
Abstract
Background
Percutaneous endoscopic gastrostomy (PEG), direct percutaneous endoscopic jejunostomy, and laparoscopic feeding tube insertion are established techniques for placing a feeding tube. However, these techniques may be difficult or contraindicated after previous gastric or upper abdominal surgery.
Methods
A total of 10 patients underwent minimally invasive jejunostomy tube insertion via endoscopic identification of the jejunum. The indications for the procedure were dysphagia, poor nutritional status, prolonged intensive care unit (ICU) admission, and gastroparesis. Eight of the patients had undergone previous upper abdominal surgeries and were rejected for either PEG or direct percutaneous jejunostomy. With the patients under general anesthesia, esophagogastroduodenoscopy was performed. The jejunum was identified and intubated. A small abdominal incision (1 in.) was made. The proximal jejunum was identified easily by the light and digital palpation of the endoscope. The jejunum was delivered in the wound, and the jejunostomy tube was inserted using Witzel’s technique. The wound was closed.
Results
All the patients tolerated the procedure well. The mean time for the procedure was 29 ± 13 min. There was no mortality related to the procedure and no complications. Jejunal feeding started on the first postoperative day.
Conclusion
The use of intraoperative endoscopy facilitated identification of the jejunum. Easy, safe, and quick, the procedure saved the patient a formal laparotomy and extensive manipulation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Long-term enteral tubes have a definite role in providing nutritional support for the debilitated patient. They provide for the administration of nutrients, fluids, or medications to patients unable to maintain adequate oral intake. Enteral nutritional support is superior to total parenteral nutrition (TPN) in achieving nutritional goals, improving outcomes, maintaining gastrointestinal mucosal integrity, promoting immunosecretory function, and avoiding infectious complications [1–5].
For certain patients, jejunal feeding is preferred over gastrostomy tube feeding. Several studies have shown that postpyloric feeding decreases the rate of aspiration of gastric contents by patients at high risk for this complication [5–11].
The percutaneous and endoscopic techniques have rapidly replaced traditional surgery as the preferred route for insertion of an enteral access. Laparoscopically assisted insertion of the feeding tube was developed as an alternative method for failed percutaneous cases [12].
Under certain circumstances, such as previous gastrectomy and previous major upper abdominal operations, insertion of percutaneous feeding tubes can be contraindicated. Under these conditions, a formal laparotomy may be required for insertion of the tube in the proper position. This can be technically demanding and may be associated with increased patient morbidity.
To date, no published studies have directly compared percutaneous endoscopic gastrostomy/jejunostomy with surgical insertion of feeding tubes [13]. In this report, the author describes a new approach that allows for safer, easier, and quicker insertion of a jejunostomy tube in challenging patients.
Materials and methods
A retrospective study analyzed 10 cases of endoscopically assisted Witzel jejunostomy tube placement. The procedures had been performed at the McClellan Veteran Administration Hospital, Little Rock, Arkansas and the University of Kansas, Kansas City, Kansas. The endoscopic part of the procedure was performed by the author, whereas the surgical part was performed by a senior surgery resident (postgraduate year 3 or above) under the direction of the author. Informed consent for upper gastrointestinal endoscopy and feeding tube placement was obtained for all the patients. Table 1 lists the indications for the procedure.
All the procedures were performed in the operating room with the patient under general anesthesia. The patient’s abdomen was prepped with DuraPrep (3 M Inc., St. Paul, MN, USA), then draped as usual. The procedures were performed with the patient in the supine position using the Pentax (PENTAX of America Inc., PENTAX Medical Company, Montvale, NJ, USA) or Olympus (Olympus America Inc., Center Valley, PA, USA) video endoscope. Either a sterile enteroscope or a colonoscope was used because either one provides the required length to reach the jejunum.
A formal endoscopic examination of the upper gastrointestinal tract was performed. Then the endoscope was passed to the jejunum. In some patients, the ligament of Treitz was challenging to cross because the endoscope tended to loop in the stomach. Straightening the endoscope as in colonoscopy helped to overcome this difficulty. Once past the ligament of Treitz, the endoscope was advanced a few more inches.
The skin was infiltrated with local anesthetic 2 in. (5 cm) below the left costal margin and in the midclavicular plane. A 1-in. (2 cm) skin incision was performed using a no. 15 surgical blade. The subcutaneous fat was dissected down to the level of the anterior abdominal wall fascia. The muscle-splitting technique was used to reach the peritoneum.
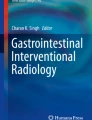
Once the peritoneal cavity was entered, any adhesions were carefully dissected. The location of the endoscope was identified using the index finger and the endoscope illumination. The loop of the jejunum containing the endoscope then was delivered in the wound using a Babcock clamp under direct visualization from within the lumen to ensure that the correct loop was being delivered (Fig. 1).

Delivery of the jejunum into the wound
Once delivered in the wound, the jejunostomy tube (12-Fr. red rubber catheter) was inserted according to Witzel’s technique. The placement of the tube in the distal jejunal loop was confirmed endoscopically. Next, the catheter was delivered through a separate incision and secured in place. The wound then was closed (Fig. 2).

The Witzel jejunostomy is completed
For the patient with a previous gastrectomy and Billroth II, portable X-ray fluoroscopy was used to identify the location of the endoscope. It was easier to identify the efferent loop by the straight pattern of the endoscope on fluoroscopy. In the later cases, the author chose to use fluoroscopy for easy identification of the endoscope’s location.
Results
From October 2003 to February 2008, 10 patients required nutritional support for different indications. Identification of the jejunum was easier using enteroscopy. No conversion to open laparotomy was needed. The mean time for the procedure was 29 ± 13 min.
All the patients with endoscopically assisted Witzel jejunostomy placement started tube feeding in the next day. The patients receiving TPN were weaned off it once feeding goals were achieved (Fig. 3).

The feeding tube is passed through a separate incision before the wound is approximated
No immediate complications related to the procedure occurred. One patient receiving tube feeding at home had dislodgment of the tube. This occurred 45 days after the patient’s discharge from the hospital. Reinsertion of a new tube was done in the emergency room through the same wound tract. The placement was radiologically confirmed, and the patient was sent home.
Discussion
Percutaneous endoscopic gastrostomy (PEG) has been the preferred method for enteral feeding. It is easy to perform, with the PEG tube inserted at the bedside. The PEG procedure may be difficult or unsuccessful for patients with prior abdominal surgery, gastric resection, ascites, hepatomegaly, or obesity. Relative contraindications to PEG include obesity, severe gastroesophageal reflux, gastroparesis, neurologic disorders, history of repeated tube feeding-related aspiration, and neoplastic, inflammatory, or infiltrative disease of the gastric or abdominal walls [14]. Percutaneous endoscopic jejunostomy (PEJ) and jejunal extension through a PEG were developed to replace PEG when gastric feeding is contraindicated or not preferred [15].
The PEG tube with the jejunostomy extension (PEG/J) was reported to have complications for 53% of patients, with 11% leakage around the tube, 23% plugging of tubes, 4% fracture of tubes, and 15% retrograde migration of tubes [16]. In the same study, 28% of the patients required exchange or removal of the PEG/J tube after a mean of 60 days.
Direct percutaneous endoscopic jejunostomy (DPEJ) is similar to PEG. It is considered more difficult due to the mobility of the jejunum and the difficulty obtaining transillumination [17]. For a Mayo clinic series, the success rate of direct percutaneous jejunostomy tube insertion was 73% [18]. The insertion of the PEJ carries a success rate of 64 to 92.3% [17, 19–22]. For ultrasound/fluoroscopically guided PEJ placement, the success rate is 87% [23].
Laparoscopic gastrostomy, jejunostomy, minilaparoscopy, and laparoendoscopic placement were introduced to overcome the aforementioned difficulties. [24–29]. In these patients, the author did not consider the PEJ approach. The contraindications for PEJ were the same as for PEG in these patients.
Tube insertion was successful for all the patients. No immediate complications were observed. The length of our procedure was shorter (29 ± 13 min) than the laparoscopic/endoscopic technique reported by Etzkorn et al. [27]. The author elected to use general anesthesia for two reasons. First, six patients were already ventilator dependent. Second, in the case of procedure failure, laparotomy was to be considered.
This report introduces a new approach to jejunal tube insertion for patients who are not candidates for minimally invasive options. Although promising, the study needs more patients before a conclusion can be drawn.
References
Wicks C, Somasundaram S, Bjarnason I, Menzies IS, Routley D, Potter D et al (1994) Comparison of enteral feeding and total parenteral after liver transplantation. Lancet 344:837–840
Lowry SF (1990) The route of feeding influences injury responses. J Trauma 30:S10–S15
Schloerb PR (2001) Immune-enhancing diets: products, components, and their rationales. JPEN J Parenter Enteral Nutr 25(2 Suppl):S3–S7
Shikora SA, Ogawa AM (1996) Enteral nutrition and the critically ill. Postgrad Med J 72:395–402
Kudsk KA, Croce MA, Fabian TC, Minard G, Tolley EA, Poret HA et al (1992) Enteral versus parenteral feeding: effects on septic morbidity after blunt and penetrating abdominal trauma. Ann Surg 215:503–513
Heyland DK, Drover JW, MacDonald S, Novak F, Lam M (2001) Effect of postpyloric feeding on gastroesophageal regurgitation and pulmonary microaspiration: results of a randomized controlled trial. Crit Care Med 29:1495–1501
Cech AC, Morris JB, Mullen JL, Crooks GW (1995) Long-term enteral access in aspiration-prone patients. J Intensive Care Med 10:179–186
Nicholas JM, Cornelius MW, Tchorz KM, Tremblay LN, Spiegelman ER, Easley KA et al (2003) A two-institution experience with 226 endoscopically placed jejunal feeding tubes in critically ill surgical patients. Am J Surg 186:583–590
Moore EE, Jones TN (1986) Benefits of immediate jejunostomy feeding after major abdominal trauma: a prospective, randomized study. J Trauma 26:874–881
Zaloga GP (1999) Early enteral nutritional support improves outcome hypothesis or fact (editorial). Crit Care Med 27:259–261
Singh G, Ram RP, Khanna SK (1998) Early postoperative enteral feeding in patients with nontraumatic intestinal perforation and peritonitis. J Am Coll Surg 187:142–146
Denzer U (2003) Minilaparoscopically guided percutaneous gastrostomy and jejunostomy. Gastrointest Endosc 58:434–438
Bosco JJ, Barkun AN, Isenberg GA, Nguyen CC, Petersen BT, Silverman WB et al (2002) Endoscopic enteral nutritional access devices. Gastrointest Endosc 56:796–802
Ponsky JL, Aszodi A (1984) Percutaneous endoscopic jejunostomy. Am J Gastroenterol 79:113–116
Gottfried EB, Plumser AB (1984) Endoscopic gastrojejunostomy: a technique to establish small bowel feeding without laparotomy. Gastrointest Endosc 30:355–357
Wolfsen HC, Kozarek RA, Ball TJ, Patterson DJ, Botoman VA (1990) Tube dysfunction following percutaneous endoscopic gastrostomy and jejunostomy. Gastrointest Endosc 36:261–263
Shike M, Latkany L, Gerdes H, Bloch AS (1996) Direct percutaneous endoscopic jejunostomy for enteral feeding. Gastrointest Endosc 44:536–540
Rumalla A, Baron TH (2000) Results of direct percutaneous endoscopic jejunostomy: an alternative method for providing jejunal feeding. Mayo Clinic Proc 75:807–810
Shike M, Wallach C, Likier H (1991) Direct percutaneous endoscopic jejunostomies. Gastrointest Endosc 37:62–65
Mellert J, Naruhn MB, Grund KE, Becker HD (1994) Direct endoscopic percutaneous jejunostomy. Surg Endosc 8:867–870
Rumall A, Baron TH (2000) Results of direct percutaneous endoscopic jejunostomy: an alternative method for providing jejunal feeding. Mayo Clin Proc 75:807–810
Varadarajulu S (2003) Use of a 19-gauge injection needle as a guide for direct percutaneous endoscopic jejunostomy tube placement. Gastrointest Endosc 57:942–945
van Overhagen H, Ludviksson MA, Lameris JS, Zwamborn AW, Tilanus HW, Dees J, Hansen BE (2000) US and fluoroscopic-guided percutaneous jejunostomy: experience in 49 patients. J Vasc Int Radiol 11:101–106
Denzer U (2003) Mini-laparoscopically guided percutaneous gastrostomy and jejunostomy. Gastrointest Endosc 58:434–438
Murayama KM, Johnson TJ, Thompson JS (1996) Laparoscopic gastrostomy and jejunostomy are safe and effective for obtaining enteral access. Am J Surg 172:591–594
Scheer MF, Miedema BW (1995) Laparoscopic assisted percutaneous endoscopic gastrostomy. Surg Laparosc Endosc 5:483–486
Etzkorn KP, Vitello J, Resnick D, McGuire DE, Venu RP, Watkins JL (1996) A new technique for jejunal tube placement: a marriage of enteroscope and laparoscope. Gastrointest Endosc 43:610–614
Morris JB, Mullen JL, Yu JC et al (1992) Laparoscopic-guided jejunostomy. Surgery 112:96–99
Eltringham WK, Roe AM, Galloway SW et al (1993) A laparoscopic technique for full-thickness intestinal biopsy and feeding jejunostomy. Gut 34:122–124
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Selim, N.M. Endoscopic identification of the jejunum facilitates minimally invasive jejunostomy tube insertion in selected cases. Surg Endosc 23, 2587–2590 (2009). https://doi.org/10.1007/s00464-009-0469-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-009-0469-4