
Abstract
Objectives
Adenocarcinoma of the esophagogastric junction (AEG) is one of the most aggressive and poor prognosis cancers. To date, no standard procedures have been established for the surgical treatment of Siewert type II. In this study, we proposed the approach of thoracoscopic-laparoscopic Ivor-Lewis surgery plus D2 celiac lymphadenectomy (TLILD2) and aimed to investigate the patterns of lymph node metastasis and long-term survival.
Methods
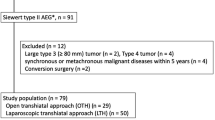
From June 2015 to June 2018, 72 patients accepted TLILD2 and enrolled in this study. Relevant patient characteristics and postoperative variables were collected and evaluated. The disease-free survival (DFS) and disease-specific survival (DSS) were determined by the Kaplan–Meier method and compared by log-rank tests.
Results
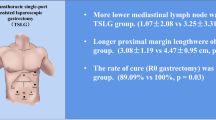
There was no case of postoperative death in this study, and the most common complication was anastomotic mediastinal fistula (5/72, 6.9%). A total of 2811 lymph nodes were retrieved, and the positivity rate was 11.9% (334/2811). The positivity rate of celiac and mediastinal lymph nodes was 14.4% (314/2186) and 3.2% (20/625), respectively. The percentage of patients who had positive celiac and mediastinal lymph nodes reached up to 58.3% (42/72) and 8.3% (6/72), respectively. The DFS and DSS of these 72 patients were 94% and 93.4% at 1 year after surgery and 59.8% and 62% at 3 years after surgery, respectively. The pTNM stage showed a significant difference between DFS and DSS.
Conclusions
TLILD2 could be a potential way to promote long-term survival of AEG patients. On the basis of the patterns of lymph nodes metastasis, we suggest that lower mediastinal and D2 celiac lymphadenectomy is necessary to improve the oncological outcome.




Similar content being viewed by others

References
Liu K, Yang K, Zhang W, Chen X, Chen X, Zhang B, Chen Z, Chen J, Zhao Y, Zhou Z, Chen L, Hu J (2016) Changes of esophagogastric junctional adenocarcinoma and gastroesophageal reflux disease among surgical patients during 1988–2012: a single-institution, high-volume experience in China. Ann Surg 263:88–95
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394–424
Rudiger SJ, Feith M, Werner M, Stein HJ (2000) Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg 232:353–361
Hasegawa S, Yoshikawa T (2010) Adenocarcinoma of the esophagogastric junction: incidence, characteristics, and treatment strategies. Gastric Cancer 13:63–73
Derakhshan MH, Malekzadeh R, Watabe H, Yazdanbod A, Fyfe V, Kazemi A, Rakhshani N, Didevar R, Sotoudeh M, Zolfeghari AA, McColl KE (2008) Combination of gastric atrophy, reflux symptoms and histological subtype indicates two distinct aetiologies of gastric cardia cancer. Gut 57:298–305
Hansen S, Vollset SE, Derakhshan MH, Fyfe V, Melby KK, Aase S, Jellum E, McColl KE (2007) Two distinct aetiologies of cardia cancer; evidence from premorbid serological markers of gastric atrophy and helicobacter pylori status. Gut 56:918–925
Heger P, Blank S, Goossen K, Nienhuser H, Diener MK, Ulrich A, Mihaljevic AL, Schmidt T (2019) Thoracoabdominal versus transhiatal surgical approaches for adenocarcinoma of the esophagogastric junction-a systematic review and meta-analysis. Langenbecks Arch Surg 404(1):103–113
Aurello P, Magistri P, Berardi G, Petrucciani N, Sirimarco D, Antolino L, Nigri G, D’Angelo F, Ramacciato G (2016) Transthoracically or transabdominally: how to approach adenocarcinoma of the distal esophagus and cardia. A meta-analysis. Tumori J 102:352–360
Brown AM, Giugliano DN, Berger AC, Pucci MJ, Palazzo F (2017) Surgical approaches to adenocarcinoma of the gastroesophageal junction: the Siewert II conundrum. Langenbecks Arch Surg 402:1153–1158
Fuchs H, Holscher AH, Leers J, Bludau M, Brinkmann S, Schroder W, Alakus H, Monig S, Gutschow CA (2016) Long-term quality of life after surgery for adenocarcinoma of the esophagogastric junction: extended gastrectomy or transthoracic esophagectomy? Gastric Cancer 19:312–317
Pedrazzani C, de Manzoni G, Marrelli D, Giacopuzzi S, Corso G, Minicozzi AM, Rampone B, Roviello F (2007) Lymph node involvement in advanced gastroesophageal junction adenocarcinoma. J Thorac Cardiovasc Surg 134:378–385
Goto H, Tokunaga M, Miki Y, Makuuchi R, Sugisawa N, Tanizawa Y, Bando E, Kawamura T, Niihara M, Tsubosa Y, Terashima M (2014) The optimal extent of lymph node dissection for adenocarcinoma of the esophagogastric junction differs between Siewert type II and Siewert type III patients. Gastric Cancer 18(2):375–381
Nunobe S, Ohyama S, Sonoo H, Hiki N, Fukunaga T, Seto Y, Yamaguchi T (2008) Benefit of mediastinal and para-aortic lymph-node dissection for advanced gastric cancer with esophageal invasion. J Surg Oncol 97:392–395
Blank S, Schmidt T, Heger P, Strowitzki MJ, Sisic L, Heger U, Nienhueser H, Haag GM, Bruckner T, Mihaljevic AL, Ott K, Buchler MW, Ulrich A (2018) Surgical strategies in true adenocarcinoma of the esophagogastric junction (AEG II): thoracoabdominal or abdominal approach? Gastric Cancer 21:303–314
Japanese Gastric Cancer Association (2017) Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 20:1–19
Rice TW, Ishwaran H, Ferguson MK, Blackstone EH, Goldstraw P (2017) Cancer of the esophagus and esophagogastric junction: an eighth edition staging primer. J Thorac Oncol 12:36–42
Inaba K, Satoh S, Ishida Y, Taniguchi K, Isogaki J, Kanaya S, Uyama I (2010) Overlap method: novel intracorporeal esophagojejunostomy after laparoscopic total gastrectomy. J Am Coll Surg 211:e25–e29
Parry K, Haverkamp L, Bruijnen RC, Siersema PD, Ruurda JP, van Hillegersberg R (2015) Surgical treatment of adenocarcinomas of the gastro-esophageal junction. Ann Surg Oncol 22:597–603
Kurokawa Y, Sasako M, Sano T, Yoshikawa T, Iwasaki Y, Nashimoto A, Ito S, Kurita A, Mizusawa J, Nakamura K (2015) Ten-year follow-up results of a randomized clinical trial comparing left thoracoabdominal and abdominal transhiatal approaches to total gastrectomy for adenocarcinoma of the oesophagogastric junction or gastric cardia. Br J Surg 102:341–348
Siewert JR, Feith M (2007) Adenocarcinoma of the esophagogastric junction: competition between Barrett and gastric cancer. J Am Coll Surg 205:S49–S53
Hasegawa S, Yoshikawa T, Cho H, Tsuburaya A, Kobayashi O (2009) Is adenocarcinoma of the esophagogastric junction different between Japan and western countries? The incidence and clinicopathological features at a Japanese high-volume cancer center. World J Surg 33:95–103
Yabusaki H, Nashimoto A, Matsuki A, Aizawa M (2014) Comparison of the surgical treatment strategies for Siewert type II squamous cell carcinoma in the same area as esophagogastric junction carcinoma: data from a single Japanese high-volume cancer center. Surg Today 44:1522–1528
Yura M, Takeuchi H, Fukuda K, Nakamura R, Suda K, Wada N, Kawakubo H, Kitagawa Y (2018) High-risk group of upper and middle mediastinal lymph node metastasis in patients with esophagogastric junction carcinoma. Ann Gastroenterol Surg 2:419–427
Suh YS, Lee KG, Oh SY, Kong SH, Lee HJ, Kim WH, Yang HK (2017) Recurrence pattern and lymph node metastasis of adenocarcinoma at the esophagogastric junction. Ann Surg Oncol 24:3631–3639
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Kun-Kun Li, Tao Bao, Ying-Jian Wang, Xue-Hai Liu, and Wei Guo have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, KK., Bao, T., Wang, YJ. et al. The Postoperative outcomes of thoracoscopic-laparoscopic Ivor-Lewis surgery plus D2 celiac lymphadenectomy for patients with adenocarcinoma of the esophagogastric junction. Surg Endosc 34, 4957–4966 (2020). https://doi.org/10.1007/s00464-019-07288-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07288-7