
Abstract
Background
Endoscopic papillectomy (EP) offers a safe and effective method for resection of ampullary adenomas. Data regarding the long-term resolution of adenoma following EP are limited. The aim of this study therefore was to examine the timing of recurrence after EP of ampullary adenomas.
Methods
This was a single-center retrospective study including patients who received EP for ampullary adenomas from 8/2000 to 1/2018. Patients with confirmed complete eradication of adenoma were included in the recurrence analysis with recurrence defined as finding adenomatous histology after 1 negative surveillance endoscopy. Kaplan–Meier estimates were calculated to determine recurrence rates.
Results
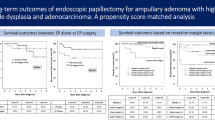
Of the 165 patients who underwent EP, 136 patients (mean age 61.9, 51.5% female) had adenomatous histology with a mean lesion size of 21.2 mm. A total of 124 (91.2%) achieved complete eradication with a follow-up of 345.8 person-years. Recurrence occurred in 20 (16.1%) patients at a mean of 3.2 (± 3) years (range 0.5–9.75 years) for a recurrence rate of 5.8 (95% CI 3.6–8.8) per 100 person-years. Nine (45%) recurrences occurred after the 1st 2 years of surveillance. Recurrence rate did not differ by baseline pathology [low-grade dysplasia: 5.2 (95% CI 3.0–9.0), high-grade dysplasia: 6.9 (95% CI 2.3–15.5), adenocarcinoma: 7.7 (95% CI 0.9–25.1)].
Conclusion
Recurrence remains a significant concern after EP. Given the timing of recurrence, long surveillance periods may be necessary. Larger multicenter studies are needed, however, to determine appropriate surveillance intervals.



Similar content being viewed by others


References
Seifert E, Schulte F, Stolte M (1992) Adenoma and carcinoma of the duodenum and papilla of Vater: a clinicopathologic study. Am J Gastroenterol 87:37–42
Ruemmele P, Dietmaier W, Terracciano L, Tornillo L, Bataille F, Kaiser A, Wuensch PH, Heinmoeller E, Homayounfar K, Luettges J, Kloeppel G, Sessa F, Edmonston TB, Schneider-Stock R, Klinkhammer-Schalke M, Pauer A, Schick S, Hofstaedter F, Baumhoer D, Hartmann A (2009) Histopathologic features and microsatellite instability of cancers of the papilla of vater and their precursor lesions. Am J Surg Pathol 33:691–704
Chathadi KV, Khashab MA, Acosta RD, Chandrasekhara V, Eloubeidi MA, Faulx AL, Fonkalsrud L, Lightdale JR, Salztman JR, Shaukat A, Wang A, Cash BD, DeWitt JM (2015) The role of endoscopy in ampullary and duodenal adenomas. Gastrointest Endosc 82:773–781
Vanbiervliet G, Strijker M, Arvanitakis M, Aelvoet A, Arnelo U, Beyna T, Busch O, Deprez PH, Kunovsky L, Larghi A, Manes G, Moss A, Napoleon B, Nayar M, Pérez-Cuadrado-Robles E, Seewald S, Barthet M, van Hooft JE (2021) Endoscopic management of ampullary tumors: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 53:429–448
Spadaccini M, Fugazza A, Frazzoni L, Leo MD, Auriemma F, Carrara S, Maselli R, Galtieri PA, Chandrasekar VT, Fuccio L, Aljahdli E, Hassan C, Sharma P, Anderloni A, Repici A (2020) Endoscopic papillectomy for neoplastic ampullary lesions: a systematic review with pooled analysis. United Eur Gastroenterol J 8:44–51
Lee TY, Cheon YK, Shim CS, Choi HJ, Moon JH, Choi JS, Oh HC (2016) Endoscopic wire-guided papillectomy versus conventional papillectomy for ampullary tumors: a prospective comparative pilot study. J Gastroenterol Hepatol 31:897–902
Onkendi EO, Naik ND, Rosedahl JK, Harmsen SW, Gostout CJ, Baron TH Sr, Sarr MG, Que FG (2014) Adenomas of the ampulla of Vater: a comparison of outcomes of operative and endoscopic resections. J Gastrointest Surg 18:1588–1596
Ma T, Jang EJ, Zukerberg LR, Odze R, Gala MK, Kelsey PB, Forcione DG, Brugge WR, Casey BW, Syngal S, Chung DC (2014) Recurrences are common after endoscopic ampullectomy for adenoma in the familial adenomatous polyposis (FAP) syndrome. Surg Endosc 28:2349–2356
Yasuda I, Kobayashi S, Takahashi K, Nanjo S, Mihara H, Kajiura S, Ando T, Tajiri K, Fujinami H (2019) Management of remnant or recurrent lesions after endoscopic papillectomy. Clin Endosc 53(6):659–662
Rustagi T, Irani S, Reddy DN, Abu Dayyeh BK, Baron TH, Gostout CJ, Levy MJ, Martin J, Petersen BT, Ross A, Topazian MD (2017) Radiofrequency ablation for intraductal extension of ampullary neoplasms. Gastrointest Endosc 86:170–176
Camus M, Napoléon B, Vienne A, Le Rhun M, Leblanc S, Barret M, Chaussade S, Robin F, Kaddour N, Prat F (2018) Efficacy and safety of endobiliary radiofrequency ablation for the eradication of residual neoplasia after endoscopic papillectomy: a multicenter prospective study. Gastrointest Endosc 88:511–518
Sakai A, Tsujimae M, Masuda A, Iemoto T, Ashina S, Yamakawa K, Tanaka T, Tanaka S, Yamada Y, Nakano R, Sato Y, Kurosawa M, Ikegawa T, Fujigaki S, Kobayashi T, Shiomi H, Arisaka Y, Itoh T, Kodama Y (2019) Clinical outcomes of ampullary neoplasms in resected margin positive or uncertain cases after endoscopic papillectomy. World J Gastroenterol 25:1387–1397
Nam K, Song TJ, Kim RE, Cho DH, Cho MK, Oh D, Park DH, Lee SS, Seo DW, Lee SK, Kim MH, Baek S (2018) Usefulness of argon plasma coagulation ablation subsequent to endoscopic snare papillectomy for ampullary adenoma. Digest Endosc 30:485–492
Yang J, Han S, Zhou H, Lou Q, Zhang X, Shah RJ (2022) The efficacy and safety of endoscopic papillectomy combined with endobiliary radiofrequency ablation for ampullary neoplasms with intraductal biliary extension. Tech Innov Gastrointest Endosc 24:240–245
Lee R, Huelsen A, Gupta S, Hourigan LF (2020) Endoscopic ampullectomy for non-invasive ampullary lesions: a single-center 10-year retrospective cohort study. Surg Endosc 35:684–692
Irani S, Arai A, Ayub K, Biehl T, Brandabur JJ, Dorer R, Gluck M, Jiranek G, Patterson D, Schembre D, Traverso LW, Kozarek RA (2009) Papillectomy for ampullary neoplasm: results of a single referral center over a 10-year period. Gastrointest Endosc 70:923–932
Moekotte AL, Lof S, Van Roessel S, Fontana M, Dreyer S, Shablak A, Casciani F, Mavroeidis VK, Robinson S, Khalil K, Gradinariu G, Mowbray N, Al-Sarireh B, Fusai GK, Roberts K, White S, Soonawalla Z, Jamieson NB, Salvia R, Besselink MG, Abu Hilal M (2019) Histopathologic predictors of survival and recurrence in resected ampullary adenocarcinoma: international multicenter cohort study. Ann Surg 272(6):1086–1093
Schneider L, Contin P, Fritz S, Strobel O, Buchler MW, Hackert T (2016) Surgical ampullectomy: an underestimated operation in the era of endoscopy. HPB 18:65–71
Klein A, Qi Z, Bahin FF, Awadie H, Nayyar D, Ma M, Voermans RP, Williams SJ, Lee E, Bourke MJ (2018) Outcomes after endoscopic resection of large laterally spreading lesions of the papilla and conventional ampullary adenomas are equivalent. Endoscopy 50:972–983
Ridtitid W, Tan D, Schmidt SE, Fogel EL, McHenry L, Watkins JL, Lehman GA, Sherman S, Cote GA (2014) Endoscopic papillectomy: risk factors for incomplete resection and recurrence during long-term follow-up. Gastrointest Endosc 79:289–296
Syngal S, Brand RE, Church JM, Giardiello FM, Hampel HL, Burt RW (2015) ACG clinical guideline: genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol 110:223–262 (quiz 263)
Cotton PB, Eisen G, Romagnuolo J, Vargo J, Baron T, Tarnasky P, Schutz S, Jacobson B, Bott C, Petersen B (2011) Grading the complexity of endoscopic procedures: results of an ASGE working party. Gastrointest Endosc 73:868–874
Acknowledgements
This article is dedicated to the memory of Dr. Brian C. Brauer (1973-2019), MD, whose presence lives on in our efforts to mentor trainees, perform research, and advance the art of endoscopic practice.
Funding
NIH T32DK007038 (SH).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Raj Shah is an advisory board member and consultant for Boston Scientific and a consultant for Olympus and Cook Medical. Dr. Sachin Wani is an advisory board member for Cernostics, a consultant for Exact Sciences and Interpace, and has received research funding from Lucid, Ambu, and CDx. Dr. Steven Edmundowicz is an advisory board member for Olympus. Dr. Mihir Wagh is a consultant for Boston Scientific and Medtronic. Dr. Hazem Hammad is a consultant for Medtronic, Olympus, and Cook Medical. Dr. Samuel Han, Dr. Joshua Turkeltaub, Dr. Daniel Jonas, Dr. Augustin Attwell, and Dr. Anna Duloy have no conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Results of this paper were presented as an oral presentation at Digestive Disease Week.
Supplementary Information
Below is the link to the electronic supplementary material.
464_2023_10567_MOESM2_ESM.tif
Supplementary Figure 1: Serial endoscopic images of subject with early recurrence starting with A) initial ampullary adenoma, B) index papillectomy, C) surveillance exam after eradication achieved, and D) recurrence of lesion at 6-month post-eradication
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Han, S., Turkeltaub, J.A., Jonas, D. et al. The timing of recurrence after endoscopic papillectomy. Surg Endosc 38, 688–696 (2024). https://doi.org/10.1007/s00464-023-10567-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-023-10567-z