
Abstract
Background
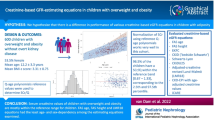
We evaluated the diagnostic performance of height-, age- and body surface area (BSA)-based kidney length (KL) percentiles in the identification of at least one small kidney (KL < 3rd) and in the prediction of reduced estimated glomerular filtration rate (eGFR) and/or elevated blood pressure (BP) in children with and without overweight (OW)/obesity(OB).
Methods
In this cross-sectional study, 744 apparently healthy children (mean age 8.3 years) were recruited in a primary care setting. Clinical data were collected, and serum creatinine and KL were measured. Height-, age- and BSA-based percentiles of KL were calculated and the association of at least one small kidney per subject with reduced eGFR and/or elevated BP was explored by logistic regression.
Results
Two hundred fifty-seven out of seven hundred forty-four (34.5%) subjects were OW/OB and 127 (17.1%) had reduced eGFR or elevated BP. In separate analyses in children with OW/OB, the KL percentiles calculated on the basis of BSA were lower compared with height- and age-based KL percentiles. Consequently, the prevalence of a small kidney was significantly higher when evaluating percentiles of KL based on BSA compared with other percentiles. In logistic regression analysis, a small kidney was significantly associated with reduced eGFR and/or elevated BP only when using height-based KL percentiles. The KL percentiles according to BSA for the ideal weight (iBSA) showed similar performance compared with height-based percentiles. No differences in the diagnostic performance of different percentiles were found in children with normal weight.
Conclusions
BSA-based percentiles underestimate KL in children with OW/OB. In these subjects, the use of height-based or iBSA-based percentiles should be preferred.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It is common practice to normalize kidney length (KL) by body surface area (BSA), based on the Mosteller [1] or Du Bois and Du Bois [2] formulae, using height and weight measurements. However, the kidneys only clear the extracellular water and not the fat mass.
It has been suggested to use ideal body weight to calculate BSA, rather than actual body weight [3], but this is rarely practiced. Since in children and adolescents with overweight (OW) or obesity (OB) the actual weight would lead to a higher BSA than BSA using ideal body weight, we hypothesized that KL percentiles would be underestimated in this group of patients despite the fact that they represent a peculiar category of subjects in whom the size of abdominal organs may increase consistently with their BMI [4,5,6]. Children with OB, in fact, have longer kidneys than their normal weight (NW) counterparts [5]. Normal limits of KL based on height for this group to avoid unnecessary evaluation for nephromegaly have thus been calculated [5].
In view of the OW/OB rates among children and adolescents worldwide with about one-third of children presenting with OW or OB [7, 8], it is important to know the degree of misdiagnosing kidney hypoplasia when the actual weight to calculate BSA is used, because this could lead to unnecessary investigations to rule out chronic kidney disease [9, 10]. We, therefore, conducted a study to identify the most appropriate method to calculate KL percentiles in children with OW/OB. To achieve this aim, we evaluated the diagnostic performance of height-, age- and BSA-based KL percentiles [11] in the identification of at least one small kidney (KL < 3rd) and in the prediction of reduced estimated glomerular filtration rate (eGFR; < 90 mL/min/1.73 m2) and/or elevated BP (> 95th percentile for age and sex). We also estimated the economic and biological costs derived from a potential small kidney misdiagnosis in children and adolescents with OW/OB.
Methods
In this study, 744 apparently healthy school-age children (coming from the general population and without a prior diagnosis of disease) were seen in a primary care setting (primary care centers of Girona and Figueres, both regions in Northeastern Spain) and recruited between 2009 and 2015 in a prospective longitudinal study of obesity and cardiovascular risk factors in children [12, 13].
Children were invited to participate in the study during their routine healthy visits in the primary care centers. These visits are part of the protocol of the Childhood Health Program established by the Catalan Public Health Agency. During the visit, the pediatrician explained the study to the families, and those interested to participate were contacted by the study investigators. Informed written consent was signed by the parents before the enrollment.
Inclusion criteria were the availability of ultrasound of both kidneys and the anthropometrical parameters allowing the calculation of height-, age-, and BSA-based KL percentiles [11].
In case of major known congenital anomalies (abnormal liver, kidney, or thyroid functions), evidence of chronic or acute illness, or prolonged use of medication, the patients were excluded from the study. The study was approved by the Institutional Review Board of Dr. Josep Trueta Hospital and was carried out according to the Declaration of Helsinki.
Assessment of subjects
Subjects were weighed on a calibrated scale and their height was measured with a Harpenden stadiometer with an accuracy of 0.1 cm and 0.05 kg, respectively.
Body-mass index (BMI) was calculated as weight (in kilograms) divided by the square of height (in meters). Age- and sex-adjusted percentiles for BMI were calculated using regional normative data [14]. The study subjects were grouped according to their BMI into normal weight (NW) if BMI was less than 85th percentile, OW if BMI between 85th to less than 95th percentile and OB if BMI was 95th percentile or greater [15]. BSA was calculated as follows: BSA (m2) = square root of [height (cm) × weight (kg)/3600] [1]. Also, ideal BSA (iBSA) was calculated computing into the above-mentioned equation the ideal weight of the subject as follows: iBSA (m2) = square root of [height (cm) × ideal weight (kg)/3600]. The ideal body weight was the weight at the same percentile as the height, for the same age and gender [16].
Systolic and diastolic blood pressures (SBP and DBP) were measured using an electronic sphygmomanometer (Dinamap Pro 100, GE Healthcare, Chalfont St. Giles, UK) after a 10 min rest on the right arm for three consecutive times with the child in the supine position. The average of the two most similar measurements was used in the analysis. Elevated BP was defined by SBP or DBP > 95th percentile for age, height, and gender [17] for this dataset. KL was measured by high-resolution ultrasonography (MyLabTM25, Esaote, Firenze, Italy) as previously reported [13]. The studies were conducted by an experienced pediatric technician using a 3.5–5 MHz convex transducer. KL was measured as the distance between the upper and the lower pole for each kidney on images taken longitudinally. The measures were taken with the child placed in the supine position and the technician situated on the right side of the child. Thereafter, all KL measurements were taken from the right and left flank of the child. Averages of three measurements were used in the study. The intra-observer error of KL measurement was 2.5% and the inter-observer error was 0%, as all ultrasound measurements were performed by the same observer who was unaware of the clinical and laboratory characteristics of the subjects. Intra-subject coefficient of variation for ultrasound measurements was less than 6%. The percentage of coefficient of variation for each sample was calculated in a smaller subset of children (n = 10) as the standard deviation of the 3 independent measurements, divided by the mean and multiplied by 100.
Height-, age- and BSA-based percentiles of both kidneys on the basis of the normative values provided by Obrycki et al. were calculated [11].
Blood samples were obtained in the morning after an overnight fast. Serum creatinine concentrations were routinely assessed in the clinical laboratory of the Hospital using the enzymatic method (COBAS 702, Roche Diagnostics, IN, USA). eGFR was calculated by the pediatric version of the FAS-equation: [eGFR = 107.3/(Scr/Q)] where Q = 0.0270 × Age + 0.232921.
We defined the eGFR as being reduced when it was < 90 mL/min/1.73 m2 [18].
The FAS-equation has previously shown the ability to better select children and adolescents with OW/OB with reduced eGFR and worse cardiometabolic profile [19]. This formula, in fact, eliminates a “potential bias” related to the higher stature of children with OW/OB compared with NW subjects matched for age and gender [19].
Classifications
A kidney with length < 3rd percentile was defined as “small kidney” in this manuscript. Subjects were also classified as having or not OW/OB, reduced eGFR and/or elevated BP as defined above.
Cost analysis
The direct costs that would have been incurred for a misdiagnosis of small kidney by BSA-based percentiles compared with the height-based percentiles were calculated. We used the reimbursement of the Catalan Health System to estimate these costs as follows: blood sample collection (€9.00), creatinine measurement (€0.93), urinalysis (€2.96), nephrological follow-up visit (€80.00), Tc99m DMSA renal scintigraphy (€53.00), and cystography (€139.00) [20].
To calculate the X-ray dose exposure, we used an estimated mean dose of 0.30 mSv for the Tc99m DMSA renal scintigraphy and an estimated mean dose of 1.85 mSv for cystography [21].
Statistical analysis
P values < 0.05 were considered significant. Differences for continuous variables were analyzed with the independent sample t-test for normally distributed variables and with the Mann–Whitney test in case of non-normality. All the data are presented as mean ± standard deviation scores (SDS). Qualitative variables were compared using the chi-squared test.
Univariate and multivariate logistic regression models were used to explore associations with reduced eGFR and/or elevated BP of a small kidney according to height-, age-, and BSA-based percentiles [11]. We computed into the multivariate logistic regression analyses the parameters showing significant differences (p < 0.05) in univariate analysis.
The Stat-Graph XVII software for Windows was used for all statistical analyses except for logistic regression models, which were carried out with SPSS 25 software for Windows.
Results
General characteristics
Participation in the study was 70% out of all invited families. We enrolled 744 children, 395 (53.1% boys), with a mean age of 8.3 years (age range: 3.2–14.8 years). The general characteristics of the enrolled subjects are shown in Table 1. Out of these 744 subjects, 257 (34.5%) were OW/OB and 127 (17.1%) had reduced eGFR or elevated BP. Specifically, four children showed both eGFR reduction and elevated BP, 77 only eGFR reduction and 46 only elevated BP. On the basis of weight status, 41 out of 257 (15.9%) children with OW/OB showed eGFR reduction and/or elevated BP compared with 86 out of 487 (17.6%) children with normal weight (NW) (p = 0.55). Children with OW/OB were older compared with those with NW (9.0 ± 2.0 years vs. 7.9 ± 1.9 years; p < 0.001).
Comparison of performance of height-, age- and BSA-based KL percentiles
When evaluating the global population (including subjects with NW, OW and OB), the KL percentiles calculated on the basis of BSA were significantly lower compared with height- and age-based percentiles. The results were similar for both kidneys (Figs. 1A and B). Moreover, the prevalence of a small kidney was significantly higher when evaluating KL by BSA-based percentiles compared with height- and age-based percentiles (Figs. 2A and B).

Comparison of the kidney length percentiles calculated on the basis of height, age and BSA in all children and in those with overweight/obesity or with normal weight. Abbreviations: BSA, body surface area; OB, obesity; OW, overweight; NW, normal weight

Prevalence of a small kidney comparing height-, age-, and BSA-based percentiles in all children and in those with overweight/obesity or with normal weight. Abbreviations: BSA, body surface area; OB, obesity; OW, overweight; NW, normal weight
Restricting the analysis to the children with OW/OB, for both kidneys, the KL percentiles calculated on the basis of BSA were lower compared with height- and age-based KL percentiles (Figs. 1C and D), and therefore the prevalence of a small kidney was significantly higher when evaluating KL by BSA-based percentiles compared with height- and age-based percentiles (Figs. 2C and D).
When the analysis was limited to the children with NW, the KL percentiles calculated on the basis of height, age and BSA (Figs. 1E and F) and the prevalence of a small kidney on the basis of height, age and BSA percentiles (Figs. 2E and F) were similar for both kidneys.
An exploratory analysis of the prediction of reduced eGFR and/or elevated BP by a small kidney on the basis of height-, age- and BSA-based KL percentile calculations was performed (Table 2). We found that, for the global population and in univariate analysis, a small kidney on the basis of height, age and BSA percentiles was significantly associated with reduced eGFR and/or elevated BP (Table 2). In multivariate analysis, only a small kidney on the basis of height persisted significantly associated with reduced eGFR and/or elevated BP (Table 2). Assessing separately children with OW/OB, a small kidney was significantly associated with reduced eGFR and/or elevated BP only when calculated on the basis of height (Table 2). On the other hand, among subjects with NW, in univariate analysis, a small kidney calculated on the basis of height-, age-, or BSA-derived KL percentiles was significantly associated with reduced eGFR and/or elevated BP (Table 2). None of them persisted as significant in multivariate analysis (Table 2).
Comparison of performance of height-, age- and iBSA-based KL percentiles in children with OW/OB
For both kidneys, the KL percentiles calculated on the basis of iBSA were significantly lower only when compared with age-based percentiles (Figs. 3A and B). The prevalence of a small kidney was similar when evaluating KL by age-based and iBSA-based percentiles (Figs. 3C and D).

Comparison of the right and left kidney length percentiles and prevalence of a small kidney on the basis of height, age, and iBSA percentiles in children with overweight/obesity. Abbreviations: iBSA, ideal body surface area; OB, obesity; OW, overweight; NW, normal weight
In univariate analysis, a small kidney on the basis of both height and iBSA was significantly associated with reduced eGFR and/or elevated BP. None of them persisted as significant in multivariate analysis (Table 3).
Estimate of economic and biological costs derived from a misdiagnosis of a small kidney obtained by BSA-based KL percentiles in children with OW/OB
On the basis of height-based KL percentiles, 18 out of 257 (7%) subjects had a small kidney (three with both small kidneys and 15 with one small kidney). On the basis of age-based KL percentiles 14 out of 247 (5.7%) subjects had a small kidney (three with both small kidneys and 11 with one small kidney). On the basis of BSA-based KL percentiles, 46 out of 257 (17.9%) subjects had a small kidney (16 with both small kidneys and 30 with one small kidney). Because the height-based KL percentiles showed the best diagnostic performance, these percentiles were used as the gold standard in the present analysis. Therefore, compared with height-based percentiles, when using the BSA-based percentiles, 28 out of 257 (10.9%) children received a misdiagnosis of a small kidney with a potential inappropriate indication to undergo further biochemical and instrumental exams.
Considering the performing of blood sample collection with creatinine measurement, urinalysis, nephro-urological visit, Tc99m DMSA renal scintigraphy and cystography for each of these 28 subjects, the cumulative direct economic and biological costs due to small kidney misdiagnosis were respectively 7976.92 € (284.89 € for each patient) and 81.7 mSv (2.15 mSv for each patient, equivalent to 107.5 chest X-rays for each patient).
Discussion
This study investigates the diagnostic performance of BSA-based percentiles of KL compared with height- and age-based percentiles. Our data indicate that the BSA-based percentiles underestimate KL in children and adolescents with OW/OB yielding a misdiagnosis of a small kidney in 11% of these subjects.
A small kidney is associated with reduced eGFR and/or hypertension [9, 22, 23]. This association has been also shown in our population (Table 2). Interestingly, not all percentiles performed similarly in predicting reduced eGFR and/or elevated BP. In the global population, in univariate analysis, a small kidney according to all the percentiles (height-, age- and BSA-based) was significantly associated with reduced eGFR and/or elevated BP. However, in multivariate analysis, only a small kidney calculated on the basis of height-based percentiles showed a significant association with reduced eGFR and/or elevated BP. Similar findings were obtained in children with OW/OB. Moreover, among children with NW, all the percentiles performed equally in the identification of a small kidney. In these subjects, in fact, in univariate analysis, a small kidney calculated on the basis of both height- and age- and BSA-based percentiles was significantly associated with reduced eGFR and/or elevated BP while in multivariate analysis, none of them remained significant.
Usually the right kidney is smaller than the left one [24, 25]; we confirmed this finding also in our pediatric population. In fact, the right KL percentiles both for age, height, BSA and iBSA and both in children with NW and OW/OB were lower compared with the left KL percentile (Fig. 1). Despite this difference, the BSA-based percentiles underestimated the KL of both kidneys compared with other percentiles.
We wish to emphasize that the percentage of subjects showing elevated BP and/or reduced eGFR is quite high (17%) in our study group. This could be explained by the cross-sectional design of the study, with measurement of the parameters only in a 1-day clinical evaluation. In fact, evidence indicates that when repeating the BP measurements in different visits, the percentage of elevated BP significantly decreases from 11.4 to 2.2% [26]. Similarly, one serum creatinine measurement is not sufficient to correctly identify the subjects with reduced eGFR levels because the creatinine measurement is influenced by several factors, such as dietary intake, body composition and muscle mass [27]. Moreover, as stated in the KDIGO chronic kidney disease guidelines, the serum creatinine measurement over a 3-month period is mandatory to correctly identify patients with chronic kidney disease [10].
The presence of a small kidney predicted the presence of reduced eGFR and/or elevated BP in our study group despite the overestimation of the subjects with these conditions. This adds further evidence to the association between small kidney and reduced eGFR and/or elevated BP and reinforces the importance of a correct interpretation of KL using the most appropriate percentiles according to weight status.
Our data indicate that when evaluating children with OW/OB, the most appropriate percentiles are those calculated on the basis of height. This finding is in line with the results of Obrycki et al. [11] who showed — with different methods and starting from a different research question — that the most significant predictor of KL was statural height. Differently from the above-mentioned paper [11], we tested the performance of the different percentiles [11] toward the diagnosis of small kidney after the classification of population in NW and OW/OB. In addition, we showed that in children with OW/OB, as an alternative, also the BSA-based percentiles can be used but it is important to calculate the subject’s BSA on the basis of ideal weight (iBSA). In this manner, a similar performance compared with height-based percentiles could be obtained in the identification of a small kidney. In fact, differences among the percentiles of KL on the basis of iBSA, height, and age were minimal (Fig. 3) and the prevalence of a small kidney was similar when using height- and iBSA-based KL percentiles (Fig. 3). Moreover, height- and iBSA-based KL percentiles performed equally well in the identification of reduced eGFR and/or elevated blood pressure by a small kidney (Table 3).
Correct identification of a small kidney is also important because it can reflect congenital anomalies of the kidney and urinary tract. The current clinical practice relies on performing a Tc99m DMSA renal scintigraphy and cystography in the case of a small kidney [9, 28].
Our cost analysis in case of misdiagnosis of a small kidney using BSA-based percentile to evaluate KL in children with OW/OB indicates both non-negligible economic and biological costs further underlining the importance of a correct selection of KL percentiles to be used in clinical practice in case of children with OW/OB. Moreover, the reduction of X-ray exposure is mandatory in children because evidence exists linking X-ray exposure, especially if occurring early in life, and increased risk of cancer during the life of the subjects [29].
Finally, we wish to emphasize that the prevalence of 34.5% of OW/OB found among Spanish children and adolescents in our study is in line with published data about children and adolescents of the same nation indicating a prevalence of OW/OB of 35.3% [30].
Limitations of our study include the cross-sectional design with the lack of a second collection of parameters within the following 3 months in subjects with elevated BP and/or reduced eGFR and the lack of availability of data regarding proteinuria.
Unfortunately, low agreement between kidney volume and KL has been demonstrated [31,32,33]. As a future perspective, it could be interesting to study the performance of kidney volume to precisely assess kidney size in children and adolescents with OW/OB. In the meantime, when evaluating KL in children with OW/OB, the KL percentiles could be evaluated on the basis of height or iBSA.
In conclusion, our study shows that the BSA-based percentiles can underestimate the KL percentiles when evaluating children with OW/OB. The most appropriate method to evaluate KL percentiles in these subjects is the use of height-based percentiles. Alternatively, also iBSA-based percentiles — by calculating BSA on the basis of ideal weight — can be used with a similar diagnostic performance in the detection of a small kidney and in the identification of subjects with elevated BP and/or reduced eGFR.
Data availability
The dataset generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Mosteller R (1987) Simplified calculation of body-surface area. N Engl J Med 317:1098–1098. https://doi.org/10.1056/NEJM198710223171717
Du Bois D, Du Bois E (1916) A formula to estimate the approximate surface area if height and weight be known. 1916 - PubMed. Arch Intern Med 17:863–871
Livingston EH, Lee S (2001) Body surface area prediction in normal-weight and obese patients. Am J Physiol Endocrinol Metab 281:586–591. https://doi.org/10.1152/AJPENDO.2001.281.3.E586/ASSET/IMAGES/LARGE/H10910507003.JPEG
Lane PH, Belsha CW, Plummer J, Steinhardt GF, Lynch RE, Wood EG (1998) Relationship of renal size, body size, and blood pressure in children. Pediatr Nephrol 12:35–39. https://doi.org/10.1007/S004670050399
Pantoja Zuzuárregui JR, Mallios R, Murphy J (2009) The effect of obesity on kidney length in a healthy pediatric population. Pediatr Nephrol 24:2023–2027. https://doi.org/10.1007/S00467-009-1202-1
Dinkel E, Ertel M, Dittrich M, Peters H, Berres M, Schulte-Wissermann H (1985) Kidney size in childhood sonographical growth charts for kidney length and volume. Pediatr Radiol 15:38–43. https://doi.org/10.1007/BF02387851
Ogden CL, Carroll MD, Kit BK, Flegal KM (2014) Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 311:806–814. https://doi.org/10.1001/JAMA.2014.732
Ahrens W, Pigeot I, Pohlabeln H, De Henauw S, Lissner L, Molnár D, Moreno LA, Tornaritis M, Veidebaum T, Siani A, IDEFICS consortium (2014) Prevalence of overweight and obesity in European children below the age of 10. Int J Obes (Lond) 38(Suppl 2):S99–S107. https://doi.org/10.1038/IJO.2014.140
Guarino S, Capalbo D, Martin N, Campana G, Rambaldi PF, Miraglia Del Giudice E, La Manna A, Marzuillo P (2020) In children with urinary tract infection reduced kidney length and vesicoureteric reflux predict abnormal DMSA scan. Pediatr Res 87:779–784. https://doi.org/10.1038/s41390-019-0676-1
KDIGO (2012) Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 33:1–150
Obrycki Ł, Sarnecki J, Lichosik M, Sopińska M, Placzyńska M, Stańczyk M, Mirecka J, Wasilewska A, Michalski M, Lewandowska W, Dereziński T, Pac M, Szwarc N, Annusewicz K, Rekuta V, Ažukaitis K, Čekuolis A, Wierzbicka A, Jankauskiene A, Kalicki B, Jobs K, Tkaczyk M, Feber J, Litwin M (2022) Kidney length normative values in children aged 0–19 years - a multicenter study. Pediatr Nephrol 37:1075–1085. https://doi.org/10.1007/S00467-021-05303-5
Xargay-Torrent S, Puerto-Carranza E, Marcelo I, Mas-Parés B, Gómez-Vilarrubla A, Martínez-Calcerrada JM, de Zegher F, Ibáñez L, López-Bermejo A, Bassols J (2021) Estimated glomerular filtration rate and cardiometabolic risk factors in a longitudinal cohort of children. Sci Rep 11:11702. https://doi.org/10.1038/s41598-021-91162-x
Lizarraga-Mollinedo E, Martínez-Calcerrada JM, Padrós-Fornieles C, Mas-Pares B, Xargay-Torrent S, Riera-Pérez E, Prats-Puig A, Carreras-Badosa G, de Zegher F, Ibáñez L, Bassols J, López-Bermejo A (2019) Renal size and cardiovascular risk in prepubertal children. Sci Rep 9:5265. https://doi.org/10.1038/s41598-019-41757-2
Carrascosa A, Fernández JM, Fernández C, Ferrández A, López-Siguero JP, Sánchez E, Sobradillo B, Yeste D (2008) Spanish growth studies 2008. New anthropometric standards Endocrinol Nutr 55:484–506. https://doi.org/10.1016/S1575-0922(08)75845-5
Centers for Disease Control and Prevention Defining Childhood Weight Status | Overweight & Obesity | CDC. https://www.cdc.gov/obesity/basics/childhood-defining.html. Accessed 11 May 2022
(2004) A health professional’s guide to using growth charts. Paediatr Child Health 9:174–176. https://doi.org/10.1093/PCH/9.3.174
Lurbe E, Cifkova R, Cruickshank JK, Dillon MJ, Ferreira I, Invitti C, Kuznetsova T, Laurent S, Mancia G, Morales-Olivas F, Rascher W, Redon J, Schaefer F, Seeman T, Stergiou G, Wühl E, Zanchetti A, Sociedad Europea de Hipertensión (2010) Management of high blood pressure in children and adolescents: recommendations of the European Society of hypertension. An Pediatr (Barc) 73:51.e1–28. https://doi.org/10.1016/J.ANPEDI.2010.04.001
Levey AS, Eckardt KU, Dorman NM, Christiansen SL, Hoorn EJ, Ingelfinger JR, Inker LA, Levin A, Mehrotra R, Palevsky PM, Perazella MA, Tong A, Allison SJ, Bockenhauer D, Briggs JP, Bromberg JS, Davenport A, Feldman HI, Fouque D, Gansevoort RT, Gill JS, Greene EL, Hemmelgarn BR, Kretzler M, Lambie M, Lane PH, Laycock J, Leventhal SE, Mittelman M, Morrissey P, Ostermann M, Rees L, Ronco P, Schaefer F, St Clair Russell J, Vinck C, Walsh SB, Weiner DE, Cheung M, Jadoul M, Winkelmayer WC (2020) Nomenclature for kidney function and disease: report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int 97:1117–1129. https://doi.org/10.1016/J.KINT.2020.02.010
Di Bonito P, Licenziati MR, Campana G, Chiesa C, Pacifico L, Manco M, Miraglia Del Giudice E, Di Sessa A, Baroni MG, Marzuillo P, Valerio G (2021) Prevalence of mildly reduced estimated GFR by height- or age-related equations in young people with obesity and its association with cardiometabolic risk factors. J Ren Nutr 31:586–592. https://doi.org/10.1053/J.JRN.2020.11.005
Departament de salut (2020) ORDRE SLT/63/2020, de 8 de març, per la qual s’aproven els preus públi. https://www.clc.cat/pdf/module_28/10015462/Ordre-SLT____TFsk9YiZzVZ9MSh7fWvy_es.pdf. Accessed 16 May 2022
Sinha A, Bagga A, Krishna A, Bajpai M, Srinivas M, Uppal R, Agarwal I; Indian Society of Pediatric Nephrology (2013) Revised guidelines on management of antenatal hydronephrosis. Indian Pediatr 50:215–231. https://doi.org/10.1007/S13312-013-0064-6
Isert S, Müller D, Thumfart J (2020) Factors associated with the development of chronic kidney disease in children with congenital anomalies of the kidney and urinary tract. Front Pediatr 8:298. https://doi.org/10.3389/FPED.2020.00298
Peters C, Rushton HG (2010) Vesicoureteral reflux associated renal damage: congenital reflux nephropathy and acquired renal scarring. J Urol 184:265–273. https://doi.org/10.1016/j.juro.2010.03.076
Moëll H (1956) Size of normal kidneys Acta radiol 46:640–645. https://doi.org/10.3109/00016925609171457
Nahm AM, Ritz E (2000) Errors in ultrasonographic measurements of the kidney. Nephrol Dial Transplant 15:549–550. https://doi.org/10.1093/ndt/15.4.549
Chiolero A, Cachat F, Burnier M, Paccaud F, Bovet P (2007) Prevalence of hypertension in schoolchildren based on repeated measurements and association with overweight. J Hypertens 25:2209–2217. https://doi.org/10.1097/HJH.0B013E3282EF48B2
Vega MW, Swartz SJ, Devaraj S, Poyyapakkam S (2020) Elevated serum creatinine: but is it renal failure? Pediatrics 146:e20192828. https://doi.org/10.1542/PEDS.2019-2828/37011
La Scola C, De Mutiis C, Hewitt IK, Puccio G, Toffolo A, Zucchetta P, Mencarelli F, Marsciani M, Dall’Amico R, Montini G (2013) Different guidelines for imaging after first UTI in febrile infants: yield, cost, and radiation. Pediatrics 131:e665–e671. https://doi.org/10.1542/peds.2012-0164
Kleinerman RA (2006) Cancer risks following diagnostic and therapeutic radiation exposure in children. Pediatr Radiol 36:121–125. https://doi.org/10.1007/s00247-006-0191-5
Bravo-Saquicela DM, Sabag A, Rezende LFM, Rey-Lopez JP (2022) Has the prevalence of childhood obesity in Spain plateaued? A systematic review and meta-analysis. Int J Environ Res Public Health 19:5240. https://doi.org/10.3390/ijerph19095240
Restrepo JM, Torres-Canchala L, Viáfara LM, Agredo MA, Quintero AM, Filler G (2021) Renal length z-score for the detection of dysfunction in children with solitary functioning kidney. Acta Paediatr Int J Paediatr 110:652–658. https://doi.org/10.1111/APA.15425
Restrepo JM, Torres-Canchala L, Cadavid JCA, Ferguson M, Villegas A, Ramirez O, Rengifo M, Filler G (2022) Renal volume of five-year-old preterm children are not different than full-term controls. J Pediatr (Rio J) 98:282–288. https://doi.org/10.1016/j.jped.2021.06.008
Torres-Canchala L, Rengifo M, Filler G, Arias JC, Ramirez O, Restrepo JM (2021) Low agreement between kidney volume and kidney length z-scores. Pediatr Nephrol 36:1525–1532. https://doi.org/10.1007/s00467-020-04836-5
Funding
Open access funding provided by Università degli Studi della Campania Luigi Vanvitelli within the CRUI-CARE Agreement. The study was supported by grants from the Ministerio de Ciencia e Innovación, Instituto de Salud Carlos III, Madrid, Spain (PI20/00399 to JB and PI19/00451 to ALB), projects co-funded by FEDER (Fondo Europeo de Desarrollo Regional). JB is an Investigator of the Miguel Servet Fund (CPII17/00013; National Institute of Health Carlos III, Spain). ALB is an Investigator of the I3 Fund for Scientific Research (Ministry of Science and Innovation, Spain).
Author information
Authors and Affiliations
Contributions
Dr Marzuillo had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis and conceptualized and designed the study, participated in the analysis and interpretation of data, drafted the manuscript, critically revised the manuscript for important intellectual content, participated in the statistical analysis.
Prof Bassols and López-Bermejo participated in the acquisition, analysis and interpretation of data, critically revised the manuscript for important intellectual content and supervised the study.
Drs Carreras-Badosa and Martínez-Calcerrada participated in the acquisition, analysis and interpretation of data, critically revised the manuscript for important intellectual content.
Drs Guarino, Palma and Petrone participated in the dataset preparation, analysis and interpretation of data, critically revised the manuscript for important intellectual content, and participated in the statistical analysis.
Prof Miraglia del Giudice participated in analysis and interpretation of data, drafted the manuscript, and critically revised the manuscript for important intellectual content.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Obtained.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
{kind=link}
Cite this article
Marzuillo, P., Carreras-Badosa, G., Martínez-Calcerrada, JM. et al. Body surface area-based kidney length percentiles misdiagnose small kidneys in children with overweight/obesity. Pediatr Nephrol 38, 1523–1532 (2023). https://doi.org/10.1007/s00467-022-05718-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05718-8