. Qage and Qheight polynomials were used to rescale SCr and multiple creatinine-based eGFR equations were compared.
Results
SCr/Q and almost all GFR estimations significantly correlated with a waist-to-hip ratio, fat mass, homeostasis model assessment for insulin resistance, and triacylglyceride, HDL cholesterol, alanine transaminase, and serum uric acid concentrations. Multiple correlations, however, were not confirmed by all equations, which suggests dependency on the mathematical form of the different eGFR equations.
Conclusions
Correlations between obesity-related comorbidities and creatinine-based eGFR are present in children with overweight and obesity, but depend to a large extent on the eGFR equation of choice. SCr/Q might be an alternative biomarker for assessing correlations between obesity-related comorbidities and kidney function in children with overweight and obesity.
Graphical Abstract

A higher resolution version of the Graphical abstract is available as Supplementary information
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The global prevalence of children with overweight and obesity has dramatically increased during the last few decades [1]. Obesity during childhood increases the risk of developing various comorbidities, including diabetes mellitus, hypertension, and dyslipidemia [2]. Additionally, children with obesity are prone to become adults with obesity, increasing the lifetime health risk even more [3]. With the first report that dates from 1974 describing an association between severe obesity and nephrotic-range proteinuria [4], nowadays, the relation between obesity and chronic kidney disease (CKD) is widely accepted [5,6,7]. Apart from the separate entity called obesity-related glomerulopathy, pathologically defined as glomerular hypertrophy and adaptive focal segmental glomerulosclerosis, obesity is an important prognostic factor for an adverse kidney outcome in patients with a solitary functioning kidney, IgA nephropathy, and autosomal dominant polycystic disease [8,9,10]. Obesity, therefore, plays a major role in the increasing prevalence of CKD, a condition that already afflicts 10% of the population worldwide [11].
The current pandemic of childhood obesity is likely to result in an increased risk of CKD in later life, as early-life adiposity is associated with CKD in the long term [12,13,14]. Unfortunately, kidney injury due to obesity might go unnoticed for years, hence named a “silent” comorbidity of obesity, with a consequence of delayed diagnosis and, therefore, impaired kidney prognosis.
Although the pathophysiology of obesity-related kidney injury is not fully understood, there seems to be a major role of glomerular hyperfiltration, increased activity of the renin-angiotensin-aldosterone system, insulin resistance, and lipid accumulation in the kidney [6, 7]. Since these alterations in the kidney occur before kidney dysfunction or the detection of microalbuminuria or hypertension [15], these markers might not be useful in the early phase of obesity-related kidney injury, and so there is need for other biomarkers. In children with obesity, urinary concentrations of neutrophil gelatinase-associated lipocalcin (NGAL) and kidney injury molecule-1 (KIM-1), both markers for proximal tubular cell injury, might be used for the early diagnosis of kidney injury [16]. In adolescents with obesity with a cystatin C-based glomerular filtration rate (GFR) ≤ 130 ml/min/1.73 m2, increased urinary NGAL concentrations might predict CKD [17]. Since these biomarkers are not (yet) implemented in clinical practice, most clinical studies on childhood obesity and kidney function use creatinine-based estimated glomerular filtration rate (eGFR) and (micro)albuminuria as markers for kidney health [13]. However, eGFR is almost always preserved in children with overweight and obesity without a history of kidney disease [18, 19], and microalbuminuria has a prevalence that ranges from 0.3 to 7.9%, which in fact is not different from the prevalence in lean children [20]. Clinical studies examining associations between obesity-related comorbidities and kidney function in childhood have yielded inconsistent results [13]. Important to consider is that eGFR equations using endogenous filtration markers are suffering from inaccuracy and imprecision [21], and not all creatinine-based GFR-estimating equations seem suitable for children with overweight and obesity [19]. Considering all of this, GFR-estimating equations might be inappropriate for evaluating correlations between kidney function and “metabolic health” in children with overweight and obesity. We postulate that the discrepant results in other studies examining associations between childhood obesity and kidney disease might be partially caused by bias and random error in eGFR equations. Therefore, in this study on children with overweight and obesity without overt kidney disease, we will compare different creatinine-based GFR-estimating equations and their correlations with anthropometric variables and obesity-related comorbidities. Additionally, we will examine whether rescaled SCr for sex and age or height might be used as an alternative marker.
Methods
Study population
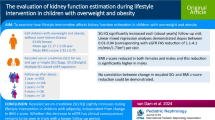
This study uses baseline, pre-intervention data from the Centre of Overweight Adolescent and Children’s Healthcare (COACH): a clinical multidisciplinary lifestyle intervention program at the Maastricht University Medical Centre + (MUMC+). In this program, children with overweight, obesity, and severe obesity are evaluated to identify the underlying cause of the adiposity and potential obesity-related comorbidities, as described previously [19,20,21,22]. Between January 1, 2011, and April 1, 2019, 662 children entered the COACH program. Exclusion criteria for this study were age ≥ 18 years (n = 5), normal weight (at the moment of the measurements in our center (n = 5)), secondary cause of adiposity, known kidney disease (congenital or acquired), diabetes mellitus, and/or use of antihypertensive medication (n = 13). Serum creatinine (SCr) was not measured in 39 children. All other children (n = 600) were included in this study. The Medical Ethical Committee of the MUMC+ approved this study and informed consent was obtained.
Clinical assessment, anthropometry, and body composition
After entering the COACH program, children were admitted for approximately 24 hours in the pediatric department of the MUMC+ for clinical evaluation. While children wore only underwear, weight and height were determined using a digital scale (Seca, Chino, CA) and stadiometer (De Grood Metaaltechniek, Nijmegen, the Netherlands), respectively. Weight and height were used to calculate body mass index (BMI) and BMI was converted into z-scores. Definitions from the International Obesity Task Force (IOTF) were used to define overweight, obesity, and severe obesity [23]. Waist and hip circumferences were determined, waist-to-hip ratio was calculated, and waist and hip circumference z-scores were obtained using reference values [24]. The equation described by Haycock et al. was used to calculate body surface area (BSA) [25]. In a subgroup of randomly chosen children (n = 285), fat mass and fat-free mass were determined by air displacement plethysmography (BodPod).
Creatinine-based eGFR equations and microalbuminuria
Serum creatinine (SCr) was measured enzymatically (Cobas 8000, Roche). Since SCr is heavily dependent on sex, age, and height [26, 27], SCr was rescaled using Qage and Qheight polynomials obtained from the literature [28, 29]. SCr/Q (“rescaled SCr”) is sex and age or height independent for healthy subjects, depending on whether Qage or Qheight is used. In a previous study, it was concluded that this concept of rescaling SCr works very well in children with overweight and obesity [19]. Rescaled SCr was evaluated using the reference band [0.67–1.33], which represents the 2.5th and 97.5th percentiles [30]. The following SCr-based eGFR equations were evaluated, as described previously [19]: FAS-age [28]; FAS-height [29]; EKFC [31]; updated bedside Schwartz [32]; Schwartz-Lyon [33]; CKiDU25 [34]; LMR18 [35]; and CKD-EPI40 [36]. Urinary albumin was determined in a random urine spot and the urine albumin-to-creatinine ratio (UACR) was calculated. Microalbuminuria was present when the UACR was between 30 and 300 mg/mg.
Laboratory analyses
Venous blood samples were collected while children were in a fasting state. Fasting plasma glucose, serum uric acid, total cholesterol, high-density lipoprotein (HDL) cholesterol, triacylglyceride, and alanine transaminase (ALT) concentrations were measured (Cobas 8000 modular analyzer, Roche). Serum insulin concentrations were analyzed (Immulite-1000, Siemens Healthcare Diagnostics). The Friedewald equation was used to calculate low-density lipoprotein (LDL) cholesterol concentrations [37]. Glycated hemoglobin (HbA1c) concentrations were measured (fully automated HPLC Variant II, Bio-Rad Laboratories). In order to estimate the presence of insulin resistance, the homeostasis model assessment for insulin resistance (HOMA-IR) was calculated from fasting glucose and insulin concentrations in which \(\text{HOMA}-\text{IR}=\frac{\mathrm f\mathrm a\mathrm s\mathrm t\mathrm i\mathrm n\mathrm g\;\mathrm g\mathrm l\mathrm u\mathrm c\mathrm o\mathrm s\mathrm e\left(\frac{\mathrm{mmol}}{\mathrm l}\right)\times\mathrm f\mathrm a\mathrm s\mathrm t\mathrm i\mathrm n\mathrm g\;\mathrm i\mathrm n\mathrm s\mathrm u\mathrm l\mathrm i\mathrm n(\frac{\mathrm{mU}}{\mathrm l})}{22.5}\) [38].
Blood pressure
Blood pressure (BP) was measured during daytime, every 3 min for about 20 times, depending on the tolerability of the child (Mobil-O-Graph, I.E.M. GmbH, Stolberg, Germany). Mean systolic BP (SBP) and diastolic (DBP) were calculated and converted into percentiles using normative pediatric BP tables [39].
Polysomnography
All participants received a full polysomnography, and definitions of apnea and hypopnea were used as described in the appropriate manual [40]. The apnea-hypopnea index (AHI) was calculated out of the average number of apneas and hypopneas per hour of total sleep time. The oxygen desaturation index (ODI) was calculated as the total of desaturations ≥ 3% per hour.
Statistical analysis
Normally distributed data are presented as mean ± standard deviation, median (interquartile range) otherwise. In the case of normally distributed data, Pearson’s correlation coefficient was used, Spearman’s correlation coefficient otherwise. A P-value below 0.05 was considered statistically significant, and all P-values are two-tailed. No correction was performed for multiple testing and P-values should be considered accordingly. The high sample size (n = 600) in this study may be responsible for turning clinically insignificant correlations into statistically significant correlations. As a rule of thumb, we here consider correlations < 0.200 as negligible from a clinical point of view. Statistical analysis was performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Clinical Trial registration: (ClinicalTrial.gov; Registration Number: NCT02091544).
Results
Characteristics
In Table 1, anthropometrical and metabolic characteristics of the 600 included children are presented, stratified according to sex. Mean age was 12.20 ± 3.28 years (ranged from 2.61 to 17.88 years) and there were slightly more females compared to males. Mean BMI z-score was 3.31 ± 0.75 and 21.3% of the children were in the overweight category, and 44.7% and 34.0% in the obese and severe obese categories, respectively. In both sexes, mean BSA was about 1.78 m2, and the body composed of approximately 44% fat mass. Compared to females, males had a significant higher BMI z-score, hip circumference z-score, waist-to-hip ratio, fasting glucose and alanine transaminase (ALT) concentration, and apnea-hypopnea index (AHI) and oxygen desaturation index (ODI). A total of 94.7% and 96.5% of the children had SCr/Qheight and SCr/Qage within the [0.67–1.33] reference interval, respectively. On the other hand, the concentration of fasting insulin was significantly higher in females, and for triacylglyceride and LDL cholesterol concentration, there was a trend towards higher values in females compared to males.
As shown in Table 2, mean and median eGFR were 98.4–115.8 ml/min/1.73 m2 and 98.1–113.7 ml/min/1.73 m2 using the different creatinine-based GFR-estimating equations, respectively. Moreover, equations differed concerning 2.5th and 97.5th percentiles and range (minimum and maximum).
In Supplementary Information Tables S1 and S2, anthropometrical and metabolic variables are compared between children with SCr/Qage and SCr/Qheight within the [0.67–1.33] reference range and values below 0.67 and above 1.33. As shown, groups are small and no multiple testing correction was performed, so the significance of the differences between the groups should be interpreted with caution.
Correlation analyses
As presented in Table 3, SCr is correlated with age, weight, height, body surface area (BSA), fat mass, waist and hip circumference z-score, and waist-to-hip ratio. In children between the ages of 2 and 14 years, however, SCr linearly increases with age with no differences between males and females. From the age of 14 years, SCr begins to differ between sexes and ends on a plateau value of 0.70 mg/dl for adult females and 0.90 mg/dl for adult males. Since it is clear that SCr correlates with age and sex, SCr was rescaled using Qage polynomials. Moreover, we rescaled SCr using Qheight polynomials as well. Correlations between SCr and age, weight, height, BSA, and hip circumference z-score disappear when SCr is rescaled using Qage. SCr/Qheight however is still correlated with weight, height, and BSA. Correlations between SCr/Q (both Qage and Qheight) and fat mass are becoming more pronounced, and there is still a correlation with waist circumference z-score and waist-to-hip ratio. SCr/Qheight was weakly inversely correlated with BMI z-score (r = − 0.109, P = 0.007). SCr and SCr/Qage did not correlate with BMI z-score. All eGFR equations correlated with fat mass and waist-to-hip ratio, whereas for the other anthropometric variables, there was no consistency in correlations with eGFR.
In Table 4, correlations are shown between SCr, SCr/Q, and different creatinine-based eGFR equations and metabolic parameters. SCr/Qage and nearly all eGFR equations correlated with HOMA-IR and HDL cholesterol, triacylglyceride, serum uric acid, and ALT concentrations. Results are similar for SCr/Qheight with a few exceptions. Apart from this, there is a major inconsistency between eGFR equations and (weak) correlations with metabolic variables.
Discussion
In this study, we evaluated correlations between serum creatinine (SCr), rescaled SCr (SCr/Q), and different creatinine-based eGFR-estimating equations with anthropometric and metabolic variables in 600 children with overweight and obesity without overt kidney disease. SCr/Q height correlated with BMI z-score, whereas SCr and SCr/Qage did not. We verified the correlation between SCr and fat mass (and thus fat-free (lean) mass) [41], and this positive correlation becomes even more pronounced after rescaling SCr using Qage and Qheight polynomials. Moreover, we showed that all examined creatinine-based eGFR equations were positively correlated with fat mass and waist-to-hip ratio. Rescaled SCr and nearly all eGFR equations correlated with HOMA-IR and HDL cholesterol, triacylglyceride, serum uric acid, and ALT concentrations. Apart from this, there is a major inconsistency between eGFR equations and (weak) correlations with other metabolic variables. Based on this study, it is clear that the choice of a creatinine-based eGFR equation has an enormous impact on possible correlations with anthropometric variables and metabolic risk factors.
Obesity and excessive visceral fat are well-known cardiovascular and metabolic risk factors. The cluster of metabolic, anthropometric, and hemodynamic abnormalities is collectively known as metabolic syndrome. In children, there are at least 40 definitions of metabolic syndrome [42], and these definitions include parameters like waist circumference, triacylglyceride, HDL cholesterol and fasting glucose concentrations, and systolic blood pressure. In this study, we evaluated these and other highly prevalent obesity-related comorbidities such as hypertension, altered glucose metabolism and insulin resistance, dyslipidemia, hyperuricemia, non-alcoholic fatty liver disease (NAFLD), and sleep-disordered breathing. SCr/Q and nearly all eGFR equations correlated with HOMA-IR and HDL cholesterol, triacylglyceride, serum uric acid, and ALT concentrations, all well-known markers for insulin resistance, dyslipidemia, hyperuricemia, and NAFLD, respectively. Our findings therefore support the relation between metabolic syndrome and the kidney in children with overweight and obesity [43].
This study also demonstrates that the choice of a creatinine-based eGFR equation has a tremendous impact on correlations with the examined variables. Important to consider is that not all creatinine-based GFR-estimating equations seem suitable in children with overweight and obesity [19]. Equations with SCr in the denominator (with “1” as a power coefficient) may result in extremely high predictions. This is an artefact of these equations and exactly the reason why the EKFC equation has been developed. In this study, a difference in correlations with age-based and height-based creatinine-based eGFR equations was observed. The CKiD, CKiDU25, and Schwartz-Lyon equations are the only equations that correlate significantly with age. Moreover, the 2.5th percentile is larger than 75 ml/min/1.73 m2 for nearly all equations (except for Schwartz-Lyon and CKD-EPI40) and has previously been considered as the lower limit for GFR in children and adolescents [30]. Finally, the EKFC, LMR18, and CKD-EPI40 equations show a much lower “spread” (standard deviation) than the other equations, mainly because these equations use different power coefficients for SCr in their equation. This also results in much lower 97.5th percentile (and maximum) values.
Most other studies that examine the association between childhood obesity and kidney function use GFR-estimating equations or presence of microalbuminuria as markers for kidney function and body mass index (BMI) as a measure for adiposity [13]. In a recent review [13], 15 such studies were described and these studies found a mix of negative, positive, and no association between eGFR and BMI. In 10 studies, a Schwartz equation (most commonly the bedside Schwartz equation) was used for GFR estimation, and in 9 of these studies, a Schwartz equation was the only equation used. The bedside Schwartz equation, which was developed and validated in growth-retarded children with CKD, shows a significant eGFR decline with age and major differences between adolescent males and females in children with a GFR within the normal range [44]. Because of this, these Schwartz equations should not be used to examine associations between obesity and/or obesity-related comorbidities and kidney function in children without CKD.
All studies included in the review by Jadresic et al. used BMI as a marker for adiposity [13]. While BMI is the most commonly used measure for obesity, it gives no information on body fat content or distribution. Human body mass can be divided into two main compartments: fat mass and lean (fat-free) mass. BMI does not distinguish lean mass from fat mass and it is known that the amount of adiposity correlates with cardiovascular risk factors independent from BMI [45]. Several methods are currently available for body composition assessment, and since field body composition methods (including anthropometrics, skinfolds, bio-electrical impedance analysis, and ultrasound) are still inferior to more sophisticated laboratory body composition methods [46], air displacement plethysmography was used in this study. Fat mass and waist-to-hip ratio, a surrogate marker for visceral fat, were correlated with SCr/Q and all examined creatinine-based GFR-estimating equations. These findings support the unhealthy aspect of visceral adiposity and suggest a relation between central adiposity and kidney function in children with overweight and obesity.
Due to the cross-sectional study design and lack of measured GFR, it is not possible to state which correlations are clinically relevant. However, we suggest that rescaling SCr (either using Qage or Qheight polynomials) can be a valuable add-on next to creatinine-based GFR-estimating equations. Advantages of SCr/Q compared to eGFR equations are:
-
There is no influence of statistical modeling to convert SCr to an eGFR formula
-
There is a clear target value (namely SCr/Q = 1) for a healthy child, independent from age and sex, and a clear reference interval of [0.67–1.33]
-
SCr/Qage (and thus eGFR FAS-age) might be directly added to the serum creatinine result of a patient in the clinical laboratory report, as height is often unavailable in the clinical laboratory. In this manner, interpretation of serum creatinine becomes more convenient for paediatricians
-
Repeated measurements of SCr/Q over time are (probably) not influenced by age, sex, and other factors (like body surface area (BSA))
-
Because SCr/Q is independent of BSA, it may serve as an excellent kidney function marker for longitudinal follow-up of children with overweight or obesity during a lifestyle program
-
SCr/Q correlates with fat mass, waist-to-hip ratio, serum uric acid, and ALT, variables that (almost) all examined eGFR equations are correlated with to more or less the same degree
The question whether childhood obesity is already related to or leads to future kidney disease can obviously not be answered in this cross-sectional study. While there are some examples of prospective studies that address these questions [12, 47,48,49], data on this are scarce. We suggest that future, prospective studies include SCr/Q as a kidney biomarker and compare our findings with measured GFR. Moreover, we suggest to include biomarkers for detection of early kidney damage due to obesity, such as urinary NGAL and KIM-1 [7].
In conclusion, correlations between obesity-related comorbidities and creatinine-based eGFR can be found in children with overweight and obesity, but depend to a large extent on the eGFR equation of choice. SCr/Q is independent of the equation of choice and might be an alternative biomarker for assessing correlations between obesity-related comorbidities and kidney function in children with overweight and obesity.
References
Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, Lee A, Marczak L, Mokdad AH, Moradi-Lakeh M, Naghavi M, Salama JS, Vos T, Abate KH, Abbafati C, Ahmed MB, Al-Aly Z, Alkerwi A, Al-Raddadi R, Amare AT, Amberbir A, Amegah AK, Amini E, Amrock SM, Anjana RM, Ärnlöv J, Asayesh H, Banerjee A, Barac A, Baye E, Bennett DA, Beyene AS, Biadgilign S, Biryukov S, Bjertness E, Boneya DJ, Campos-Nonato I, Carrero JJ, Cecilio P, Cercy K, Ciobanu LG, Cornaby L, Damtew SA, Dandona L, Dandona R, Dharmaratne SD, Duncan BB, Eshrati B, Esteghamati A, Feigin VL, Fernandes JC, Fürst T, Gebrehiwot TT, Gold A, Gona PN, Goto A, Habtewold TD, Hadush KT, Hafezi-Nejad N, Hay SI, Horino M, Islami F, Kamal R, Kasaeian A, Katikireddi SV, Kengne AP, Kesavachandran CN, Khader YS, Khang YH, Khubchandani J, Kim D, Kim YJ, Kinfu Y, Kosen S, Ku T, Defo BK, Kumar GA, Larson HJ, Leinsalu M, Liang X, Lim SS, Liu P, Lopez AD, Lozano R, Majeed A, Malekzadeh R, Malta DC, Mazidi M, McAlinden C, McGarvey ST, Mengistu DT, Mensah GA, Mensink GBM, Mezgebe HB, Mirrakhimov EM, Mueller UO, Noubiap JJ, Obermeyer CM, Ogbo FA, Owolabi MO, Patton GC, Pourmalek F, Qorbani M, Rafay A, Rai RK, Ranabhat CL, Reinig N, Safiri S, Salomon JA, Sanabria JR, Santos IS, Sartorius B, Sawhney M, Schmidhuber J, Schutte AE, Schmidt MI, Sepanlou SG, Shamsizadeh M, Sheikhbahaei S, Shin MJ, Shiri R, Shiue I, Roba HS, Silva DAS, Silverberg JI, Singh JA, Stranges S, Swaminathan S, Tabarés-Seisdedos R, Tadese F, Tedla BA, Tegegne BS, Terkawi AS, Thakur JS, Tonelli M, Topor-Madry R, Tyrovolas S, Ukwaja KN, Uthman OA, Vaezghasemi M, Vasankari T, Vlassov VV, Vollset SE, Weiderpass E, Werdecker A, Wesana J, Westerman R, Yano Y, Yonemoto N, Yonga G, Zaidi Z, Zenebe ZM, Zipkin B, Murray CJL (2017) Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med 377:13–27
Skinner AC, Perrin EM, Moss LA, Skelton JA (2015) Cardiometabolic risks and severity of obesity in children and young adults. N Engl J Med 373:1307–1317
Juhola J, Magnussen CG, Viikari JS, Kähönen M, Hutri-Kähönen N, Jula A, Lehtimäki T, Åkerblom HK, Pietikäinen M, Laitinen T, Jokinen E, Taittonen L, Raitakari OT, Juonala M (2011) Tracking of serum lipid levels, blood pressure, and body mass index from childhood to adulthood: the cardiovascular risk in young Finns study. J Pediatr 159:584–590
Weisinger JR, Kempson RL, Eldridge FL, Swenson RS (1974) The nephrotic syndrome: a complication of massive obesity. Ann Intern Med 81:440–447
Ejerblad E, Fored CM, Lindblad P, Fryzek J, McLaughlin JK, Nyrén O (2006) Obesity and risk for chronic renal failure. J Am Soc Nephrol 17:1695–1702
D’Agati VD, Chagnac A, de Vries AP, Levi M, Porrini E, Herman-Edelstein M, Praga M (2016) Obesity-related glomerulopathy: clinical and pathologic characteristics and pathogenesis. Nat Rev Nephrol 12:453–471
Martínez-Montoro JI, Morales E, Cornejo-Pareja I, Tinahones FJ, Fernández-García JC (2022) Obesity-related glomerulopathy: current approaches and future perspectives. Obes Rev 23:e13450
La Scola C, Guarino S, Pasini A, Capalbo D, Liguori L, Di Sessa A, Bertulli C, Mencarelli F, De Mutiis C, Campana G, La Manna A, Miraglia Del Giudice E, Pession A, Marzuillo P (2020) Effect of body mass index on estimated glomerular filtration rate levels in children with congenital solitary kidney: a cross-sectional multicenter study. J Ren Nutr 30:261–267
Bonnet F, Deprele C, Sassolas A, Moulin P, Alamartine E, Berthezène F, Berthoux F (2001) Excessive body weight as a new independent risk factor for clinical and pathological progression in primary IgA nephritis. Am J Kidney Dis 37:720–727
Nowak KL, You Z, Gitomer B, Brosnahan G, Torres VE, Chapman AB, Perrone RD, Steinman TI, Abebe KZ, Rahbari-Oskoui FF, Yu ASL, Harris PC, Bae KT, Hogan M, Miskulin D, Chonchol M (2018) Overweight and obesity are predictors of progression in early autosomal dominant polycystic kidney disease. J Am Soc Nephrol 29:571–578
GBD Chronic Kidney Disease Collaboration (2020) Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet 395:709–733
Silverwood RJ, Pierce M, Hardy R, Thomas C, Ferro C, Savage C, Sattar N, Kuh D, Nitsch D (2013) Early-life overweight trajectory and CKD in the 1946 British birth cohort study. Am J Kidney Dis 62:276–284
Jadresic L, Silverwood RJ, Kinra S, Nitsch D (2019) Can childhood obesity influence later chronic kidney disease? Pediatr Nephrol 34:2457–2477
Stern-Zimmer M, Calderon-Margalit R, Skorecki K, Vivante A (2021) Childhood risk factors for adulthood chronic kidney disease. Pediatr Nephrol 36:1387–1396
Serra A, Romero R, Lopez D, Navarro M, Esteve A, Perez N, Alastrue A, Ariza A (2008) Renal injury in the extremely obese patients with normal renal function. Kidney Int 73:947–955
Goknar N, Oktem F, Ozgen IT, Torun E, Kuçukkoc M, Demir AD, Cesur Y (2015) Determination of early urinary renal injury markers in obese children. Pediatr Nephrol 30:139–144
Mackowiak-Lewandowicz K, Ostalska-Nowicka D, Zaorska K, Kaczmarek E, Zachwieja J, Witt M, Nowicki M (2022) Chronic kidney disease predictors in obese adolescents. Pediatr Nephrol 37:2479–2488
Ding W, Mak RH (2015) Early markers of obesity-related renal injury in childhood. Pediatr Nephrol 30:1–4
van Dam MJCM, Pottel H, Vreugdenhil ACE (2022) Creatinine-based GFR-estimating equations in children with overweight and obesity. Pediatr Nephrol 37:2393–2403
Tsioufis C, Mazaraki A, Dimitriadis K, Stefanidis CJ, Stefanadis C (2011) Microalbuminuria in the paediatric age: current knowledge and emerging questions. Acta Paediatr 100:1180–1184
den Bakker E, Gemke R, Bokenkamp A (2018) Endogenous markers for kidney function in children: a review. Crit Rev Clin Lab Sci 55:163–183
van Dam M, Rijks J, Dorenbos E, Horuz F, van Dael K, Vreugdenhil A (2019) The effect of one year lifestyle intervention on eGFR in children and adolescents with overweight, obesity and morbid obesity. Sci Rep 9:4504
Cole TJ, Lobstein T (2012) Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes 7:284–294
Fredriks AM, van Buuren S, Fekkes M, Verloove-Vanhorick SP, Wit JM (2005) Are age references for waist circumference, hip circumference and waist-hip ratio in Dutch children useful in clinical practice? Eur J Pediatr 164:216–222
Haycock GB, Schwartz GJ, Wisotsky DH (1978) Geometric method for measuring body surface area: a height-weight formula validated in infants, children, and adults. J Pediatr 93:62–66
Pottel H, Vrydags N, Mahieu B, Vandewynckele E, Croes K, Martens F (2008) Establishing age/sex related serum creatinine reference intervals from hospital laboratory data based on different statistical methods. Clin Chim Acta 396:49–55
Ceriotti F, Boyd JC, Klein G, Henny J, Queraltó J, Kairisto V, Panteghini M (2008) Reference intervals for serum creatinine concentrations: assessment of available data for global application. Clin Chem 54:559–566
Pottel H, Hoste L, Martens F (2012) A simple height-independent equation for estimating glomerular filtration rate in children. Pediatr Nephrol 27:973–979
Hoste L, Dubourg L, Selistre L, De Souza VC, Ranchin B, Hadj-Aïssa A, Cochat P, Martens F, Pottel H (2014) A new equation to estimate the glomerular filtration rate in children, adolescents and young adults. Nephrol Dial Transplant 29:1082–1091
Pottel H, Hoste L, Delanaye P (2015) Abnormal glomerular filtration rate in children, adolescents and young adults starts below 75 mL/min/1.73 m(2). Pediatr Nephrol 30:821–828
Pottel H, Björk J, Courbebaisse M, Couzi L, Ebert N, Eriksen BO, Dalton RN, Dubourg L, Gaillard F, Garrouste C, Grubb A, Jacquemont L, Hansson M, Kamar N, Lamb EJ, Legendre C, Littmann K, Mariat C, Melsom T, Rostaing L, Rule AD, Schaeffner E, Sundin PO, Turner S, Bökenkamp A, Berg U, Åsling-Monemi K, Selistre L, Åkesson A, Larsson A, Nyman U, Delanaye P (2021) Development and validation of a modified full age spectrum creatinine-based equation to estimate glomerular filtration rate: a cross-sectional analysis of pooled data. Ann Intern Med 174:183–191
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637
De Souza VC, Rabilloud M, Cochat P, Selistre L, Hadj-Aissa A, Kassai B, Ranchin B, Berg U, Herthelius M, Dubourg L (2012) Schwartz formula: is one k-coefficient adequate for all children? PLoS One 7:e53439
Pierce CB, Muñoz A, Ng DK, Warady BA, Furth SL, Schwartz GJ (2021) Age- and sex-dependent clinical equations to estimate glomerular filtration rates in children and young adults with chronic kidney disease. Kidney Int 99:948–956
Björk J, Nyman U, Delanaye P, Grubb A, Larsson A, Vranken L, Åkesson A, Pottel H (2020) A novel method for creatinine adjustment makes the revised Lund-Malmö GFR estimating equation applicable in children. Scand J Clin Lab Invest 80:456–463
Björk J, Nyman U, Larsson A, Delanaye P, Pottel H (2021) Estimation of the glomerular filtration rate in children and young adults by means of the CKD-EPI equation with age-adjusted creatinine values. Kidney Int 99:940–947
Friedewald WT, Levy RI, Fredrickson DS (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18:499–502
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, de Ferranti SD, Dionne JM, Falkner B, Flinn SK, Gidding SS, Goodwin C, Leu MG, Powers ME, Rea C, Samuels J, Simasek M, Thaker VV, Urbina EM (2017) Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140:e20171904
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, Marcus CL, Mehra R, Parthasarathy S, Quan SF, Redline S, Strohl KP, Davidson Ward SL, Tangredi MM (2012) Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med 8:597–619
Baxmann AC, Ahmed MS, Marques NC, Menon VB, Pereira AB, Kirsztajn GM, Heilberg IP (2008) Influence of muscle mass and physical activity on serum and urinary creatinine and serum cystatin C. Clin J Am Soc Nephrol 3:348–354
Ford ES, Li C (2008) Defining the metabolic syndrome in children and adolescents: will the real definition please stand up? J Pediatr 152:160–164
Litwin M, Niemirska A (2014) Metabolic syndrome in children with chronic kidney disease and after renal transplantation. Pediatr Nephrol 29:203–216
Pottel H, Björk J, Delanaye P, Nyman U (2022) Evaluation of the creatinine-based chronic kidney disease in children (under 25 years) equation in healthy children and adolescents. Pediatr Nephrol 37:2213–2216
Gishti O, Gaillard R, Durmus B, Abrahamse M, van der Beek EM, Hofman A, Franco OH, de Jonge LL, Jaddoe VW (2015) BMI, total and abdominal fat distribution, and cardiovascular risk factors in school-age children. Pediatr Res 77:710–718
Orsso CE, Silva MIB, Gonzalez MC, Rubin DA, Heymsfield SB, Prado CM, Haqq AM (2020) Assessment of body composition in pediatric overweight and obesity: a systematic review of the reliability and validity of common techniques. Obes Rev 21:e13041
Vivante A, Golan E, Tzur D, Leiba A, Tirosh A, Skorecki K, Calderon-Margalit R (2012) Body mass index in 1.2 million adolescents and risk for end-stage renal disease. Arch Intern Med 172:1644–1650
Silverwood RJ, Pierce M, Thomas C, Hardy R, Ferro C, Sattar N, Whincup P, Savage C, Kuh D, Nitsch D (2013) Association between younger age when first overweight and increased risk for CKD. J Am Soc Nephrol 24:813–821
Yan Y, Zheng W, Ma Q, Chu C, Hu J, Wang K, Liao Y, Chen C, Yuan Y, Lv Y, Xu X, Wang Y, Mu J (2021) Child-to-adult body mass index trajectories and the risk of subclinical renal damage in middle age. Int J Obes (Lond) 45:1095–1104
Acknowledgements
We are grateful to all participating children and their parents, and to the members of COACH (Centre for Overweight Adolescent and Children’s Healthcare).
The corresponding author confirms that he has had full access to the data in the study and final responsibility for the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
Each author contributed to the study conception and design. Mark J.C.M. van Dam and Hans Pottel performed data collection and analysis. Mark J.C.M. van Dam wrote the first draft of the manuscript. The final manuscript was read and approved by all the authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van Dam, M.J.C.M., Pottel, H. & Vreugdenhil, A.C.E. Relation between obesity-related comorbidities and kidney function estimation in children. Pediatr Nephrol 38, 1867–1876 (2023). https://doi.org/10.1007/s00467-022-05810-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05810-z