
Abstract
Background
Despite increases in the performance of pure laparoscopic living donor hepatectomy, variations in the bile duct or portal vein have been regarded as relative contraindications to this technique [1,2,3]. This report describes a donor with separate right posterior and right anterior hepatic ducts and portal veins who underwent pure laparoscopic living donor right hemihepatectomy, integrated with 3D laparoscopy and indocyanine green (ICG) near-infrared fluorescence cholangiography [1, 4, 5].
Methods
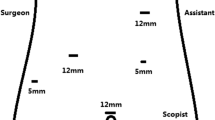
A 50-year-old man offered to donate part of his liver to his older brother, who required a transplant for hepatitis B-associated liver cirrhosis and hepatocellular carcinoma. Donor height was 178.0 cm, body weight was 82.7 kg, and body mass index was 26.1 kg/m2. Preoperative computed tomography and magnetic resonance cholangiopancreatography showed that the donor had separate right posterior and right anterior hepatic ducts and portal veins. The entire procedure was performed under 3D laparoscopic view. Following intravenous injections of 0.05 mg/kg ICG, ICG near-infrared fluorescence camera was used to demarcate the exact transection line and determine the optimal bile duct division point.
Results
The total operation time was 443 min; the donor required no transfusions and experienced no intraoperative complications. The graft weighed 1146 g with a graft-to-recipient weight ratio of 1.88%. The optimal bile duct division point was identified using ICG fluorescence cholangiography, and the bile duct was divided with good patency without any stricture. The right anterior and posterior portal veins were transected with endostaplers without any torsion. The patient was discharged on postoperative day 8, with no complications.
Conclusion
Using a 3D view and ICG fluorescence cholangiography, pure 3D laparoscopic living donor right hemihepatectomy is feasible in a donor with separate right posterior and right anterior hepatic ducts and portal veins.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Suh KS, Hong SK, Yi NJ, Lee KW, Kim HS, Yoon KC et al (2016) Pure 3-dimensional laparoscopic extended right hepatectomy in a living donor. Liver Transpl 22:1431–1436
Soubrane O, Perdigao Cotta F, Scatton O (2013) Pure laparoscopic right hepatectomy in a living donor. Am J Transplant 13:2467–2471
Han HS, Cho JY, Yoon YS, Hwang DW, Kim YK, Shin HK et al (2015) Total laparoscopic living donor right hepatectomy. Surg Endosc 29:184
Velayutham V, Fuks D, Nomi T, Kawaguchi Y, Gayet B (2016) 3D visualization reduces operating time when compared to high-definition 2D in laparoscopic liver resection: a case-matched study. Surg Endosc 30:147–153
Mizuno S, Isaji S (2010) Indocyanine green (ICG) fluorescence imaging-guided cholangiography for donor hepatectomy in living donor liver transplantation. Am J Transplant 10:2725–2726
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 1 (WMV 175649 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hong, S.K., Suh, KS., Kim, HS. et al. Pure 3D laparoscopic living donor right hemihepatectomy in a donor with separate right posterior and right anterior hepatic ducts and portal veins. Surg Endosc 31, 4834–4835 (2017). https://doi.org/10.1007/s00464-017-5535-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5535-8