
Abstract
Introduction
Ultrasound has been nicknamed “the surgeon’s stethoscope”. The advantages of laparoscopic ultrasound beyond a substitute for the sense of touch are considerable, especially for robotic surgery. Being able to see through parenchyma and into vascular structures enables to avoid unnecessary dissection by providing a thorough assessment at every stage without the need for contrast media or ionising radiation. The limitations of restricted angulation and access within the abdominal cavity during laparoscopy can be overcome by robotic handling of miniaturised ultrasound probes and the use of various and specific frequencies will meet tissue- and organ-specific characteristics. The aim of this systematic review was to assess the reported applications of intraoperative ultrasound-guided robotic surgery and to outline future perspectives.
Methods
The study adhered to the PRISMA guidelines. PubMed, Google Scholar, ScienceDirect and ClinicalTrials.gov were searched up to October 2023. Manuscripts reporting data on ultrasound-guided robotic procedures were included in the qualitative analysis.
Results
20 studies met the inclusion criteria. The majority (53%) were related to the field of general surgery during liver, pancreas, spleen, gallbladder/bile duct, vascular and rectal surgery. This was followed by other fields of oncological surgery (42%) including urology, lung surgery, and retroperitoneal lymphadenectomy for metastases. Among the studies, ten (53%) focused on locating tumoral lesions and defining resection margins, four (15%) were designed to test the feasibility of robotic ultrasound-guided surgery, while two (10.5%) aimed to compare robotic and laparoscopic ultrasound probes. Additionally two studies (10.5%) evaluated the robotic drop-in probe one (5%) assessed the hepatic tissue consistency and another one (5%) aimed to visualize the blood flow in the splenic artery.
Conclusion
The advantages of robotic instrumentation, including ergonomics, dexterity, and precision of movements, are of relevance for robotic intraoperative ultrasound (RIOUS). The present systematic review demonstrates the virtue of RIOUS to support surgeons and potentially reduce minimally invasive procedure times.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
In the last few decades, there has been a rapid succession of technological advances, marking a radical shift from the open to the minimally invasive surgical (MIS) approach [1]. The advantages of laparoscopy over laparotomy are now widely acknowledged [2]. Over the past twenty-five years, robotic surgery has experienced a raise and today, with the availability of several platforms alongside the continuously leading da Vinci systems (Intuitive Surgical Inc., Sunnyvale, CA, USA), robotic approaches are playing an increasingly crucial role [3, 4]. Despite observed advantages for certain patient characteristics (e.g., BMI > 30), challenges such as the lack of dedicated reimbursement, high costs and often longer operating times still limit the widespread use of robotic platforms worldwide [5]. Open surgery provides direct visual and tactile information of the explored regions. In contrast, MIS comes at the cost of predominantly two-dimensional view and limited tactile assessment. Intraoperative ultrasound (IOUS) is commonly utilized during open surgery with linear or finger probes, particularly in the hepatobiliary (HPB) and urological fields [6, 7]. In laparoscopic setting, ultrasound probes for guidance in MIS are more challenging to handle [8]. To overcome this limitation, innovative approaches for robotic platforms integrate ultrasound imaging to facilitate its use in MIS [9]. Image-guided robotic approaches, particularly those based on three-dimensional (3D) imaging, augmented reality (AR), and machine learning algorithms, offer advantages in the era of digital surgery [10]. Real-time, non-invasive, cost-effective and dynamic intraoperative imaging of complex anatomy are the main benefits of computer-assisted surgery. In this context, IOUS has emerged as the imaging modality of choice facilitated by the introduction of articulated robotic instruments to handle ultrasound probes [11]. The augmentation and fusion of imaging modalities are especially beneficial for delineating healthy and neoplastic tissue in oncological surgery [12]. The navigation of drop-in ultrasound probes manoeuvred by articulated robotic graspers provides access to anatomical spaces and angles that are inconvenient for relatively rigid laparoscopic probes. While initial reports of applications of intraoperative ultrasound during robotic surgery (RIOUS) have been published in the fields traditionally managed by open surgery, with encouraging results., pooled data are lacking [6, 13]. Therefore, the aim of this systematic review is to assess the reported applications of intraoperative ultrasound-guided robotic surgery and to outline future perspectives.
Materials and methods
Search strategy
The systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [14] and registered with the International Prospective Register of Systematic Reviews PROSPERO (n CRD42023494430) prior to data extraction. Articles were obtained by querying the PubMed database, Google Scholar, ScienceDirect and ClinicalTrial.gov filtered by the English language up to October 2023 without additional restrictions. The database was retrieved through title and abstract screening using the following search terms: “intraoperative”, “robotic”, “surgery”, “ultrasound”, “laparoscopic”, “probe”.
Data extraction
After removing duplicate publications, titles, abstracts, and keywords were independently reviewed by M.P and E.T. for inclusion, followed by full text review of eligible articles. In case of discrepancies, a consensus was reached through agreement with a third author (M.G.). The inclusion criterion was the description of ultrasound-assisted robotic surgical procedures. Excluded were articles without robotic use of the probe, as well as abstracts, reviews, meta-analyses, letters, and editorials. Studies reporting robotic ultrasound imaging independently of a surgical procedure, or those focused on percutaneous ultrasound-guided techniques and biopsies were also excluded. Data about the authors, surgical procedures, probes specifics and ultrasound-assisted robotic procedures were extracted for further analysis.
Results
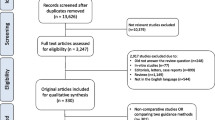
The search strategy identified studies reporting intraoperative ultrasound imaging during robotic surgery. Initially, 781 studies were identified, and 68 full texts were selected through title and abstract screening. Finally, 20 studies met the inclusion criteria for the systematic review (Fig. 1). Due to the low number of reports, a qualitative analysis was performed [6,7,8, 11, 13, 15,16,17,18,19,20,21,22,23,24,25,26,27,28].

PRISMA flow diagram of study selection
Among the included studies, two were prospective (10%), fifteen teen were retrospective (75%), three were experimental (15%), involving laboratory tests in vivo (porcine models) or on ex vivo phantoms. The studies were mainly (53%) from the field of general surgery during liver, pancreas, spleen, gallbladder/bile duct, vascular and rectal surgery [6, 8, 11, 16,17,18,19,20,21,22, 28]. The remaining studies(42%) covered other fields of oncological surgery including urology [7, 13, 23,24,25,26], lung surgery [27], and retroperitoneal lymphadenectomy for metastases [15].
Ten studies (53%) were focused on locating tumoral lesions and defining resection margins [7, 11, 13, 18,19,20, 22, 25, 27, 29]. Additionally, four studies (15%) were designed to assess the feasibility of robotic ultrasound-guided surgery [8, 15, 23], two (10.5%) aimed to compare robotic and laparoscopic ultrasound probes [6, 24], another two (10.5%) were conducted to evaluate the robotic drop-in probe [13, 16], one study (5%) focused on assessing hepatic tissue consistency [17] and another (5%) aimed to visualize the blood flow in the splenic artery [21].
In eleven articles (55%), a miniaturized linear drop-in probe was used [6, 7, 11, 13, 15, 16, 23,24,25, 27, 28]. These probes can be introduced via a 10–12 mm accessory trocar and steered from the surgeon’s console using robotic graspers (Fig. 2). Five manuscripts reported the use of rigid probes, which can be docked to the robotic arm (12 mm trocar) as prototypes corresponding to da Vinci robotic instruments (Fig. 2) [8, 21]. Alternatively, a laparoscopic articulated probe can be used during robotic surgery, introduced via the 10 mm accessory port and manipulated by the bedside assistant (Fig. 2). The ultrasound frequencies of the probes used in the included studies ranged from 3 to 13 MHz. All reported procedures were performed with the da Vinci robotic platforms. Table 1 summarizes the characteristics of the included articles, and details about ultrasound probes and surgical applications. No clinical trials on the use of RIOUS were registered at the timepoint of the database query. Due to the heterogeneity of data concerning probes, frequencies, procedures and study outcomes, a quantitative analysis of the results was deemed inappropriate.

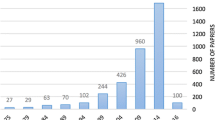
Timeline of intraoperative ultrasound techniques
Discussion
In this systematic review, we present a a comprehensive analysis that sheds light on the current state of intraoperative ultrasound for guidance in robotic procedures.
Summary of main results
Despite the high quality level of evidence supporting laparoscopic ultrasound in various thoraco-abdominal pathologies [30] and the desire to implement RIOUS for over two decades [31], the literature still reflects limited evidence regarding ultrasound guidance during robotic surgery, with relatively small cohort sizes.
All included studies, however, consistently report satisfactory performance of RIOUS. To facilitate the widespread adoption of RIOUS, there is a need for increased adoption of robotic surgical procedures and training for surgeons in IOUS. The utilization of computer assistance for image acquisition and interpretation, through the development and training of machine learning algorithms, could contribute to overcoming operator dependency in ultrasound examinations [32]. In line with the findings of this analysis on RIOUS, image guidance for identifying resection margins by differentiating between healthy and neoplastic tissues has proven particularly useful in oncological diseases [33]. The foremost beneficiary of (R)IOUS thus far is the hepatobiliary field, particularly for the comprehensive anatomical assessment of the biliary and vascular trees [34]. In liver surgery, IOUS plays a well-established role as an intraoperative guidance tool in combination with preoperative CT and MRI imaging. Surgical radicality depends on the detectability of lesions in the different imaging modalities. Techniques such as image fusion of CT/MRI and US, multimodal registration of 2D and 3D imaging modalities as well as (contrast-enhanced) ultrasound contribute to identifying known and preoperatively undetected lesions in order to intraoperatively tailor the surgical strategy [35, 36]. Furthermore, RIOUS was demonstrated to have superior performance compared to conventional LIOUS with a success rate exceeding the one of LIOUS in liver surface exploration (85% vs. 73%, P = 0.030) and tool manipulation (79% vs. 57%, P = 0.028) [8]. Post-task questionnaires completed by participating surgeons revealed that robotic ultrasound significantly improved probe positioning (80%), reduced fatigue (90%), and was overall more useful than LIOUS (90%) [8]. Facilitating precise probe positioning in RIOUS not only enhances surgical precision but also reduces the physical strain on surgeons during complex procedures [6]. An even more significant benefit is the opportunity to identify otherwise undetected lesions, such as in pancreatic lesions [18]. In benign disease of the biliary tract, IOUS has demonstrated comparable efficacy with intraoperative cholangiography in diagnosing choledocholithiasis, surpassing it in terms of speed and completion rates. This is achieved without the need for a contrast agent, with reduced invasiveness and a decreased risk of infection.The comprehensive assessment of the intra- and extrahepatic biliary tree can be accomplished in an average time of 164.1 s using RIOUS and can be complemented by Doppler ultrasound for assessing the porta hepatis. Precise measurements of the biliary tree and ductal stones enable intraoperative decision-making and management of ductal pathologies, including hybrid approaches [6, 37].
Similarly, rectal tumours were successfully detected using RIOUS, showing its effectiveness in determining the optimal transection line for rectal surgeries, especially in cases where tumours are too high for transanal palpation [16]. Furthermore, in obese patient with rectal cancer RIOUS has been proved to be useful to safely guide vascular dissection [28]. Nephron-sparing surgery, as an alternative to radical nephrectomy, is gaining support as an oncologically equivalent procedure while preserving renal functional capacity [9]. The evolution of robot-assisted partial nephrectomy techniques has ushered in a progressive refinement of tools aiding surgeons in the identification of masses and their vascular networks. A remarkable 100% success rate was demonstrated in identifying kidney lesions with RIOUS [25], optimizing tumour identification, enhancing renal tissue preservation through partial nephrectomy, and ensuring oncological safety [6, 9, 37]. In transoral robotic tongue base resection for obstructive sleep apnoea RIOUS has emerged as an invaluable tool for locating the lingual artery and assessing laryngeal tissues. The integration of RIOUS significantly enhances efficiency by substantially reducing the risk of detrimental intraoperative bleeding complications [29].
Despite the numerous advantages observed across various surgical domains, the integration of intraoperative ultrasound in the robotic field remains underused due to costs consideration, lack of expertise, and the necessity for highly skilled minimally invasive surgeons trained in both robotics and ultrasound techniques [11]. Moreover, although rigid prototypes compatible with robotic arms have been developed [8, 20], they are barely due to cost and the absence of a significant advantages over rigid laparoscopic probes, [6, 38]. In contrast, the adaptability of drop-in probes to all multi- and single-port robotic platforms offers high scalability in clinical applications [6, 8, 20, 38].
Results in the context of published literature
Applications of IOUS originated in 1960 for the identification of kidney stones in A-mode [34, 39]. Since 1980s, rapid innovations have progressed with applications in hepato-pancreato-biliary and gastrointestinal surgery [40, 41]. In the 1990s, attempts were made to extend the benefits of IOUS to minimally invasive surgery by creating dedicated probes for laparoscopic ultrasound [42]. When used in the robotic setting, these probes were operated by the bedside assistant. However, laparoscopic probes lack the flexibility of IOUS in open surgery (Fig. 2). As robotic platforms do not yet provide integrated ultrasound probes, a specific transducer known as the “drop-in-probe" was recently introduced for robotic surgery. This probe, with a dorsal fin to be grasped with a robotic instrument, can be steered from the console. The small transducer attached to a highly flexible cable, coupled with the motion range of the articulating instrument, facilitates access to anatomical areas that are hard to reach with standard laparoscopic probes.
Furthermore, dedicated robotic console software, such as TilePro (Intuitive Surgical Inc., Sunnyvale, CA, USA), enables the surgeon to create an in-console split-view with side-by-side intraoperative and ultrasound images, or switch between the minimally invasive 3D camera and ultrasound view directly from the console [22]. On platforms with open consoles, surgeons can switch from the integrated robotic display to the external ultrasound screen ideally positioned close to the console surgeon [43]. One of the known limitations of laparoscopy, and even more so in robotic surgery, is the reduced/absent tactile feedback, requiring considerable training is needed to learn to replace haptic with visual information. Consequently, the availability of additional information via RIOUS is particularly relevant in oncology, where achieving zero residual tumour is a major prognostic factor [44,45,46,47,48]. Exploration of the abdominal cavity with LIUOS can detect malignant deposits preventing conversions to open surgery when remaining disease can be excluded [44,45,46,47, 49]. Fertility-sparing surgery can be enhanced by IOUS assistance by discriminating healthy from cancerous tissues and to spare ovarian parenchyma [46]. Image-guided organ exploration during surgery could also impact the detection of undiagnosed masses, especially in pancreatic and splenic diseases [11, 18, 19]. Therefore, margin assessment and mapping resection guidance with IOUS are highly relevant in conservative oncologic surgery [50, 51]. However, large-scale future randomized controlled trials (RCTs) are necessary to demonstrate the utility of IOUS in assessing oncological outcomes.
Although the limited number of publications and the presence of heterogeneity among the included studies, mostly consisting of case reports and case series which have been included to report comprehensively the literature evidence, this systematic review on RIOUS procedures highlights the relevance of the technical advances in robotic surgery which underline its expected impact in the field of image-guided surgery.
Implications for practice and future research
In recent years, an increasing number of robotic platforms has entered the marketplace, a trend expected to persist with decreasing costs and user-friendly platforms for a variety of procedures [3]. However, as the integration of advanced technology based on artificial intelligence and augmented reality is not yet fully automated, making the inclusion of real-time 3D image information into MIS a crucial step in advancing surgical care [10]. Ultrasound-assisted procedures are poised to play a pivotal role in filling this technological gap and are anticipated to grow in parallel with ongoing advancements.
Beyond 3D macroscopic guidance, there is a growing demand for real-time intraoperative tissue analysis, particularly for tailoring the radicality of resection in oncological diseases. In vivo 3D tissue analysis would be ideal for guiding surgery intraoperatively. A variety of intraoperative optical imaging techniques are currently under assessment to complement or potentially replace extemporaneous histopathological analysis [23, 52]. For in vivo tissue, 3D high resolution ultrasound represents a significant step forward in intraoperative analysis within the anatomical context, aiding decision-making on whether resection is required, such as in lymph node metastasis [50]. High (up to 70 MHz) and ultra-high (up to 100 MHz) frequency probes are considered candidates to achieve a resolution of 30 µm, similar to histopathology [53]. An immediate ex vivo imaging system that does not require dedicated sample preparation is full-field optical coherence tomography (FF-OCT), showing a rapid learning curve and analysis of tissue sections similar to [54, 55]. On resected specimens, whole-slide imaging can be used for digital reconstruction as a 3D volume preventing missed lesions for skipped depth slide [56]. In the era of digital surgery, robotic platforms represent computer interfaces capable of integrating multiple modalities of real-time data analysis [10] (Fig. 3). The integration of surgical and imaging sciences will need interdisciplinary training and specific core curricula such as the Master in Image-Guided Surgery, teaching surgeons to perform IOUS, particularly in MIS [57]. Moreover, ongoing studies in deep learning applied to new diagnostic technologies will address the need for standardised IOUS performance and data interpretation by surgeons who may lack adequate radiological expertise [58,59,60].

(Copyright Barbara Seeliger/ Carlos Amato; Chengyuan Yang; Niloofar Badihi; IHU Strasbourg and Cannon Design USA)
The next-generation hybrid operating room integrating artificial intelligence and robotics for diagnostic imaging, procedure planning and execution: the operating room of the future is envisioned as the centre of a technology ecosystem. Illustrated technology include advanced interactive digital displays with real-time connectivity and AI analytics, mixed-reality environments, and robotic applications for various interventions, imaging (ultrasound, cone-beam CT, intraoperative CT/MRI, etc.), nursing assistance and sterile instrument management, as well as a predictive logistics supply system with Automatic Guided Vehicles [61]
Conclusions
Robotic surgery has become increasingly common in routine clinical practice. Recent technological advancements have paved the way for new tools and equipment in robotic and image-guided surgery. The advantages of robotic instrumentation, including ergonomics, dexterity, and precision of movements, are particularly relevant for robotic intraoperative ultrasound. This systematic review demonstrates the virtue of RIOUS to support intraoperative decision-making and potentially reduce minimally invasive procedure times. Prospective studies, however, are needed to better understand its potential, including disciplines like gynaecologic oncology, where these procedures are not yet commonly performed.
Data availability
All data generated or analysed in this review are included in this article and/or its figures. Further enquiries can be directed to the corresponding author.
References
Gueli Alletti S, Rosati A, Capozzi VA, Pavone M, Gioè A, Cianci S et al (2022) Use of laparoscopic and laparotomic J-plasma handpiece in gynecological malignancies: results from a pilot study in a tertiary care center. Front Oncol 12:868930
Gueli Alletti S, Petrillo M, Vizzielli G, Bottoni C, Nardelli F, Costantini B et al (2016) Minimally invasive versus standard laparotomic interval debulking surgery in ovarian neoplasm: a single-institution retrospective case-control study. Gynecol Oncol 143(3):516–520
Pavone M, Marescaux J, Seeliger B (2023) Current status of robotic abdominopelvic surgery. 秀傳醫學雜誌;(預刊文章):1–15
Pavone M, Seeliger B, Alesi MV, Goglia M, Marescaux J, Scambia G et al (2023) Initial experience of robotically assisted endometriosis surgery with a novel robotic system: first case series in a tertiary care center. Updates Surg. https://doi.org/10.1007/s13304-023-01724-z
Monterossi G, Pedone Anchora L, Gueli Alletti S, Fagotti A, Fanfani F, Scambia G (2022) The first European gynaecological procedure with the new surgical robot HugoTM RAS. A total hysterectomy and salpingo-oophorectomy in a woman affected by BRCA-1 mutation. Facts Views Vis Obgyn 14(1):91–4
Glaysher MA, Beable R, Ball C, Carter NC, Knight BC, Pucher PH et al (2023) Intra-operative ultrasound assessment of the biliary tree during robotic cholecystectomy. J Robot Surg 17(6):2611–2615
Kaczmarek BF, Sukumar S, Petros F, Trinh QD, Mander N, Chen R et al (2013) Robotic ultrasound probe for tumor identification in robotic partial nephrectomy: initial series and outcomes. Int J Urol 20(2):172–176
Schneider CM, Peng PD, Taylor RH, Dachs GW, Hasser CJ, DiMaio SP et al (2012) Robot-assisted laparoscopic ultrasonography for hepatic surgery. Surgery 151(5):756–762
Di Cosmo G, Verzotti E, Silvestri T, Lissiani A, Knez R, Pavan N et al (2018) Intraoperative ultrasound in robot-assisted partial nephrectomy: state of the art. Arch Ital Urol Androl 90(3):195–198
Lecointre L, Verde J, Goffin L, Venkatasamy A, Seeliger B, Lodi M et al (2022) Robotically assisted augmented reality system for identification of targeted lymph nodes in laparoscopic gynecological surgery: a first step toward the identification of sentinel node. Surg Endosc 36(12):9224–9233
Guerra F, Amore Bonapasta S, Annecchiarico M, Bongiolatti S, Coratti A (2015) Robot-integrated intraoperative ultrasound: initial experience with hepatic malignancies. Minim Invas Ther Allied Technol 24(6):345–349
Sokolenko A, Preobrazhenskaya E, Marchetti C, Piermattei A, Zagrebin F, Kuligina E et al (2023) Origin of residual tumor masses in BRCA1/2-driven ovarian carcinomas treated by neoadjuvant chemotherapy: selection of preexisting BRCA1/2-proficient tumor cells but not the gain of second ORF-restoring mutation. Pathobiology. https://doi.org/10.1159/000533591
Sun Y, Wang W, Zhang Q, Zhao X, Xu L, Guo H (2021) Intraoperative ultrasound: technique and clinical experience in robotic-assisted renal partial nephrectomy for endophytic renal tumors. Int Urol Nephrol 53(3):455–463
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2006) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6(7):e1000097
Zhang K, Zhu G, Liu X, Tian J, Gu Y, Zhai M et al (2019) Robot-assisted laparoscopic retroperitoneal lymph node dissection with concomitant inferior vena cava thrombectomy for metastatic mixed testicular germ cell cancer: a case report. J Med Case Rep 13(1):272
Otani K, Kiyomatsu T, Ishimaru K, Kataoka A, Hayashi Y, Gohda Y (2023) Usefulness of real-time navigation using intraoperative ultrasonography for rectal cancer resection. Asian J Endosc Surg 16(4):819–821
Giulianotti PC, Buchs NC, Coratti A, Sbrana F, Lombardi A, Felicioni L et al (2011) Robot-assisted treatment of splenic artery aneurysms. Ann Vasc Surg 25(3):377–383
Liu Y, Ji WB, Wang HG, Luo Y, Wang XQ, Lv SC et al (2015) Robotic spleen-preserving laparoscopic distal pancreatectomy: a single-centered Chinese experience. World J Surg Oncol 13(1):275
Araujo RLC, de Castro LA, Fellipe FEC, Burgardt D, Wohnrath DR (2018) Robotic left lateral sectionectomy as stepwise approach for cirrhotic liver. J Robot Surg 12(3):549–552
Di Mitri M, Thomas E, Di Carmine A, Manghi I, Cravano SM, Bisanti C et al (2023) Intraoperative ultrasound in minimally invasive laparoscopic and robotic pediatric surgery: our experiences and literature review. Children (Basel) 10(7):1153
Billings S, Deshmukh N, Kang HJ, Taylor R, Boctor EM (2012) System for robot-assisted real-time laparoscopic ultrasound elastography. In: Medical Imaging 2012: Image-Guided Procedures, Robotic Interventions, and Modeling. SPIE, pp 589–596. https://doi.org/10.1117/12.911086. Accessed 1 Oct 2023
Pessaux P, Diana M, Soler L, Piardi T, Mutter D, Marescaux J (2015) Towards cybernetic surgery: robotic and augmented reality-assisted liver segmentectomy. Langenbecks Arch Surg 400(3):381–385
Yakoubi R, Autorino R, Laydner H, Guillotreau J, White MA, Hillyer S et al (2012) Initial laboratory experience with a novel ultrasound probe for standard and single-port robotic kidney surgery: increasing console surgeon autonomy and minimizing instrument clashing. Int J Med Robot 8(2):201–205
Kaczmarek BF, Sukumar S, Kumar RK, Desa N, Jost K, Diaz M et al (2013) Comparison of robotic and laparoscopic ultrasound probes for robotic partial nephrectomy. J Endourol 27(9):1137–1140
Gunelli R, Fiori M, Salaris C, Salomone U, Urbinati M, Vici A et al (2016) The role of intraoperative ultrasound in small renal mass robotic enucleation. Arch Ital Urol Androl 88(4):311–313
Zhang Y, Ouyang W, Wu B, Pokhrel G, Ding B, Xu H et al (2020) Robot-assisted partial nephrectomy with a standard laparoscopic ultrasound probe in treating endophytic renal tumor. Asian J Surg 43(2):423–427
Zhou Z, Wang Z, Zheng Z, Cao J, Zhang C, He Z et al (2017) An ‘alternative finger’ in robotic-assisted thoracic surgery: intraoperative ultrasound localization of pulmonary nodules. Med Ultrason 19(4):374–379
Maertens V, Stefan S, Mykoniatis I, Siddiqi N, David G, Khan JS (2023) Robotic CME in obese patients: advantage of robotic ultrasound scan for vascular dissection. J Robot Surg 17(1):155–161
Chang CC, Wu JL, Hsiao JR, Lin CY (2021) Real-time, intraoperative, ultrasound-assisted transoral robotic surgery for obstructive sleep apnea. Laryngoscope 131(4):E1383–E1390
Jamal KN, Smith H, Ratnasingham K, Siddiqui MR, McLachlan G, Belgaumkar AP (2016) Meta-analysis of the diagnostic accuracy of laparoscopic ultrasonography and intraoperative cholangiography in detection of common bile duct stones. Ann R Coll Surg Engl 98(4):244–249
Angelini L, Papaspyropoulos V (2000) Robotics and telecommunication systems to provide better access to ultrasound expertise in the OR. Minim Invas Ther Allied Technol 9(3–4):219–224
Avesani G, Tran HE, Cammarata G, Botta F, Raimondi S, Russo L et al (2022) CT-based radiomics and deep learning for BRCA mutation and progression-free survival prediction in ovarian cancer using a multicentric dataset. Cancers (Basel) 14(11):2739
Sena G, Paglione D, Gallo G, Goglia M, Osso M, Nardo B (2022) Surgical resection of a recurrent hepatocellular carcinoma with portal vein thrombosis: is it a good treatment option? A case report and systematic review of the literature. J Clin Med 11(18):5287
Schlegel JU, Diggdon P, Cuellar J (1961) The use of ultrasound for localizing renal calculi. J Urol 86(4):367–369
Jung EM, Clevert DA (2018) Contrast-enhanced ultrasound (CEUS) and image fusion for procedures of liver interventions. Radiologe 58(6):538–544
Torzilli G (2004) Contrast-enhanced intraoperative ultrasonography in surgery for liver tumors. Eur J Radiol 51(Suppl):S25-29
Dietrich CF, Braden B, Burmeister S, Aabakken L, Arciadacono PG, Bhutani MS et al (2022) How to perform EUS-guided biliary drainage. Endosc Ultrasound 11(5):342–354
Leven J, Burschka D, Kumar R, Zhang G, Blumenkranz S, Dai XD et al (2005) DaVinci canvas: a telerobotic surgical system with integrated, robot-assisted, laparoscopic ultrasound capability. Med Image Comput Comput Assist Interv 8(Pt 1):811–818
Knight PR, Newell JA (1963) Operative use of ultrasonics in Cholelithiasis. Lancet 281(7289):1023–1025
Sigel B, Coelho JC, Spigos DG, Donahue PE, Renigers SA, Capek V et al (1980) Real-time ultrasonography during biliary surgery. Radiology 137(2):531–533
Fukuda M (1982) Studies on echolaparoscopy. Scan J Gastroenterol 17(Suppl 78):186
Jakimowicz JJ, Ruers TJM (2008) Ultrasound-assisted laparoscopic cholecystectomy: preliminary experience. Dig Surg 8(2):114–117
Pavone M, Goglia M, Campolo F, Scambia G, Ianieri MM (2023) En-block butterfly excision of posterior compartment deep endometriosis: the first experience with the new surgical robot Hugo™ RAS. Facts Views Vis Obgyn 15(4):359–362
De Blasis I, Tortorella L, Macchi C, Arciuolo D, Scambia G, Testa AC (2019) Intraoperative ultrasound diagnosis of metastatic lymph node in serous borderline ovarian tumor. Ultrasound Obstet Gynecol 54(4):562–563
Mascilini F, Quagliozzi L, Moro F, Moruzzi MC, Gallotta V, Alletti SG et al (2018) Role of intraoperative ultrasound to extend the application of minimally invasive surgery for treatment of recurrent gynecologic cancer. J Minim Invas Gynecol 25(5):848–854
Mascilini F, Quagliozzi L, Bolomini G, Scambia G, Testa AC, Fagotti A (2019) Intraoperative ultrasound through laparoscopic probe in fertility-sparing surgery for borderline ovarian tumor recurrence. Ultrasound Obstet Gynecol 54(2):280–282
Moro F, Uccella S, Testa AC, Scambia G, Fagotti A (2018) Intraoperative ultrasound-guided excision of cardiophrenic lymph nodes in an advanced ovarian cancer patient. Int J Gynecol Cancer 28(9):1672–1675
Marchetti C, Rosati A, De Felice F, Boccia SM, Vertechy L, Pavone M et al (2021) Optimizing the number of cycles of neoadjuvant chemotherapy in advanced epithelial ovarian carcinoma: a propensity-score matching analysis. Gynecol Oncol 163(1):29–35
Jones BP, Saso S, Farren J, El-Bahrawy M, Ghaem-Maghami S, Smith JR et al (2017) Ultrasound-guided laparoscopic ovarian wedge resection in recurrent serous borderline ovarian tumours. Int J Gynecol Cancer 27(9):1813–1818
Ferrucci M, Milardi F, Passeri D, Mpungu LF, Francavilla A, Cagol M et al (2023) Intraoperative ultrasound-guided conserving surgery for breast cancer: no more time for blind surgery. Ann Surg Oncol 30(10):6201–6214
Juvekar P, Torio E, Bi WL, Bastos DCDA, Golby AJ, Frisken SF (2023) Mapping resection progress by tool-tip tracking during brain tumor surgery for real-time estimation of residual tumor. Cancers (Basel) 15(3):825
Mascagni P, Padoy N (2021) OR black box and surgical control tower: recording and streaming data and analytics to improve surgical care. J Visc Surg 158(3S):S18-25
Izzetti R, Vitali S, Aringhieri G, Nisi M, Oranges T, Dini V et al (2021) Ultra-high frequency ultrasound, a promising diagnostic technique: review of the literature and single-center experience. Can Assoc Radiol J 72(3):418–431
Yang H, Zhang S, Liu P, Cheng L, Tong F, Liu H et al (2020) Use of high-resolution full-field optical coherence tomography and dynamic cell imaging for rapid intraoperative diagnosis during breast cancer surgery. Cancer 126(S16):3847–3856
Pavone M, Spiridon IA, Lecointre L, Seeliger B, Scambia G, Venkatasamy A et al (2023) Full-field optical coherence tomography imaging for intraoperative microscopic extemporaneous lymph node assessment. Int J Gynecol Cancer. https://doi.org/10.1136/ijgc-2023-005050
Seeliger B, Spiridon IA (2023) Towards optimisation in surgical pathology–the potential of artificial intelligence. BJS Academy. https://doi.org/10.58974/bjss/azbc011
Petter Frühling MD, Seeliger B, Rivera AKU, Freedman J, Giménez M, Digests HPB (2023) Image-guided ablation for liver tumours–an addition to the armamentarium of multidisciplinary oncological and surgical approaches. HPB. https://doi.org/10.58974/bjss/azbc025
Ho C, Calderon-Delgado M, Chan C, Lin M, Tjiu J, Huang S et al (2021) Detecting mouse squamous cell carcinoma from submicron full-field optical coherence tomography images by deep learning. J Biophotonics 14(1):e202000271
Mandache D, Dalimier E, Durkin JR, Boceara C, Olivo-Marin JC, Meas-Yedid V (2018) Basal cell carcinoma detection in full field OCT images using convolutional neural networks. In: 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), pp 784–787. https://ieeexplore.ieee.org/abstract/document/8363689
Scholler J, Mandache D, Mathieu MC, Lakhdar AB, Darche M, Monfort T et al (2023) Automatic diagnosis and classification of breast surgical samples with dynamic full-field OCT and machine learning. J Med Imaging (Bellingham) 10(3):034504
Seeliger B, Karagyris A, Mutter D (2023) The role of artificial intelligence in diagnostic medical imaging and next steps for guiding surgical procedures. BJS Academy. https://www.bjsacademy.com/the-role-of-artificial-intelligence-in-diagnostic-medical-imaging-and-next-steps-for-guiding-surgical-procedures. Accessed 17 Nov 2023
Acknowledgements
The authors are grateful to Catherine Cers-Meunier for illustrating the surgical procedures.
Funding
Open access funding provided by Università Cattolica del Sacro Cuore within the CRUI-CARE Agreement. This work was supported by French state funds managed within the “Plan Investissements d’Avenir” and by the ANR (reference ANR-10-IAHU-02).
Author information
Authors and Affiliations
Contributions
MP, BS, AT and DQ contributed to the study design. MP, ET and MG performed the literature research. MP, BS, ET, MG, NB drafted the manuscript. LL, CA, AF, JM, GS, ACT and DQ are responsible for the critical revision of the manuscript and for important intellectual content. All Authors have read and commented on the working versions and approved the final manuscript before submission.
Corresponding author
Ethics declarations
Disclosures
Barbara Seeliger has a research and education consultant agreement with CMR Surgical and Intuitive Surgical. Jacques Marescaux is the President and Founder of the IRCAD Institute, which is partly funded by Karl Storz, Medtronic and Intuitive Surgical. Matteo Pavone, Elena Teodorico, Marta Goglia, Nicolo` Bizzarri, Cristina Taliento, Antonello Forgione Giovanni Scambia, Antonia Carla Testa and Denis Querleu have no relevant conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pavone, M., Seeliger, B., Teodorico, E. et al. Ultrasound-guided robotic surgical procedures: a systematic review. Surg Endosc 38, 2359–2370 (2024). https://doi.org/10.1007/s00464-024-10772-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-024-10772-4