
Abstract
Background
Traditionally, splenectomy is considered as the treatment for splenic lesions. The risk of early and late complications and the awareness of immunologic function of spleen have pushed the development of spleen sparing techniques. This study aimed to evaluate the safety and feasibility of laparoscopic partial splenectomy in selected patients.
Methods
From May 2011 we initiated performing laparoscopic partial splenectomy in patients with focal benign splenic lesion. The main surgical procedure consisted of four steps: 1. Mobilizing the perisplenic ligaments. 2. Ligating and dissecting the vessels which supplying the involved spleen. 3. Dissecting the spleen along the demarcation. 4. Hemostasis was achieved by bipolar energy device. The perioperative data were collected and analyzed. The follow-up including quality of life and splenic regrowth was routinely undergone 6 months after surgery.
Results
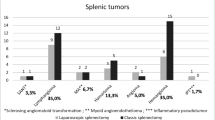
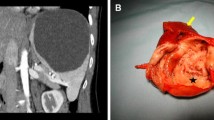
From May 2011 to December 2013, laparoscopic partial splenectomy had been performed on 11 patients aged from 13 to 57 (mean 33). The indications included nonparasitic cyst (n = 6), lymphangioma (n = 3), and hemangioma (n = 2). The mean operative time was 148 min (range 110–200 min). The mean estimated blood loss was 189 ml (range 100–400 ml). One patient converted to total splenectomy because of hemorrhaging. Two patients suffered from postoperative complications: the one who converted to total splenectomy suffered from portal vein thrombosis, the other one underwent partial splenectomy suffered from fluid collection around splenic recess. There was no blood transfusion and postoperative mortality. All patients discharged uneventfully. Seven patients finished the follow-up including evaluation of CT scan and quality of life 6 month after surgery. The results demonstrated all these patients had different degree of splenic regrowth and gained a good quality of life.
Conclusions
Laparoscopic partial splenectomy is safe and effective in patients with focal benign splenic lesion. Meanwhile, this technique potentially retains some splenic function, and confers the benefit of a minimal access technique.



Similar content being viewed by others

References
Wolf HM, Eibl MM, Georgi E, Samstag A, Spatz M, Uranus S, Passl R (1999) Long-term decrease of CD4+CD45RA+T cells and impaired primary immune response after post-traumatic splenectomy. Br J Haematol 107:55–68
Hansen K, Singer DB (2001) Asplenic-hyposplenic overwhelming sepsis: postsplenectomy sepsis revisited. Pediatr Dev Pathol 4:105–121
Tracy ET, Haas KM, Gentry T, Danko M, Roberts JL, Kurtzberg J, Rice HE (2011) Partial splenectomy but not total splenectomy preserves immunoglobulin M memory B cells in mice. J Pediatr Surg 46:1706–1710
Gumbs AA, Bouhanna P, Bar-Zakai B, Briennon X, Gayet B (2008) Laparoscopic partial splenectomy using radiofrequency ablation. J Laparoendosc Adv Surg Tech A 18:611–613
Uranues S, Grossman D, Ludwig L, Bergamaschi R (2007) Laparoscopic partial splenectomy. Surg Endosc 21:57–60
Delaitre B, Maignien B, Icard P (1992) Laparoscopic splenectomy. Br J Surg 79:1334
McHorney CA, Ware JE Jr, Raczek AE (1993) The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care 31:247–263
Li J, Liu C, Li N, He T, Li B (2001) Scaling the SF-36 in a Chinese population. Hua Xi Yi Ke Da Xue Xue Bao 32(36–38):47
Yu J, Coons SJ, Draugalis JR, Ren XS, Hays RD (2003) Equivalence of Chinese and US-English versions of the SF-36 health survey. Qual Life Res 12:449–457
Lynch AM, Kapila R (1996) Overwhelming postsplenectomy infection. Infect Dis Clin N Am 10:693–707
Robinette CD, Fraumeni JF Jr (1977) Splenectomy and subsequent mortality in veterans of the 1939–1945 war. Lancet 2:127–129
Schilling RF (1997) Spherocytosis, splenectomy, strokes, and heat attacks. Lancet 350:1677–1678
Mackenzie RK, Youngson GG, Mahomed AA (2004) Laparoscopic decapsulation of congenital splenic cysts: a step forward in splenic preservation. J Pediatr Surg 39:88–90
Schier F, Waag KL, Ure B (2007) Laparoscopic unroofing of splenic cysts results in a high rate of recurrences. J Pediatr Surg 42:1860–1863
Westermann J, Pabst R (1986) Autotransplantation of splenic fragments: lymphocyte subsets in blood, lymph nodes and splenic tissue. Clin Exp Immunol 64:188–194
Malangoni MA, Evers BM, Peyton JC, Wellhausen SR (1988) Reticuloendothelial clearance and splenic mononuclear cell populations after resection and autotransplantation. Am J Surg 155:298–302
Buesing KL, Tracy ET, Kiernan C, Pastor AC, Cassidy LD, Scott JP, Ware RE, Davidoff AM, Rescorla FJ, Langer JC, Rice HE, Oldham KT (2011) Partial splenectomy for hereditary spherocytosis: a multi-institutional review. J Pediatr Surg 46:178–183
Hery G, Becmeur F, Mefat L, Kalfa D, Lutz P, Lutz L, Guys JM, de Lagausie P (2008) Laparoscopic partial splenectomy: indications and results of a multicenter retrospective study. Surg Endosc 22:45–49
Liu DL, Xia S, Xu W, Ye Q, Gao Y, Qian J (1996) Anatomy of vasculature of 850 spleen specimens and its application in partial splenectomy. Surgery 119:27–33
Okano K, Kakinoki K, Suto H, Oshima M, Akamoto S, Hagiike M, Usuki H, Suzuki Y (2011) Hand-assisted laparoscopic partial splenectomy using an endopath monopolar sealer. Surg Laparosc Endosc Percutan Tech 21:e291–e294
Giulianotti PC, Buchs NC, Addeo P, Ayloo S, Bianco FM (2011) Robot-assisted partial and total splenectomy. Int J Med Robot 7:482–488
Khelif K, Maassarani F, Dassonville M, Laet MH (2006) Laparoscopic partial splenectomy using radiofrequency ablation for nonparasitic splenic cysts in two children. J Laparoendosc Adv Surg Tech A 16:414–417
Zacharoulis D, Katsogridakis E, Hatzitheofilou C (2006) A case of splenic abscess after radiofrequency ablation. World J Gastroenterol 12:4256–4258
Patrzyk M, Glitsch A, Hoene A, von Bernstorff W, Heidecke CD (2011) Laparoscopic partial splenectomy using a detachable clamp with and without partial splenic embolisation. Langenbecks Arch Surg 396:397–402
Bader-Meunier B, Gauthier F, Archambaud F, Cynober T, Mielot F, Dommergues JP, Warszawski J, Mohandas N, Tchernia G (2001) Long-term evaluation of the beneficial effect of subtotal splenectomy for management of hereditary spherocytosis. Blood 97:399–403
Goldthorn JF, Schwartz AD, Swift AJ, Winkelstein JA (1978) Protective effect of residual splenic tissue after subtotal splenectomy. J Pediatr Surg 13:587–590
Slater BJ, Chan FP, Davis K, Dutta S (2010) Institutional experience with laparoscopic partial splenectomy for hereditary spherocytosis. J Pediatr Surg 45:1682–1686
Morinis J, Dutta S, Blanchette V, Butchart S, Langer JC (2008) Laparoscopic partial vs total splenectomy in children with hereditary spherocytosis. J Pediatr Surg 43:1649–1652
Acknowledgments
This study was granted by the West China Hospital, Sichuan University.
Disclosure
Xin Wang, Mingjun Wang, Hua Zhang, and Bing Peng have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Wang, X., Wang, M., Zhang, H. et al. Laparoscopic partial splenectomy is safe and effective in patients with focal benign splenic lesion. Surg Endosc 28, 3273–3278 (2014). https://doi.org/10.1007/s00464-014-3600-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3600-0