
Abstract
Background
To improve endoscopic surgical skills, an increasing number of surgical residents practice on box or virtual-reality (VR) trainers. Current training is mainly focused on hand–eye coordination. Training methods that focus on applying the right amount of force are not yet available.
Methods
The aim of this project is to develop a system to measure forces and torques during laparoscopic training tasks as well as the development of force parameters that assess tissue manipulation tasks. The force and torque measurement range of the developed force platform are 0–4 N and 1 Nm (torque), respectively. To show the potential of the developed force platform, a pilot study was conducted in which five surgeons experienced in intracorporeal suturing and five novices performed a suture task in a box trainer.
Results
During the pilot study, the maximum and mean absolute nonzero force that the novice used were 4.7 N (SD 1.3 N) and 2.1 N (SD 0.6 N), respectively. With a maximum force of 2.6 N (SD 0.4 N) and mean nonzero force of 0.9 N (SD 0.3 N), the force exerted by the experts was significantly lower.
Conclusions
The designed platform is easy to build, affordable, and accurate and sensitive enough to reflect the most important differences in, e.g., maximal force, mean force, and standard deviation. Furthermore, the compact design makes it possible to use the force platform in most box trainers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Use of minimally invasive techniques in medicine is rapidly increasing and offers the patient many advantages compared with open surgery. Because of the increasing complexity of minimally invasive procedures, effective and affordable training tools are required to improve the endoscopic skills of surgical trainees. New training tools such as box trainers equipped with motion detection [1, 2] or virtual-reality trainers [3, 4] have been developed to enable trainees to practice outside the operation room and to objectively assess their skills. Current assessment focuses mainly on efficiency of instrument movements and task (completion) time in basic grasping and positioning tasks. However, there is also a need for objective assessment of performance in delicate tasks such as tissue handling and suturing [5, 6]. During these tasks high forces can cause serious tissue damage, therefore monitoring other parameters (i.e., the interaction force between tools and tissue) is essential for proper assessment of endoscopic skills. When box trainers are equipped with force-sensing technology, information about interaction force and torque can be used to train delicate tasks that require adequate force control. If trainees use these training tasks and assessment methods to train tissue-handling skills in a laboratory setting before operating on a patient, the risks of tissue damage can be reduced. The present research consists of two parts. The first objective is to develop a simple and low-cost force platform system that measures force and torque applied on tissue with standard laparoscopic tools inside a standard box trainer. The second objective is to illustrate the potential of the developed platform by measuring the difference in performance of one novice and one expert during a simple needle-driving task.
Requirements
The design of a platform that measures forces and moments generated between instruments and tissue, should meet the following requirements:
-
1.
Measurement of forces in three directions (X, Y, Z);
-
2.
Measurement of moments around the X, Y, and Z axes;
-
3.
Device fits in different standard box trainers with minimal modifications of the training setup;
-
4.
Multiple training tasks can be trained with the device;
-
5.
Plug and play, and compatible with all standard computer operating systems;
-
6.
Low cost, robust, and easy to assemble;
-
7.
Accuracy of ±10%;
-
8.
Able to measure frequencies up to 20 Hz [7];
-
9.
Force and torque range should be adjustable for different trainings tasks;
-
10.
The platform must be able to measure forces and torques up to 12 N and 0.7 Nm [8–11], respectively.
Based on these requirements, a prototype was made that makes use of a commercially available six-dimensional (6D) mouse (SpaceNavigator; 3Dconnexion GmbH, Seefeld, Germany). This mouse is typically used to move objects in a three-dimensional virtual environment. The potential of the prototype for performance evaluation in laparoscopic tasks was investigated in a pilot study.
Optoelectronic 6D mouse
The SpaceNavigator is a USB device that can be read with standard communication protocols as used by Windows®. In Fig. 1, a schematic exploded view of the SpaceNavigator itself is presented. Relative movements and position of the table are determined by optoelectronic components installed inside the SpaceNavigator. Basically, three bundles of infrared light are created by three pairs of light-emitting diodes (LEDs) mounted on a printed circuit board (PCB) (1). With a triangular plastic block (2) with slit diagraph (3), placed over the LEDs (4), the three bundles are reshaped into 3 × 2 light paths. The light paths are detected by three light-detecting components (8), installed on a second PCB (5). Both PCBs are connected by small springs (6) that allow independent movement in all directions.

Schematic exploded view of the SpaceNavigator (adapted from patent EP1850210)
Materials and methods
Software
Software was written in C++ to record rotation and translation vectors at a rate of 60 Hz (Fig. 3). The data were saved in arbitrary units together with a time vector. To compute the force in Newton and torque in newton millimeter for further analysis, the relationship between the measurements and the applied forces was determined by calibrating the force platform.
Mechanical components
To use the SpaceNavigator as a 6D force platform in box trainers, the allowable range of forces needs to be increased. Increased stiffness in all directions is required to measure forces over 2 N without limiting the movement of the cap. This is accomplished by adding three springs around the SpaceNavigator (Fig. 2). On one side the springs are connected to the table (i.e., the upper plate) that is mounted on the cap of the SpaceNavigator. On the other side, the springs are connected to a base plate fixed on the housing of the SpaceNavigator. Small adjustments in the position and orientation of all individual springs, with respect to the base plate and table, are possible by repositioning of the spring holders with the three star screws at the top and three Allen screws at the base plate (Fig. 3). If springs with stiffness of 14 N/mm are used, a force range of 12 N is easily reached. For the first needle-driving tests a lower force range of 6 N is sufficient. Therefore, springs with 4 N/mm stiffness were used to maximize resolution.

Left: force platform built from mechanical components. Right: modified SpaceNavigator that is fixed between base plate and table

Vector representation of example nonselective manipulation
Calibration
Calibration was accomplished with standardized weights of 50, 100, 250, and 500 g. A frame was built from mechanical components to exert well-defined forces and torques, in all directions, at the center of the platform table. During the force calibration of each axis, the load on the platform was increased from −650 to 650 g in steps of 50 g. The torque on the platform was increased from −1.08 to 1.08 Nm in steps of 98.1 × 10−3 Nm. Each axis was calibrated three times. After calibration, regression lines were added to the platform output data of each individual axis.
Accuracy
The forces applied during calibration result in force and torque vectors with components in three orthogonal axes (X, Y, and Z). During calibration, the output error is determined for every individual axis. However, if the force or torque vector is spanned between two or three axes, each individual translation along, or rotation around, one axis can influence the force–output or torque–output relation of the other axis. To determine a general value for the accuracy of the platform, a series of tests were conducted. During the first test series, three different forces of 0.981, 1.962, and 2.943 N were exerted in line with the eight direction vectors (Fig. 4, Q1 to Q8). During the second test series, three different torque values of 0.384, 0.256, and 0.28 Nm were exerted around the eight direction vectors (Q1 to Q8). During both tests, each measurement was repeated three times.

Direction of applied force and torque during testing
Pilot study: needle-driving task
A pilot study in which subjects performed a needle-driving task was undertaken to investigate the potential of the force platform. The task was conducted inside a training box (Fig. 5, right) equipped with two 5-mm and one 11-mm trocars (Endopath XCEL; Johnson & Johnson), two needle drivers (B Braun), and one laparoscopic camera. Artificial tissue, imitating skin and fat layers (Professional Skin Pad, Mk 2; Limbs & Things, Bristol, UK), was fixed on the force platform. On top of the artificial tissue, the point of insertion and direction were marked by two lines (Fig. 5, left). The line thickness was 2 mm, and the distance between the two lines was 9 mm. The test group (n = 10) consisted of five surgeons who had performed at least 50 laparoscopic sutures during surgery and five novices without hands-on experience in laparoscopic surgery or training. All subjects were asked to pick up a needle (Vicryl 3–0 SH plus 26 mm; Ethicon, Johnson & Johnson) with the needle driver and to insert it at the right line on the tissue. Secondly, the subjects were asked to drive the needle, in the desired direction, through the tissue and to remove it completely at the location of the left line. If a subject was not able to insert the needle at the right line or to remove it at the left line, the measurement was removed from the database and the subject was asked to try it again. All subjects were asked to complete the needle-driving task two times. During the test, no feedback was given to the subjects. For each subject we determined the maximum absolute force and the mean absolute nonzero force. We defined the mean absolute nonzero force as the force averaged across all samples during which force was exerted so that the resulting measure is based only on the periods of time when interaction took place. To determine whether the results obtained for the experienced surgeons differed from the data from the novices we performed Student’s t-tests (SPSS 17.0) to compare group means. Also, striking differences in force signatures were further investigated. In addition, we asked one novice and one expert to perform the needle-driving task four times instead of two. This was done to see if learning effects occurred within a small number of repetitions.

Left: force platform with artificial skin tissue. Right: test setup with box trainer, trocars, laparoscope, needle holders, and force platform
Results
Calibration
The maximal force range per axis is determined by the linearity of the force platform output. As soon as the moving parts are out of boundary and motion is restricted, the force platform output becomes highly nonlinear and unpredictable. Within the working range, the output of the force platform is linear. For torque applied around the X and Y axes, the output is linear. However, if torque is applied around the Z axis, the output is quadratic. Table 1 presents the regression lines and R 2 values for the fitted data of each axis. The positive mean sensor output and output errors (±standard deviation, SD), together with linear fitted regression lines are presented in Fig. 6. The force and torque graphs of the negative sensor output range are similar to the graphs of the positive sensor output range of Fig. 6.

Mean ± standard deviation (SD) sensor output in arbitrary units and regression lines for a positive force and torque range
Accuracy
In Fig. 7 the results of the force and torque accuracy tests are presented. Three horizontal lines indicate the desired value.

Mean ± standard deviation (SD) sensor output during test run 1–3. Q1 to Q8 represent the direction vectors of the applied force and torque as described in the “Materials and methods” section
Sensitivity
A threshold, below which all data are discarded, prevents the untouched 3Dconnexion mouse from drifting. Until this threshold displacement is reached, the output values are zero. The threshold displacement together with the stiffness of the installed spring determines the threshold force and torque. Therefore, a stiffer set of springs increases the measurement range as well as the threshold value. In the force platform with a suitable measurement range for suture tasks, threshold values of 0.7 N for the Z axis and 0.5 N for the X and Y axes were found. Furthermore, the torque threshold values were determined as 0.02 Nm for the Z axis and 0.03 Nm for the X and Y axes.
Pilot study: needle-driving task
It took the surgeons 17.8 s (SD 2.1 s) and the novices 29.4 (SD 3.7 s) to complete the task. Before the surgeons and novices inserted the needle into the artificial tissue, a clear difference between orientation and position of the needle inside the needle driver was visible. After inserting the needle tip, the two types of subjects used different strategies to drive the needle through the tissue. The surgeons used mostly rotation (R) of the needle around an imaginary rotation point (Fig. 8A), whereas the novices used rotation (R) as well as translation (X, Y) (Fig. 8B). Furthermore, unlike most surgeons, all novices pressed the needle driver against the tissue during the task. A force graph and 3D force signature of the best-performing surgeon and novice are presented in Fig. 9A, B. The absolute nonzero mean force and maximal force of all subjects, measured during the needle-driving task, are presented in Fig. 10. The force graphs of the novice and surgeon who performed the needle-driving task four times are presented in Fig. 11. The maximum and mean absolute nonzero force used by the novices was on average 4.7 N (SD 1.3 N) and 2.1 N (SD 0.6 N), respectively. For surgeons, the average maximum force (2.6 N, SD 0.4 N) and the average mean force (0.9 N, SD 0.3 N) were much lower. Student t-tests showed that there was significant difference between the two groups of subjects for both depend variables (mean nonzero force: t = 4.3, p < 0.005, maximum force: t = 3.6, p < 0.017).

Observed difference in needle driving between expert (A) and novice (B). R is rotation around needle centre point, X is translation parallel to X-axis, Y is translation parallel to Y-axis

A Absolute force exerted on artificial tissue. B Three-dimensional representation of force exerted on artificial tissue

Differences between experts and novices in performance. Each data point represents the averaged value over two measurements of one subject

Force graphs of a novice and surgeon who performed the needle-driving task four times
Discussion
The developed force platform has mean accuracy for measuring forces of 0.1 N (SD 0.073 N) and 0.02 Nm (SD 0.016 Nm) for measuring torques. This makes the force platform suitable for almost any delicate training task that involves tissue manipulation. However, if forces are exerted at a position further than 60 mm from the midpoint of the force platform table, the mean output error can increase to ±10%. To account for larger deviations from the midpoint, the platform can be used in combination with endoscopic box-trainer tools that track motion, such as TrEndo [1]. If the position of the tip of the instrument with respect to the force platform midpoint is known, the accuracy can be improved.
The potential of the developed force platform for assessment in laparoscopic tasks was evaluated in a needle-driving task. During the needle-driving experiment only the force was measured and analyzed. Since the needle is inserted directly above the platform midpoint, the internal torque is negligible. For other tasks, depending on the dimensions of the task and required accuracy, torque measurements could be highly relevant for performance evaluation.
From our observations during the needle-driving experiment it became clear that the needle-driving strategy and performance speed had a great influence on the outcome of time-dependent parameters. Thus, if force parameters are used for subject assessment, it is important to take into account that occasionally there is no interaction between instruments and tissue. In this study we therefore excluded all zero force values when computing the performance measure of the mean force. Other observations suggest that it may be possible to use force measurements to reveal a learning curve (Fig. 11). However, a larger test group and more measurements per subject are needed before it is possible to determine which force parameters are representative for dexterous performance.
Force and torque information in training tasks
In the present study we evaluated performance in a needle-driving task. However, potentially any training task used to practice laparoscopic skills can be mounted on the force platform just like the suture task used in the pilot study. Box trainers equipped with the force platform can provide students and instructors with objective information about interaction forces and torques for more effective training and assessment.
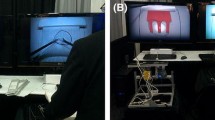
With respect to training, an important question that remains is how to present torque and force data to the student in real time (Fig. 12). When tasks are performed inside a laparoscopic box trainer, the resident’s attention is directed to the monitor. Furthermore, the complexity of the task may make it difficult to detect whether the proper amount of force is applied. If the platform is used for well-defined simple tasks, it should be possible to find an effective method of providing force feedback during training. One option is to use this same monitor to display torque and force information. Another option is to use sounds to indicate, for example, that the exerted torque or force exceeds a stored maximum value.

Schematic diagram of a resident during training on box trainer equipped with a force platform
Conclusions
An easy-to-use 6D platform was developed to measure force and torque in three directions during performance of endoscopic tasks inside box trainers. The low cost of the components and the compact design of the platform make it suitable for a broad range of training task purposes. The platform requires no modifications of instruments or box trainers. The developed software runs on a laptop or desktop system with a standard operating system. The first prototype, designed for delicate tasks in laparoscopy, measured forces and torques with mean accuracy of 0.1 N (SD 0.07 N) and 0.02 Nm (SD 0.016 Nm), respectively. Unfortunately, due to the threshold in the hardware of the mouse, forces less than 0.7 N and torques less than 0.03 Nm were not detected. However, a pilot needle-driving test conducted by five surgeons and five novices indicated that the platform is accurate and sensitive enough to reflect the most important differences in performance.
References
Chmarra MK, Bakker NH, Grimbergen CA, Dankelman J (2005) TrEndo, a device for tracking minimally invasive surgical instruments in training setups. Sens Actuators 126(2):328–334
Van Sickle KR, McCluskyIII DA, Gallagher AG, Smith CD (2005) Construct validation of the ProMIS simulator using a novel laparoscopic suturing task. Surg Endosc 19(9):1432–2218
Verdaasdonk EGG, Stassen LPS, Monteny LJ, Dankelman J (2006) Validation of a new basic virtual reality simulator for training of basic endoscopic skills—the Simendo. Surg Endosc 20(3):511–518
Middlebrook A, Chater P, Wilson M, Stone R, Sutton C, McCloy R (1997) MIST VR. A laparoscopic surgery procedures trainer and evaluator. Stud Health Technol Inform 39(6):598–607
Oshima N, Aizudding M, Midorikawa R, Solis J, Ogura Y, Takanishi A (2007) Development of a suture/ligature training system designed to provide quantitative information of the learning progress of trainees. In: IEEE international conference on robotics and automation, pp 2285–2291, 10–14 April 2007
Oshima N, Solis J, Ishii H, Matsuoka N, Hatake K, Takanishi A (2008) Integration of an evaluation function into the suture/ligature training system WKS-2R. In: ICRA 2008. IEEE international conference on robotics and automation, pp 1094–1099, 19–23 May 2008
Brooks TL (1990) Telerobotic response requirements. In: IEEE international conference on systems, man and cybernetics Conference Proceedings, pp 113–120, 4–7 Nov 1990
Heijnsdijk EAM, Pasdeloup A, van der Pijl AJ, Dankelman J, Gouma DJ (2003) The influence of force feedback and visual feedback in grasping tissue laparoscopically. Surg Endosc 18(6):980–985
Heijnsdijk EAM, de Visser H, Dankelman J, Gouma DJ (2004) Slip and damage properties of jaws of laparoscopic graspers. Surg Endosc 18(6):974–979
De Visser H, Heijnsdijk EAM, Herder JL, Pistecky PV (2002) Forces and displacements in colon surgery. Surg Endosc 16(10):1426–1430
Westebring van der Putten EP, Goossens RHM, Jakimowicz JJ, Dankelman J (2008) Haptics in minimally invasive surgery—a review. Minimally Invasive Ther Allied Technol 17(1):3–16
Acknowledgments
The authors would like to thank the BioMechanical Engineering (BME) technicians of the Delft University of Technology and Skillslab technicians of the Leiden University Medical Center for help in manufacturing and testing the force platform. They thank all students, surgeons, and gynecologists for participating in this study and providing practical information about surgical training tasks and box trainers.
Disclosures
Authors Tim Horeman, Sharon P Rodrigues, Frank-Willem Jansen, Jenny Dankelman, and John J van den Dobbelsteen have no conflicts of interest or financial ties to disclose.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Horeman, T., Rodrigues, S.P., Jansen, FW. et al. Force measurement platform for training and assessment of laparoscopic skills. Surg Endosc 24, 3102–3108 (2010). https://doi.org/10.1007/s00464-010-1096-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-1096-9