
Abstract
Background
Benign esophageal strictures are a frequent complication after esophageal surgery or extensive endoscopic submucosal dissection. Endoscopic dilation is the preferred treatment in clinical practice. However, the allocation of time for each dilation is unclear. The aim of this study was to evaluate the appropriate duration of endoscopic dilation for benign esophageal strictures after esophageal surgery or endoscopic submucosal dissection.
Methods
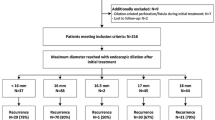
Patients with benign esophageal strictures after esophageal surgery or endoscopic submucosal dissection between July 2010 and July 2018 were retrospectively included in this study. According to the dilation time (1, 3, 5 min), patients were divided into three groups. The clinical effects and adverse events were compared among the three groups.
Results
Altogether, 57 patients, including 21 in the 1-min group, 18 in the 3-min group and 18 in the 5-min group, were included. All patients underwent endoscopic treatment successfully. The stricture recurrence rate was 76.19% in the 1-min group, 55.56% in the 3-min group and 61.11% in the 5-min group. The median overall dysphagia-free period was 2.60 (range, 0.80–12.00) months in the 1-min group, 6.60 (range, 1.80–12.00) months in the 3-min group and 6.25 (range, 2.40–12.00) months in the 5-min group (P < 0.05). For patients who developed stricture recurrence, the mean dysphagia-free periods were 2.26 ± 1.27 months, 4.00 ± 1.76 months and 4.23 ± 1.63 months, respectively (P < 0.05). The dysphagia-free periods were comparable between the 3- and 5-min groups and were longer than those in the 1-min group. Muscle layer damage occurred in two patients (11.11%) in the 5-min group and in no patients in the other two groups.
Conclusion
Three minutes was considered a safe and effective dilation duration for benign esophageal strictures after esophageal surgery or endoscopic submucosal dissection.

Similar content being viewed by others


References
Altintas E, Kacar S, Tunc B, Sezgin O, Parlak E, Altiparmak E, Saritas U, Sahin B (2004) Intralesional steroid injection in benign esophageal strictures resistant to bougie dilation. J Gastroenterol Hepatol 19:1388–1391
Haverkamp L, van der Sluis PC, Verhage RJ, Siersema PD, Ruurda JP, van Hillegersberg R (2013) End-to-end cervical esophagogastric anastomoses are associated with a higher number of strictures compared with end-to-side anastomoses. J Gastrointest Surg 17:872–876
van Heijl M, Gooszen JA, Fockens P, Busch OR, van Lanschot JJ, van Berge Henegouwen MI (2010) Risk factors for development of benign cervical strictures after esophagectomy. Ann Surg 251:1064–1069
Nederlof N, Tilanus HW, Tran TC, Hop WC, Wijnhoven BP, de Jonge J (2011) End-to-end versus end-to-side esophagogastrostomy after esophageal cancer resection: a prospective randomizedstudy. Ann Surg 254:226–233
Price TN, Nichols FC, Harmsen WS, Allen MS, Cassivi SD, Wigle DA, Shen KR, Deschamps C (2013) A comprehensive review of anastomotic technique in 432 esophagectomies. Ann Thorac Surg 95:1154–1160
Honda M, Kuriyama A, Noma H, Nunobe S, Furukawa TA (2013) Hand-sewn versus mechanical esophagogastric anastomosis after esophagectomy: a systematic review and meta-analysis. Ann Surg 257:238–248
Ono S, Fujishiro M, Niimi K, Goto O, Kodashima S, Yamamichi N, Omata M (2009) Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest Endosc 70:860–866
Saeed ZA, Winchester CB, Ferro PS, Michaletz PA, Schwartz JT, Graham DY (1995) Prospective randomized comparison of polyvinyl bougies and through-the-scope balloons for dilation of peptic strictures of the esophagus. Gastrointest Endosc 41:189–195
Scolapio JS, Pasha TM, Gostout CJ, Mahoney DW, Zinsmeister AR, Ott BJ, Lindor KD (1999) A randomized prospective study comparing rigid to balloon dilators for benign esophageal strictures and rings. Gastrointest Endosc 50:13–17
Cox JG, Winter RK, Maslin SC, Dakkak M, Jones R, Buckton GK, Hoare RC, Dyet JF, Bennett JR (1994) Balloon or bougie for dilatation of benign esophageal stricture? Dig Dis Sci 39:776–781
Hernandez LV, Jacobson JW, Harris MS (2000) Comparison among the perforation rates of Maloney, balloon, and Savary dilation of esophageal strictures. Gastrointest Endosc 51:460–462
Polese L, Angriman I, Bonello E, Erroi F, Scarpa M, Frego M, D’AmicoNorberto FL (2007) Endoscopic dilation of benign esophageal strictures in a surgical unit: a report on 95 cases. Surg Laparosc Endosc Percutan Tech 17:477–481
Egan JV, Baron TH, Adler DG, Davila R, Faigel DO, Gan SL, Hirota WK, Leighton JA, Lichtenstein D, Qureshi WA, Rajan E, Shen B, Zuckerman MJ, VanGuilder T, Fanelli RD, Standards of Practice C (2006) Esophageal dilation. Gastrointest Endosc 63:755–760
Zhang Y, Wang X, Liu L, Chen JP, Fan ZN (2015) Intramuscular injection of mitomycin C combined with endoscopic dilation for benign esophageal strictures. J Dig Dis 16:370–376
Ogilvie AL, Dronfield MW, Ferguson R, Atkinson M (1982) Palliative intubation of oesophagogastric neoplasms at fibreoptic endoscopy. Gut 23:1060–1067
van Halsema EE, Noordzij IC, van Berge Henegouwen MI, Fockens P, Bergman JJ, van Hooft JE (2017) Endoscopic dilation of benign esophageal anastomotic strictures over 16 mm has a longer lasting effect. Surg Endosc 31:1871–1881
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394–424
Lew R, Kochman M (2002) A review of endoscopic methods of esophageal dilation. J Clin Gastroenterol 35:117–126
Walter B, Schmidbaur S, Rahman I, Albers D, Schumacher B, Meining A (2019) The BougieCap - a new method for endoscopic treatment of complex benign esophageal stenosis: results from a multicenter study. Endoscopy 51:866–870
Bi Y, Ren J, Li J, Yu Z, Han X, Wu G (2019) A novel fully covered self-expandable segmental metallic stents for the treatment of refractory esophageal stenosis. J Thorac Dis 11:1363–1369
Minamino H, Machida H, Tominaga K, Sugimori S, Okazaki H, Tanigawa T, Yamagami H, Watanabe K, Watanabe T, Fujiwara Y, Arakawa T (2013) Endoscopic radial incision and cutting method for refractory esophageal stricture after endoscopic submucosal dissection of superficial esophageal carcinoma. Dig Endosc 25:200–203
Ikeya T, Ohwada S, Ogawa T, Tanahashi Y, Takeyoshi I, Koyama T, Morishita Y (1999) Endoscopic balloon dilation for benign esophageal anastomotic stricture: factors influencing its effectiveness. Hepatogastroenterology 46:959–966
Mendelson AH, Small AJ, Agarwalla A, Scott FI, Kochman ML (2015) Esophageal anastomotic strictures: outcomes of endoscopic dilation, risk of recurrence and refractory stenosis, and effect of foreign body removal. Clin Gastroenterol Hepatol 13:263–271
Park JY, Song HY, Kim JH, Park JH, Na HK, Kim YH, Park SI (2012) Benign anastomotic strictures after esophagectomy: long-term effectiveness of balloon dilation and factors affecting recurrence in 155 patients. AJR Am J Roentgenol 198:1208–1213
Lian JJ, Ma LL, Hu JW, Chen SY, Qin WZ, Xu MD, Zhou PH, Yao LQ (2014) Endoscopic balloon dilatation for benign esophageal stricture after endoscopic submucosal dissection for early esophageal neoplasms. J Dig Dis 15:224–229
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Jiankun Wang, Lili Zhao, Rui Wu, Min Wang, Li Liu, Xiang Wang, Wenjie Liu, Kexin He, Lin Miao and Zhining Fan declare that they have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, J., Zhao, L., Wu, R. et al. Appropriate duration of endoscopic dilation for postoperative benign esophageal strictures. Surg Endosc 36, 1263–1268 (2022). https://doi.org/10.1007/s00464-021-08400-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-021-08400-6