
Abstract
Introduction
Fine-needle aspiration (FNA) is a well-established technique to obtain cytological specimens, but it does not permit the extraction of histological tissue-core samples, which, if available, may increase the yield and accuracy of the histopathological diagnosis. This prospective study was designed to assess the yield and diagnostic accuracy of endoscopic ultrasound (EUS)-guided Trucut needle biopsy (TNB) as first-line diagnostic method for suspected malignant lesions identified by upper gastrointestinal EUS.
Methods
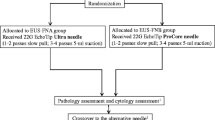
In a prospective case series, 24 consecutive patients (14 women; median age, 68 (range, 38–84) years) with suspected malignancy underwent EUS-TNB with a 19-gauge needle. EUS was performed with a linear scanning echo endoscope. When the EUS-TNB device did not collect adequate samples, subsequent EUS-FNA was performed. The presence or absence of malignancy was confirmed by postoperative histopathology or diagnostic imaging follow-up for at least 9 months.
Results
Adequate tissue specimens were obtained in 20 of 24 (83%) patients by TNB. An accurate diagnosis was achieved in 19 of 20 (95%) patients in whom TNB was successful with a sensitivity and specificity of 93% and 100%, respectively. In 11 patients malignant disease was found, whereas 8 patients showed benign lesions on TNB-obtained histopathology. Thirteen patients underwent additional EUS-FNA. The diagnosis by TNB was confirmed in seven of nine (78%) patients with additional FNA. In three of four patients with inadequate TNB, the diagnosis was established by FNA. The overall accuracy of EUS-TNB was 79% (19/24) for all patients and 92% (22/24) with subsequent FNA. The positive and negative predictive values for the diagnosis of a malignant lesion by EUS-TNB were 57.9% and 88.9%, respectively. Neither method had any procedure-related complications.
Conclusions
EUS-guided TNB is a safe and accurate technique to obtain core specimen for histopathologic diagnosis in patients with suspected malignancies on upper gastrointestinal EUS. FNA can serve as rescue technique and should be performed if TNB fails to obtain adequate tissue samples.
Similar content being viewed by others


References
Shah JN, Ahmad NA, Beilstein MC, Ginsberg GG, Kochman ML (2004) Clinical impact of endoscopic ultrasonography on the management of malignancies. Clin Gastroenterol Hepatol 2:1069–1073
Savides TJ, Donohue M, Hunt G, Al-Haddad M, Aslanian H, Ben-Menachem T, Chen VK, Coyle W, Deutsch J, DeWitt J, Dhawan M, Eckardt A, Eloubeidi M, Esker A, Gordon SR, Gress F, Ikenberry S, Joyce AM, Klapman J, Lo S, Maluf-Filho F, Nickl N, Singh V, Wills J, Behling C (2007) EUS-guided FNA diagnostic yield of malignancy in solid pancreatic masses: a benchmark for quality performance measurement. Gastrointest Endosc 66:277–282
Mortensen MB, Pless T, Durup J, Ainsworth AP, Plagborg GJ, Hovendal C (2001) Clinical impact of endoscopic ultrasound-guided fine needle aspiration biopsy in patients with upper gastrointestinal tract malignancies. A prospective study. Endoscopy 33:478–483
Erickson RA (2004) EUS-guided FNA. Gastrointest Endosc 60:267–279
Iglesias Garcia J, Dominguez-Munoz JE (2007) Endoscopic ultrasound-guided biopsy for the evaluation of pancreatic tumors. Gastroenterol Hepatol 30:597–601
Saftoiu A, Vilmann P, Guldhammer Skov B, Georgescu CV (2007) Endoscopic ultrasound (EUS)-guided Trucut biopsy adds significant information to EUS-guided fine-needle aspiration in selected patients: a prospective study. Scand J Gastroenterol 42:117–125
Eloubeidi MA, Tamhane A, Jhala N, Chhieng D, Jhala D, Crowe DR, Eltoum IA (2006) Agreement between rapid onsite and final cytologic interpretations of EUS-guided FNA specimens: implications for the endosonographer and patient management. Am J Gastroenterol 101:2841–2847
Levy MJ, Jondal ML, Clain J, Wiersema MJ (2003) Preliminary experience with an EUS-guided Trucut biopsy needle compared with EUS-guided FNA. Gastrointest Endosc 57:101–106
Varadarajulu S, Fraig M, Schmulewitz N, Roberts S, Wildi S, Hawes RH, Hoffman BJ, Wallace MB (2004) Comparison of EUS-guided 19-gauge Trucut needle biopsy with EUS-guided fine-needle aspiration. Endoscopy 36:397–401
Wiersema MJ, Hawes RH, Tao LC, Wiersema LM, Kopecky KK, Rex DK, Kumar S, Lehman GA (1992) Endoscopic ultrasonography as an adjunct to fine needle aspiration cytology of the upper and lower gastrointestinal tract. Gastrointest Endosc 38:35–39
Gines A, Wiersema MJ, Clain JE, Pochron NL, Rajan E, Levy MJ (2005) Prospective study of a Trucut needle for performing EUS-guided biopsy with EUS-guided FNA rescue. Gastrointest Endosc 62:597–601
DeWitt J, McGreevy K, LeBlanc J, McHenry L, Cummings O, Sherman S (2005) EUS-guided Trucut biopsy of suspected nonfocal chronic pancreatitis. Gastrointest Endosc 62:76–84
Aithal GP, Anagnostopoulos GK, Tam W, Dean J, Zaitoun A, Kocjan G, Ragunath K, Pereira SP (2007) EUS-guided tissue sampling: comparison of “dual sampling” (Trucut biopsy plus FNA) with “sequential sampling” (Trucut biopsy and then FNA as required). Endoscopy 39:725–730
Wittmann J, Kocjan G, Sgouros SN, Deheragoda M, Pereira SP (2006) Endoscopic ultrasound-guided tissue sampling by combined fine needle aspiration and Trucut needle biopsy: a prospective study. Cytopathology 17:27–33
Larghi A, Verna EC, Stavropoulos SN, Rotterdam H, Lightdale CJ, Stevens PD (2004) EUS-guided Trucut needle biopsies in patients with solid pancreatic masses: a prospective study. Gastrointest Endosc 59:185–190
Itoi T, Itokawa F, Sofuni A, Nakamura K, Tsuchida A, Yamao K, Kawai T, Moriyasu F (2005) Puncture of solid pancreatic tumors guided by endoscopic ultrasonography: a pilot study series comparing Trucut and 19-gauge and 22-gauge aspiration needles. Endoscopy 37:362–366
Levy MJ, Wiersema MJ (2005) EUS-guided Trucut biopsy. Gastrointest Endosc 62:417–426
Pungpapong S, Wallace MB (2005) EUS-guided Trucut needle biopsy: is more tissue really better? Gastrointest Endosc 62:602–604
Levy MJ, Reddy RP, Wiersema MJ, Smyrk TC, Clain JE, Harewood GC, Pearson RK, Rajan E, Topazian MD, Yusuf TE, Chari ST, Petersen BT (2005) EUS-guided Trucut biopsy in establishing autoimmune pancreatitis as the cause of obstructive jaundice. Gastrointest Endosc 61:467–472
Yadav D, Levy MJ, Schwartz D, Jondal ML, Clain J, Wiersema MJ (2003) EUS-guided Trucut biopsy for diagnosis of an esophageal stromal tumor: case report. Gastrointest Endosc 58:457–460
Ribeiro A, Vernon S, Quintela P (2004) EUS-guided Trucut biopsy with immunohistochemical analysis of a gastric stromal tumor. Gastrointest Endosc 60:645–648
Gleeson F, Clarke E, Kelly S, Hargadan G, Kenny E, MacMathuna P, Lennon J (2005) Diagnosis by EUS Trucut biopsy of extrapulmonary tuberculosis in a patient with Crohn’s disease treated with infliximab. Gastrointest Endosc 61:489–492
Aithal GP, Anagnostopoulos GK, Kaye P (2005) EUS-guided Trucut mural biopsies in the investigation of unexplained thickening of the esophagogastric wall. Gastrointest Endosc 62:624–629
Storch I, Shah M, Thurer R, Donna E, Ribeiro A (2008) Endoscopic ultrasound-guided fine-needle aspiration and Trucut biopsy in thoracic lesions: when tissue is the issue. Surg Endosc 22:86–90 Epub 2007 May 4
Storch I, Jorda M, Thurer R, Raez L, Rocha-Lima C, Vernon S, Ribeiro A (2006) Advantage of EUS Trucut biopsy combined with fine-needle aspiration without immediate on-site cytopathologic examination. Gastrointest Endosc 64:505–511
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wahnschaffe, U., Ullrich, R., Mayerle, J. et al. EUS-guided Trucut needle biopsies as first-line diagnostic method for patients with intestinal or extraintestinal mass lesions. Surg Endosc 23, 2351–2355 (2009). https://doi.org/10.1007/s00464-009-0345-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-009-0345-2