
Abstract
Introduction
A dilatation of the main pancreatic duct (MPD) is mainly due to obstructive causes (pancreatic tumor, chronic pancreatitis) or intraductal papillary mucinous neoplasm (IPMN). This study aims to assess the risk of pre-malignancy or malignancy in case of MPD dilatation with no visible mass nor obstructive calcification on computed tomography scan (CT-scan) in a population operated for it.
Patients and methods
All patients operated on from November 2015 to December 2019 in our center for a significant dilatation of the MPD without visible obstructive cause on CT-scan were included. Preoperative work-up included at least CT-scan, magnetic resonance imaging (MRI), and endoscopic ultrasonography (EUS). Primary endpoint was the final pathological diagnosis. Secondary endpoints were predictive factors of malignancy.
Results
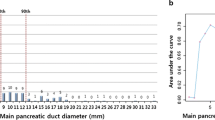
101 patients were included, mean age 68 years-old. Final pathological data were pancreatic adenocarcinoma (n = 2), IPMN with high-grade dysplasia (n = 37), high-grade Pancreatic Intraepithelial Neoplasia (PanIN) (n = 2) (total of pre-malignant or malignant lesions: n = 41), neuroendocrine tumor (n = 6), IPMN with low-grade dysplasia (n = 45), low-grade PanIN (n = 5), chronic pancreatitis (n = 3), and benign stenosis (n = 1). On preoperative explorations, the median diameter of MPD was 7 mm [3–35]. MRI and/or EUS showed intraductal material, nodule, or cyst in 22, 32, and 52 patients, respectively; 22 patients without nodule visible on MRI or EUS had still a pre-malignant or malignant lesion. In multivariate analysis, predictive factors for pre-malignancy or malignancy were symptoms before surgery (p = 0.01), MPD dilatation without downstream stenosis (p = 0.046), and the presence of nodule (p = 0.009).
Conclusion
A dilatation of the MPD without detectable mass or obstructive calcification on CT-scan was associated with a pre-malignant or malignant lesion in 41 patients. Symptoms before surgery, MPD dilatation without duct narrowing, and the presence of nodules on MRI/EUS were associated with the risk of pre-malignancy or malignancy.

Similar content being viewed by others


Abbreviations
- CH:
-
Contrast harmonic
- CI:
-
Confidence intervals
- CT-scan:
-
Computed tomography scan
- EUS:
-
Endoscopic ultrasonography
- FNA:
-
Fine-needle aspiration
- FNB:
-
Fine-needle biopsy
- HGD:
-
high-grade dysplasia
- HR:
-
Hazard ratios
- IPMN:
-
Intraductal papillary mucinous neoplasm LGD : low-grade dysplasia
- LGD:
-
low-grade dysplasia
- MPD:
-
Main pancreatic duct
- MRI:
-
Magnetic resonance imaging
- PanIN:
-
Pancreatic Intraepithelial Neoplasia
- SD:
-
Standard deviation
References
Tanaka M, Fernández-Del Castillo C, Kamisawa T, Jang JY, Levy P, Ohtsuka T et al (2017) Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 17(5):738–753
Del Chiaro M, Besselink M, Scholten L, Bruno MJ, Cahen DL, Gress TM et al (2018) European evidence-based guidelines on pancreatic cystic neoplasms. Gut 67(5):789–804
Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang J-Y et al (2012) International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 12(3):183–97
Canto MI, Almario JA, Schulick RD, Yeo CJ, Klein A, Blackford A et al (2018) Risk of neoplastic progression in individuals at high risk for pancreatic cancer undergoing long-term surveillance. Gastroenterology 155(3):740-751.e2
Basturk O, Hong S-M, Wood LD, Adsay NV, Albores-Saavedra J, Biankin AV et al (2015) A revised classification system and recommendations from the Baltimore consensus meeting for neoplastic precursor lesions in the pancreas. Am J Surg Pathol 39(12):1730–1741
Salvia R, Fernández-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W et al (2004) Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg 239(5):678–85 (discussion 685–687)
Miyasaka Y, Ohtsuka T, Matsuda R, Mori Y, Nakata K, Ohuchida K et al (2020) High-risk lesions in the remnant pancreas: fate of the remnant pancreas after pancreatic resection for pancreatic cancer and intraductal papillary mucinous neoplasms. Surg Today 50(8):832–840
van Roessel S, Kasumova GG, Verheij J, Najarian RM, Maggino L, de Pastena M et al (2018) International validation of the eighth edition of the American joint committee on cancer (AJCC) TNM staging system in patients with resected pancreatic cancer. JAMA Surg 153(12):e183617
Ohno E, Hirooka Y, Itoh A, Ishigami M, Katano Y, Ohmiya N et al (2009) Intraductal papillary mucinous neoplasms of the pancreas: differentiation of malignant and benign tumors by endoscopic ultrasound findings of mural nodules. Ann Surg 249(4):628–634
Tanaka M (2004) Intraductal papillary mucinous neoplasm of the pancreas: diagnosis and treatment. Pancreas 28(3):282–288
Ohtsuka T, Gotoh Y, Nakashima Y, Okayama Y, Nakamura S, Morita M et al (2018) Role of SpyGlass-DS(tm) in the preoperative assessment of pancreatic intraductal papillary mucinous neoplasm involving the main pancreatic duct. Pancreatology 18(5):566–71
Nagayoshi Y, Aso T, Ohtsuka T, Kono H, Ideno N, Igarashi H et al (2014) Peroral pancreatoscopy using the SpyGlass system for the assessment of intraductal papillary mucinous neoplasm of the pancreas. J Hepato-Biliary-Pancreat Sci 21(6):410–417
Mujica VR, Barkin JS, Go VL (2000) Acute pancreatitis secondary to pancreatic carcinoma. Study Group Participants. Pancreas 21(4):329–32
Falconi M, Eriksson B, Kaltsas G, Bartsch DK, Capdevila J, Caplin M et al (2016) ENETS consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non-functional pancreatic neuroendocrine tumors. Neuroendocrinology 103(2):153–171
Bagni K, Chen IM, Johansen AZ, Dehlendorff C, Jensen BV, Hansen CP et al (2020) Prognostic impact of Charlson’s Age-Comorbidity Index and other risk factors in patients with pancreatic cancer. Eur J Cancer Care 29(3):e13219
Vincent A, Herman J, Schulick R, Hruban RH, Goggins M (2011) Pancreatic cancer. The Lancet 378(9791):607–20
Acknowledgements
Guarantor of the article: Frédérique MAIRE, MD. All authors had access to the study data and reviewed and approved this final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Antoine Martin, Jérôme Cros, Marie-Pierre Vullierme, Safi Dokmak, Prs. Alain Sauvanet, Philippe Levy, Vinciane Rebours, and Dr. Frédérique Maire have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Martin, A., Cros, J., Vullierme, MP. et al. Dilatation of the main pancreatic duct of unknown origin: causes and risk factors of pre-malignancy or malignancy. Surg Endosc 37, 3684–3690 (2023). https://doi.org/10.1007/s00464-022-09854-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09854-y