
Abstract
Background
Laparoscopic colorectal resection (LCR) is gaining popularity. Nonetheless, open surgery remains an important technique. Thus, surgeons should be technically proficient in both open and laparoscopic surgery. One question however remains unanswered: Can training for open and LCR occur simultaneously? The objective of this paper is to review the learning curve for open and laparoscopic colon resection of one surgeon who underwent a rigorous training program.
Methods
A review of consecutive patients who underwent surgery for colon and rectosigmoid junction cancers by one trainee surgeon was performed. This surgeon had completed his basic surgical residency but had limited experience in colorectal cancer surgery. In total, 75 patients were included in this study. All operations were supervised by at least one staff surgeon with experience of more than 300 LCR cases. The trainee surgeon was allowed to train in both laparoscopic and open colorectal resection simultaneously.
Results
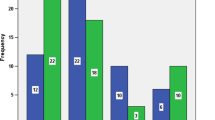
Forty-three patients underwent laparoscopic resection, while 32 patients underwent open surgery. Age, gender, mean body mass index (BMI), preoperative risk, and history of past abdominal surgery showed no significant difference between laparoscopic and open groups. There were no differences in tumor stage [International Union against Cancer (UICC)] or tumor size (p = 0.068 and 0.228, respectively). The morbidity rate for open and laparoscopic surgery was 3.1% (1/32) and 4.7% (2/43), respectively (p = 0.484). Operation time decreased with increasing experience, and plateaued after 25 cases in the laparoscopic group and 22 cases in the open group. The learning curve for open cases was 11 cases, and 7 for laparoscopic surgery.
Conclusions
Surgeons who have completed a basic surgical residency but have limited colorectal surgery experience can learn both open and laparoscopic colorectal surgery simultaneously in an effective manner under supervision by well-experienced surgeons.


Similar content being viewed by others

References
Hewett PJ, Allardyce RA, Bagshaw PF, Frampton CM, Frizelle FA, Rieger NA, Smith JS, Solomon MJ, Stephens JH, Stevenson AR (2008) Short-term outcomes of the Australasian randomized clinical study comparing laparoscopic and conventional open surgical treatments for colon cancer: the ALCCaS trial. Ann Surg 248(5):728–738
Braga M, Vignali A, Gianotti L, Zuliani W, Radaelli G, Gruarin P, Dellabona P, Di Carlo V (2002) Laparoscopic versus open colorectal surgery: a randomized trial on short-term outcome. Ann Surg 236(6):759–766 disscussion 67
Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith AM, Heath RM, Brown JM (2007) Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol 25(21):3061–3068
Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ, Haglind E, Pahlman L, Cuesta MA, Msika S, Morino M, Lacy AM (2005) Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol 6(7):477–484
Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW Jr, Hellinger M, Flanagan R Jr, Peters W, Nelson H (2007) Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg 246(4):655–662; discussion 62–64
Jamali FR, Soweid AM, Dimassi H, Bailey C, Leroy J, Marescaux J (2008) Evaluating the degree of difficulty of laparoscopic colorectal surgery. Arch Surg 143(8):762–767; discussion 8
Li JC, Hon SS, Ng SS, Lee JF, Yiu RY, Leung KL (2009) The learning curve for laparoscopic colectomy: experience of a surgical fellow in an university colorectal unit. Surg Endosc 23(7):1603–1608
Tekkis PP, Senagore AJ, Delaney CP, Fazio VW (2005) Evaluation of the learning curve in laparoscopic colorectal surgery: comparison of right-sided and left-sided resections. Ann Surg 242(1):83–91
Reichenbach DJ, Tackett AD, Harris J, Camacho D, Graviss EA, Dewan B, Vavra A, Stiles A, Fisher WE, Brunicardi FC, Sweeney JF (2006) Laparoscopic colon resection early in the learning curve: what is the appropriate setting? Ann Surg 243(6):730–735; discussion 5–7
Simons AJ, Anthone GJ, Ortega AE, Franklin M, Fleshman J, Geis WP, Beart RW Jr (1995) Laparoscopic-assisted colectomy learning curve. Dis Colon Rectum 38(6):600–603
Fukunaga Y, Higashino M, Tanimura S, Takemura M, Osugi H (2008) Laparoscopic colorectal surgery for neoplasm. A large series by a single surgeon. Surg Endosc 22(6):1452–1458
Wishner JD, Baker JW Jr, Hoffman GC, Hubbard GW II, Gould RJ, Wohlgemuth SD, Ruffin WK, Melick CF (1995) Laparoscopic-assisted colectomy. The learning curve. Surg Endosc 9(11):1179–1183
Choi DH, Jeong WK, Lim SW, Chung TS, Park JI, Lim SB, Choi HS, Nam BH, Chang HJ, Jeong SY (2009) Learning curves for laparoscopic sigmoidectomy used to manage curable sigmoid colon cancer: single-institute, three-surgeon experience. Surg Endosc 23(3):622–628
Dincler S, Koller MT, Steurer J, Bachmann LM, Christen D, Buchmann P (2003) Multidimensional analysis of learning curves in laparoscopic sigmoid resection: eight-year results. Dis Colon Rectum 46(10):1371–1378; discussion 8–9
Schlachta CM, Mamazza J, Seshadri PA, Cadeddu M, Gregoire R, Poulin EC (2001) Defining a learning curve for laparoscopic colorectal resections. Dis Colon Rectum 44(2):217–222
Yap CH, Colson ME, Watters DA (2007) Cumulative sum techniques for surgeons: a brief review. Aust N Z J Surg 77(7):583–586
Lin YY, Shabbir A, So JB (2009) Laparoscopic appendectomy by residents: evaluating outcomes and learning curve. Surg Endosc 24(1):125–130
Friedman RL, Pace BW (1996) Resident education in laparoscopic cholecystectomy. Surg Endosc 10(1):26–28
Kauvar DS, Braswell A, Brown BD, Harnisch M (2006) Influence of resident and attending surgeon seniority on operative performance in laparoscopic cholecystectomy. J Surg Res 132(2):159–163
Wilkiemeyer M, Pappas TN, Giobbie-Hurder A, Itani KM, Jonasson O, Neumayer LA (2005) Does resident post graduate year influence the outcomes of inguinal hernia repair? Ann Surg 241(6):879–882; discussion 82–84
Anderson BO, Sun JH, Moore EE, Thompson LL, Harkin AH, Bartle EJ (1989) The development and evaluation of a clinical test of surgical resident proficiency. Surgery 106(2):347–352; discussion 52–53
Bowles TA, Watters DA (2007) Time to CUSUM: simplified reporting of outcomes in colorectal surgery. Aust N Z J Surg 77(7):587–591
Park IJ, Choi GS, Lim KH, Kang BM, Jun SH (2009) Multidimensional analysis of the learning curve for laparoscopic resection in rectal cancer. J Gastrointest Surg 13(2):275–281
Maeda T, Tan KY, Konishi F, Tsujinaka S, Mizokami K, Sasaki J, Kawamura YJ (2009) Trainee surgeons do not cause more conversions in laparoscopic colorectal surgery if they are well supervised. World J Surg 33(11):2439–2443
Elliot DL, Hickam DH (1987) Evaluation of physical examination skills. Reliability of faculty observers and patient instructors. JAMA 258(23):3405–3408
Van Rij AM, McDonald JR, Pettigrew RA, Putterill MJ, Reddy CK, Wright JJ (1995) Cusum as an aid to early assessment of the surgical trainee. Br J Surg 82(11):1500–1503
de Leval MR, Francois K, Bull C, Brawn W, Spiegelhalter D (1994) Analysis of a cluster of surgical failures. Application to a series of neonatal arterial switch operations. J Thorac Cardiovasc Surg 107(3):914–923; discussion 23–24
Disclosures
Authors Maeda, Tan, Konishi, Tsujinaka, Mizokami, Sasaki, and Kawamura have no conflicts of interest or financial ties to disclosure.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maeda, T., Tan, K.Y., Konishi, F. et al. Accelerated learning curve for colorectal resection, open versus laparoscopic approach, can be attained with expert supervision. Surg Endosc 24, 2850–2854 (2010). https://doi.org/10.1007/s00464-010-1063-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-1063-5