
Abstract
Background
Benign anastomotic colonic stenosis sometimes occur after surgery and usually require surgical or endoscopic dilation. Endoscopic dilation of anastomotic colonic strictures by using balloon or bougie-type dilators has been demonstrated to be safe and effective in multiple uncontrolled series. However, few data are available on safety and efficacy of endoscopic electrocautery dilation. The aim of our study was to retrospectively investigate safety and efficacy of endoscopic electrocautery dilation of postsurgical benign anastomotic colonic strictures.
Methods
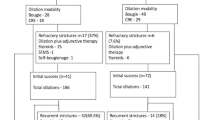
Sixty patients (37 women; median age 63.6 years, range 22.6–81.7) with benign anastomotic colonic or rectal strictures treated with endoscopic electrocautery dilation between June 2001 and February 2013 were included in the study. Anastomotic stricture was defined as a narrowed anastomosis through which a standard colonoscope could not be passed. Only annular anastomotic strictures were considered suitable for electrocautery dilation which consisted of radial incisions performed with a precut sphincterotome. Treatment was considered successful if the colonic anastomosis could be passed by a standard colonoscope immediately after dilation. Recurrence was defined as anastomotic stricture reappearance during follow-up.
Results
The time interval between colorectal surgery and the first endoscopic evaluation or symptoms development was 7.3 months (1.3–60.7). Electrocautery dilation was successful in all the patients. There were no procedure-related complications. Median follow-up was 35.5 months (2.0–144.0). Anastomotic stricture recurrence was observed in three patients who were successfully treated with electrocautery dilation and Savary dilation.
Conclusions
Endoscopic electrocautery dilation is a safe and effective treatment for annular benign anastomotic postsurgical colonic strictures.



Similar content being viewed by others


References
Luchtefeld AM, Milsom JW, Senagore A, Surrell JA, Mazier WP (1989) Colorectal anastomotic stenosis: results of a survey of the ASCRS membership. Dis Colon Rectum 32:733–736
Irvin TT, Goligher JC (1973) Aetiology of disruption of intestinal anastomoses. Br J Surg 60:461–464
Morgenstern L (1981) The intestinal anastomosis with the end-to-end stapling instrument. Progress and problems, 1980. Arch Surg 166:141–142
Waxman BP (1983) Large bowel anastomoses. II. The circular staplers. Br J Surg 70:64–67
Araujo SE, Furtado Costa A (2008) Efficacy and safety of endoscopic balloon dilation of benign anastomotic strictures after oncologic anterior rectal resection. Report on 24 cases. Surg Laparosc Endosc Percutaneous Tech 18:565–568
Belvedere B, Frattaroli S, Crabone A, Viceconte G (2012) Anastomotic strictures in colorectal surgery: treatment with endoscopic balloon dilation. G Chir 33:243–245
Werre A, Mulder C, van Heteren C, Bilgen ES (2000) Dilation of benign strictures following low anterior resection using Savary–Gilliard bougies. Endoscopy 32(5):385–388
Brandimarte G, Tursi A, Gasbarrini G (2000) Endoscopic treatment of benign anastomotic colorectal stenosis with electrocautery. Endoscopy 32(6):461–463
Polese L, Vecchiato M, Frigo AC, Sarzo G, Cadrobbi R, Rizzato R, Bressan A, Merigliano S (2012) Risk factors for colorectal anastomotic stenoses and their impact on quality of life: what are the lessons to learn? Colorectal Dis 14(3):e124–e128
Bouvier AM, Latournerie M, Jooste V, Lepage C, Cottet V, Faivre J (2008) The lifelong risk of metachronous colorectal cancer justifies long-term colonoscopic follow-up. Eur J Cancer 44:522–527
Schlegel RD, Dheni N, Parc R, Caplin S, Tiret E (2001) Results of reoperations in colorectal anastomotic strictures. Dis Colon Rectum 44:146–148
Pietropaolo V, Masoni L, Ferrara M, Montori A (1990) Endoscopic dilation of colonic postoperative strictures. Surg Endosc 4:26–30
Disclosures
Drs. Ivana Bravi, Davide Ravizza, Giancarla Fiori, Darina Tamayo, Cristina Trovato, Giuseppe De Roberto and Chiara Genco have no conflicts of interest or financial ties to disclose. Dr. Crosta is consultant and teacher of Pentax Education Center in Milan. The European Institute of Oncology receives an unrestricted grant by Pentax Italia to undertake research activities and training programs.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bravi, I., Ravizza, D., Fiori, G. et al. Endoscopic electrocautery dilation of benign anastomotic colonic strictures: a single-center experience. Surg Endosc 30, 229–232 (2016). https://doi.org/10.1007/s00464-015-4191-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4191-0