
Abstract
Objective
To explore the value of 99mTc-isonitrile deoxyglucosamine (CNDG) SPECT/CT in the staging and resectability diagnosis of non-small cell lung cancer (NSCLC) compared with contrast-enhanced CT (CECT).
Methods
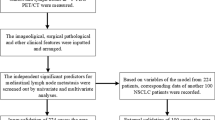
This research was approved by the hospital ethics review committee. Sixty-three patients with NSCLC received 99mTc-CNDG SPECT/CT, CECT and initial TNM staging before treatment. Thirty-three patients who underwent radical surgery underwent postoperative pathological TNM staging as the reference standard. Another thirty patients underwent radiochemotherapy; among them, the reference standard of 7 patients of N staging and 5 patients of M staging was based on biopsy pathology, and the diagnosis of the remaining lesions was confirmed by at least one different image or clinical imaging follow-up for more than 3 months. The McNemar test and receiver operating characteristic (ROC) curve analysis were used to compare the diagnostic accuracy of staging and resectability of 99mTc-CNDG SPECT/CT and CECT in NSCLC, respectively.
Results
For all patients and surgical patients, the accuracies of 99mTc-CNDG SPECT/CT in diagnosing the T stage and N stage were higher than those of CECT (all patients: 90.5%, 88.9% vs. 79.4%, 60.3%; surgical patients: 81.8%, 78.8% vs. 60.6%, 51.5%), and the differences were statistically significant (all patients: T stage, P = 0.016; N stage, P = 0.000; surgical patients: T stage, P = 0.016; N stage, P = 0.004). For all patients, the accuracy of 99mTc-CNDG SPECT/CT in diagnosing the M stage was higher than that of CECT (96.8% vs. 90.5%), but the difference was not statistically significant (P = 0.289). ROC curve analysis showed that the accuracy of 99mTc-CNDG SPECT/CT in diagnosing the potential resectability of NSCLC was significantly better than that of CECT (P = 0.046).
Conclusion
This preliminary clinical study shows that 99mTc-CNDG SPECT/CT is of great value for accurate clinical staging of NSCLC compared with CECT and can significantly improve the accuracy of resectability diagnosis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Malignant tumors are characterized by uncontrolled proliferation, invasion and metastasis. During malignant tumor evolution, glucose transporters (Gluts), which are the main carriers of cell glucose transmembrane transport, and hexokinase (HK), which is an important rate-limiting enzyme in the glycolytic pathway, are overexpressed, which significantly increases the glucose uptake and glycolysis rate of malignant tumor cells. The abnormal increase in glucose metabolism in malignant tumor cells is more than 200 times greater than that in normal cells, which is called the Warburg effect. Warburg effect has been recognized as a feature of cancer and as a promising tumor-specific target.Glucose carbons can supply several metabolic pathways, including hexosamine biosynthesis, redox balance, nucleotide production through pentose phosphate pathway, but the detailed tumor metabolic pathway of glucose in vivo is not fully understood (Feng et al. 2019; Reckzeh and Waldmann 2020). Based on this, PET/CT and SPECT/CT nuclear medicine tumor molecular imaging modalities are used for tumor glucose metabolism imaging, and 18F-2-deoxy-D-fluoro-glucose (18F-FDG) has become a widely used glucose metabolism imaging agent in tumor diagnosis, staging and treatment decisions (Zhang et al. 2021; Kandathil et al. 2018). However, 18F-FDG PET/CT has some shortcomings, such as false positives in benign proliferative inflammatory lesions, false negatives in some types of malignant tumors or well-differentiated malignant tumors, complex preparation of 18F-FDG, expensive equipment and poor accessibility to primary hospitals (Werutsky et al. 2019).
99mTc-labeled glucose SPECT/CT is a widely available, inexpensive and convenient molecular imaging technique of nuclear medicine. 99mTc has excellent nuclide properties (Eγ = 140 keV, T1/2 = 6.02 h), and its various oxidation states can be coordinated with different ligands to prepare various new radiopharmaceuticals. 99mTc is supplied internally by a molybdenum technetium generator at a low price; additionally, the number of SPECT/CT scanners worldwide far exceeds that of PET/CT scanners, which confers 99mTc-labeled glucose SPECT/CT with broad clinical application prospects (Meng et al. 2015; Gan et al. 2021). Recently, Zhang et al. (2018) of Beijing Normal University drew on the fact that the single ligand isonitrile (CN-R) can form a stable 99mTc complex ([99mTc(CN-R)6]+) with a 99mTc(I) nucleus in high yield, innovatively synthesize isonitrile deoxyglucosamine (CNDG), and obtain a new glucosamine imaging agent99mTc-CNDG. As an glucosamine analogue, 99mTc-CNDG has been proved that its tumor cell uptake is significantly related to glucose transporters and can potentially reflect the abnormal proliferation activity of tumor cells through additional glucosamine biosynthetic metabolic pathways and transcription processes involving the nucleus. In this study, surgical operation pathology, biopsy pathology and clinical imaging follow-up after treatment were used as reference standards for staging of non-small cell lung cancer (NSCLC), and the accuracies of 99mTc-CNDG SPECT/CT in the diagnosis of TNM staging and resectability of NSCLC were prospectively evaluated compared with conventional contrast-enhanced CT (CECT).
Patients and methods
Patients
This prospective study was approved by the hospital ethics review committee (20190627) and registered online in China National Medical Research Registration Information System (MR-46-22-022254). From January 2019 to October 2021, sixty-three patients (27 women, 36 men) with NSCLC diagnosed pathologically in our hospital were enrolled in this study. The mean age of the patients was 60.5 ± 8.8 years (range 43–83 years). In addition to routine laboratory examination, neck and abdomen ultrasound, chest routine CT, chest X-ray, brain CT, brain MRI, 99mTc-methylene diphosphate (MDP) bone imaging and other standard staging inspections, all patients underwent 99mTc-CNDG SPECT/CT and CECT within 2 weeks. The inclusion criteria were as follows: (1) patients who underwent radical surgery or radiochemotherapy within 2 weeks after imaging evaluation; and (2) patients who underwent pathology staging of radical surgery, pathology staging of puncture biopsy and clinical imaging follow-up staging for more than 3 months. The exclusion criteria were as follows: (1) patients with insulin-dependent diabetes mellitus or patients with a fasting blood glucose concentration exceeding 11.1 mmol/L before injection of 99mTc-CNDG; (2) patients who received radiochemotherapy before examination; and (3) patients with hepatic and renal insufficiency. In this study, patients with non-small cell lung cancer in different stages were included, and the potential effects of pre-99mTc-CNDG SPECT/CT blood glucose and radiochemotherapy were excluded, which could comprehensively and accurately reflect the accurate staging value of 99mTc-CNDG SPECT/CT for NSCLC.All patients were included in this study after informed consent was obtained.
99mTc-CNDG SPECT/CT
Fresh sodium pertechnetium solution was obtained by washing with a molybdenum technetium generator provided by Beijing Institute of Atomic Energy (Beijing, China). CNDG was provided by Beijing Shihong Pharmaceutical Center of Beijing Normal University (Beijing, China) with a freeze-dried kit. 2220–4400 MBq/1–5 ml sodium pertechnetium solution was added to a freeze-dried bottle of CNDG (1 mgCNDG, 0.06 mgSnCl2 H2O, 1 mg sodium citrate, 1 mgL-cysteine), placed in a water bath at 100 °C for 20 min, and then cooled to room temperature for later use. Radiochemical purity was determined by chromatography with a γ counter, and only when the labeling rate was greater than 95% could it be used.
Patients needed to fast for more than 6 h before injecting 99mTc-CNDG, and only a high-protein and low-sugar diet was allowed before imaging. After intravenous injection of 99mTc-CNDG (14.8–22.2 MBq/kg), patients rested in a supine position, and 800–1000 ml of sugar-free water was drinked for hydration before imaging. SPECT/CT was performed from the clavicular area to the upper abdomen after 3 h. The Symbia T16 SPECT/CT system from Siemens company was used, and it was equipped with a low-energy high-resolution collimator. The acquisition parameters were as follows: 5.6°/frame, 25 s/frame, 180° noncircular orbit rotation and 256 × 256 matrix. The images were reconstructed by an iterative method. Chest spiral CT was used for attenuation correction, anatomical localization and structural imaging diagnosis. SPECT/CT fusion images were obtained by using the Syngo workstation of Siemens company. 99mTc-CNDG drug labeling, quality control, 99mTc-CNDG SPECT/CT technical parameters and image post-processing technology were trained and standardized before the study. Any related side effects of the intravenous injection and imaging of 99mTc-CNDG were recorded.
CECT
The Discovery 750HD CT system from GE company was used. The dosage of contrast agent Ultravist (300 mg/ml) was injected intravenously according to the patient's weight (1.0–1.2 ml/kg), and the injection rate was 3.0–3.5 ml/second. Scanning from the clavicle area to the upper abdomen was performed 30 s and 45 s after injection of contrast agent, respectively, to obtain the images of arterial phase and venous phase of CECT. The acquisition parameters were as follows: voltage 120 kV, current 230 mA and pitch 1. The images were reconstructed with a 3.0 mm slice thickness. The use of CECT imaging agent Ultravist, imaging technical parameters and image post-processing technology were trained and standardized before the study.
Image analysis
Image interpretation was performed by two independent review boards of trained nuclear medicine physicians/radiologists. Readers were blinded to all patient dates other than the suspicion of NSCLC. If the diagnosis was inconsistent, consensus was reached through discussion. The interpretation of 99mTc-CNDG SPECT/CT was as follows: positive radioactive uptake was based on a visual method combined with a semi-quantitative parameter method, and visual assessment was based on whether the lesion had abnormal radioactive local uptake higher than the surrounding background. The parameter used in the semi-quantitative method was the target to nontarget tissue uptake ratio (T/NT), and it was judged as positive when T/NT ≥ 1.2,this positive criterion of cut-off value of T/NT ≥ 1.2 was based on the author's previous work (Wang et al. 2023). According to the fused image, the lesion site with abnormally high positive radioactivity was located, and the nature of the lesion was determined by lesion radioactive uptake combined with the structural image characteristics. The interpretation of CECT was as follows: positive lesions were interpreted based on the imaging structure and blood supply characteristics, and the nature of the lesions was determined according to lesion size, anatomical shape, enhancement degree and structural infiltration (including chest wall, mediastinum, esophagus, spine, etc.). In the image analysis of CECT, pulmonary lesions were analyzed with arterial images, while mediastinal lymph nodes, adrenal glands and liver lesions were analyzed with venous images.
Treatment methods and reference standards
Radical resection of lung cancer and lymph node dissection were performed for those patients who were clinically evaluated as resectable. With reference to 99mTc-CNDG SPECT/CT and CECT before the operation, the surgeon removed all accessible abnormal tumor tissues and abnormal lymph nodes in the hilum and mediastinum and then numbered the localized tumors and lymph nodes. The pathologist performed hematoxylin–eosin staining and immunohistochemistry to obtain histopathological results and pathological TNM staging. Radiochemotherapy was performed for those patients who were clinically evaluated as unresectable, and the TNM staging of these unresectable patients was determined by the biopsy pathology of the lesion and at least one different imaging method or clinical imaging follow-up for more than 3 months. The diagnosis of lesions by 99mTc-CNDG SPECT/CT and CECT was assessed in relation to the results of postoperative pathology, biopsy pathology and follow-up imaging.
The international multidisciplinary classification standard of lung cancer jointly introduced by the International Society for Lung Cancer Research (IASLC) and the American Thoracic Society (ATS) in 2011 was adopted for the pathological classification of lung cancer (Travis et al. 2011). The eighth edition Union for International Cancer Control (UICC) TNM staging standard was adopted for lung cancer staging (Detterbeck et al. 2017). Regional lymph node stations of lung cancer were divided into 14 groups according to the international lymph node map recommended by IASLC (Rusch et al. 2009). Potential resectability was characterized as the prevalence of 3 conditions: a T stage of less than 4, an N stage of less than 3, and an M stage of 0 (Vansteenkiste et al. 2013).
Statistical analysis
Statistical analysis was conducted using SPSS software (IBM SPSS Statistics 19, USA). Quantitative variables were expressed as the mean ± standard deviation, and qualitative variables were expressed as percentages. An independent sample t test was used to compare the mean of the two samples. 99mTc-CNDG SPECT/CT visual interpretation and semi-quantitative analysis were blind to pathology and follow-up results, and data analysis was carried out in strict accordance with statistical principles in statistical analysis. Considering that McNemar's test was suitable for comparing the paired sample rates of two imaging methods, it was used in this study to compare the diagnostic accuracy of 99 m Tc-CNDG SPECT/CT and CECT in NSCLC TNM staging; Considering that receiver operating characteristic (ROC) curve analysis and Z-test of comparison of area under curve were suitable for comparing the accuracy of different diagnostic tests, they were used in this study to compare the accuracy of 99mTc-CNDG SPECT/CT and CECT in diagnosing the potential resectability of tumors. P < 0.05 was considered statistically significant.
Results
Biological distribution and safety of 99mTc-CNDG in the human body
The imaging quality of 99mTc-CNDG SPECT/CT in the sixty-three patients with NSCLC was preferable. Three-hour whole-body imaging showed that there was no obvious uptake of 99mTc-CNDG in the normal brain, myocardium, lung, bone and muscle. A small amount of 99mTc-CNDG was found in the liver, spleen, nasopharynx, synovium of joints and peripheral blood, and a large amount of 99mTc-CNDG was found in the kidney, bladder, gallbladder and intestine. The low background of the lung, brain, myocardium, bone and muscle made it easy to display lung lesions and metastatic lesions of the brain, bone and mediastinal lymph nodes, while the metastatic lesions of the liver, adrenal gland and abdominal lymph nodes were relatively difficult to display because of the high background of surrounding tissues. No adverse reactions were reported during the injection and imaging of 99mTc-CNDG.
Pathology and follow-up
Of the sixty-three patients with NSCLC, 33 patients (52.4%) were clinically evaluated as operable and underwent radical resection of lung cancer plus lymph node dissection, and another 30 patients (47.6%) were clinically evaluated as inoperable and underwent radiochemotherapy. Among the 33 surgical patients, 30 patients underwent endoscopic radical resection of lung cancer plus lymph node dissection, and 3 patients underwent thoracotomy radical resection of lung cancer plus lymph node dissection. Among the 30 nonsurgical patients, 6 cases did not complete the scheduled radiochemotherapy, and 7 patients and 5 patients obtained histopathological N staging by lymph node biopsy and M staging by bone or pleural biopsy, respectively. The diagnoses of the remaining lesions were confirmed by at least one different image or follow-up imaging for more than 3 months.
For the 33 surgical patients with postoperative pathology, TNM staging was classified as stage IA in 19 patients, IB in 4, IIA in 1, IIB in 2, IIIA in 4, and IIIB in 3. For the 30 nonsurgical patients with biopsy pathology and clinical imaging follow-up, TNM staging was classified as stage IIIA in 2 patients, IIIB in 5, IIIC in 3, IVA in 14, and IVB in 6. The histopathological results of the 63 patients are presented in Table 1.
TNM staging accuracy
T staging accuracy
The uptake of 99mTc-CNDG was abnormally increased in the primary tumor of all sixty-three patients. The mean primary tumor long axis diameter was 34.11 ± 20.58 mm (range 9–90 mm), and the mean primary tumor T/NT was 3.55 ± 1.78 (range 1.2–9.0). One patient with suspected ipsilateral lung lobe metastasis by CECT showed negative 99mTc-CNDG SPECT/CT, and no metastasis was confirmed by postoperative pathology. There were 2 patients with nodular pericardial invasion, 1 patient was positive on both CECT and 99mTc-CNDG SPECT/CT, and 1 patient with only 99mTc-CNDG SPECT/CT showed abnormally increased tumor activity. One patient suspected of pericardial invasion by CECT showed no abnormal tumor activity by 99mTc-CNDG SPECT/CT and was confirmed as having a benign lesion after 10 months of CECT follow-up after radical resection of lung cancer. Among the 13 patients with incorrect T staging on CECT, 7 patients were overestimated (11.11%), and 6 patients were underestimated (9.52%). Among the 6 patients with incorrect T staging on 99mTc-CNDG SPECT/CT, 4 patients were overestimated (6.35%), and 2 patients were underestimated (3.17%).
N staging accuracy
Of the 33 patients who underwent surgery with regional lymph node pathological diagnosis conducted by surgical mediastinal lymph node dissection, 8 patients had lymph node metastasis, and 25 patients had no lymph node metastasis. In 22 metastatic lymph node stations, the mean lymph node short axis diameter was 9.23 ± 2.29 mm (range 4–14 mm),and the mean lymph node T/NT was 2.70 ± 1.76 (range 1.1–8.3). In 124 nonmetastatic lymph node stations, the mean lymph node short axis diameter was 6.78 ± 3.08 mm (range 3–18 mm),and the mean lymph node T/NT was 1.11 ± 0.29 (range 1.0–2.8). The differences in lymph node size and T/NT between the two groups were statistically significant (all P < 0.001). Of the 22 metastatic lymph node stations, 17 stations were not enlarged by CECT, of which 13 stations were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT, and 4 stations were found to have no increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. Five stations were enlarged by CECT, all of which were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. Of the 124 nonmetastatic lymph node stations, 109 stations were not enlarged by CECT, of which 2 stations were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. Fifteen stations were enlarged by CECT, of which 8 stations were found to have no increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. The pathological manifestations of those patients with abnormal radioactive uptake increase in nonmetastatic lymph nodes were inflammatory proliferation reactions. Of the 30 nonsurgery patients with regional lymph node metastasis diagnosis based on lymph node biopsy pathology and follow-up imaging, all these nonsurgery patients had lymph node metastasis. In 118 metastatic lymph node stations, the mean lymph node short axis diameter was 14.65 ± 5.91 mm(range 7–52 mm), and the mean lymph node T/NT was 2.10 ± 0.82 (range 1.2–5.8). All 118 metastatic lymph node stations were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT, of which 101 stations were enlarged by CECT. Among 25 patients with incorrect N staging on CECT, 10 patients were overestimated (15.87%), and 15 patients were underestimated (23.81%). Among 7 patients with incorrect N staging on 99mTc-CNDG SPECT/CT, 6 patients were overestimated (9.52%), and 1 patient was underestimated (1.59%).
M staging accuracy
No distant metastasis was found in the clinicopathological diagnosis of the 33 surgical patients, while 20 of the 30 nonsurgical patients were diagnosed with distant metastasis based on biopsy pathology and follow-up imaging. In 20 patients with distant metastasis, a total of 34 distant metastatic lesions with high uptake of 99mTc-CNDG were found, the mean metastatic lesions T/NT was 2.58 ± 0.86 (range 1.5–6.1).There were 6 patients with pleural metastasis, and both CECT and 99mTc CNDG SPECT/CT were positive. There were 5 patients with contralateral lung metastasis who were positive on CECT, and 4 patients who were positive on 99mTc-CNDG SPECT/CT. There were 9 patients with bone metastasis who were positive on 99mTc-CNDG SPECT/CT. Only 4 patients showed abnormal bone density by CECT. In 1 patient with osteoclastic bone metastasis in the rib detected by CT, 99mTc-CNDG SPECT/CT showed an abnormal radioactive uptake increase, while 99mTc-MDP bone imaging showed no abnormal radioactive uptake. There were 2 patients with benign bone lesions with abnormal bone density on CT that was suspected to be bone metastases, and 99mTc-CNDG SPECT/CT and 99mTc-MDP bone imaging confirmed that there were no abnormalities. There were 3 patients with adrenal metastasis, all of whom were positive on CECT, 1 patient was positive on 99mTc-CNDG SPECT/CT, and 2 patients did not show any adrenal metastasis on 99mTc-CNDG SPECT/CT due to the high radioactive distribution near the kidney. There was 1 patient with liver metastasis and 1 patient with subcutaneous metastasis, and both CECT and 99mTc CNDG SPECT/CT were positive. Among 6 patients with incorrect M staging on CECT, 1 patient was overestimated (1.59%), and 5 patients were underestimated (7.94%). Both patients with incorrect M staging on 99mTc-CNDG SPECT/CT were underestimated (3.17%).
The comparison of TNM staging accuracy
For all patients and surgical patients who underwent postoperative pathology, the accuracies of 99mTc-CNDG SPECT/CT in diagnosing T stage and N stage were higher than those of CECT, and the differences were statistically significant. For all patients, the accuracy of 99mTc-CNDG SPECT/CT in diagnosing M staging was higher than that of CECT, but the difference was not statistically significant. The comparison of the diagnostic accuracy of TNM stage between the two methods is presented in Table 2. The staging diagnoses of 99mTc-CNDG SPECT/CT and CECT in surgical patients and in nonsurgical patients are shown in Figs. 1 and 2, respectively.

Representative case of surgery. A 50-year-old female with lung adenocarcinoma in the right upper lobe, postoperative pathological stage T3N2bM0. CECT image (A) showed that the lobulated primary tumor (arrow) and distal strip shadow (arrowhead) of the right upper lobe were abnormally enhanced, which was suspected to be right upper lung cancer complicated with obstructive pneumonia. 99mTc-CNDG fusion SPECT/CT image (B) confirmed that the primary tumor (arrow) and distal lesion (arrowhead) were highly CNDG-avid, suggesting right upper lung cancer complicated with intrapulmonary metastasis. CECT image (C) showed that the lobulated primary tumor (arrow) of the right upper lobe and slightly larger lymph node station 4R (arrowhead) were abnormally enhanced. 99mTc-CNDG fusion SPECT/CT images (D) confirmed that the primary tumor (arrow) and lymph node station 4R (arrowhead) were highly CNDG-avid, and metastatic lymph node station 4R, which was not confirmed by CECT, was definitively diagnosed by 99mTc-CNDG SPECT/CT. CECT image (E) showed abnormal enhancement of obviously enlarged lymph node station 7 (arrowhead). 99mTc-CNDG fusion SPECT/CT images (F) showed that there was no abnormal increase in CNDG in lymph node station 7 (arrowhead), and nonmetastatic lymph node station 7, which was misdiagnosed by CECT, was correctly diagnosed by 99mTc-CNDG SPECT/CT. Postoperative pathology confirmed that the lesion far from the primary tumor of the right upper lobe was an intrapulmonary metastasis, lymph node station 4R was metastasis and lymph node station 7 was nonmetastasis. Compared with CECT, 99mTc-CNDG SPECT/CT accurately diagnosed intrapulmonary metastases and differentiated mediastinal lymph node metastasis

Representative case of nonsurgery. A 60-year-old male with large cell carcinoma in the left lower lobe, clinicopathological staging T4N2aM1c. CECT image (A) showed that the nodular primary tumor (arrow) of the left lower lobe and pleural nodule (arrowhead) were abnormally enhanced. 99mTc-CNDG fusion SPECT/CT image (B) showed that the primary tumor (arrow) and pleural nodule invading the left 6th anterior rib (arrowhead) were highly CNDG-avid, suggesting that the tumor had invaded the adjacent rib. A diagnostic bone window CT image (C) showed that the density of the left 6th anterior rib (arrow) near the pleural metastasis was normal. 99mTc-MDP fusion SPECT/CT bone image (D) and anterior 99mTc-MDP whole-body bone image (E) confirmed left 6th anterior rib metastasis (arrow) and left 7th anterior rib metastasis (arrowhead). Compared with CECT, 99mTc-CNDG SPECT/CT accurately diagnosed the invasion of bone by pleural metastasis of lung cancer
Potential respectability
To compare the accuracies of 99mTc-CNDG SPECT/CT and CECT in evaluating the potential resectability of NSCLC, the areas under the ROC curve of the two methods were calculated, as shown in Fig. 3. The accuracy of 99mTc-CNDG SPECT/CT in evaluating the potential resectability of NSCLC was significantly higher than that of CECT (P = 0.046).

Graph illustrating receiver operating characteristic curves for the potential resectability of tumors with 99mTc-CNDG SPECT/CT and CECT. Potential resectability of a tumor was defined as a T stage below 4, an N stage below 3, and an M stage of 0 (99mTc-CNDG SPECT/CT: area under the curve, 0.97; 95% confidence interval, 0.89–1.00 [P = 0.023]; CECT: area under the curve, 0.87; 95% confidence interval, 0.76–0.94 [P = 0.043])
Discussion
TNM staging of NSCLC is a standard method to determine the tumor range based on the characteristics of the primary tumor, regional lymph node and distant metastasis, which is the pillar of clinical treatment decision and prognosis evaluation of NSCLC, and the resectability of NSCLC patients can be accurately evaluated according to TNM staging (Leiro-Fernández and Fernández-Villar 2021). CECT structural images can be used to diagnose obvious local, mediastinal and distant invasion by showing tumor size, morphology, pulmonary nodules, pleural nodules, pericardial nodules, lymphadenopathy, adrenal nodules and abnormal bone density, but the diagnostic accuracy is poor for slightly atypical invasion and metastasis. Thus, CECT is unreliable for accurate staging of NSCLC (Volpi et al. 2018). Molecular imaging of nuclear medicine with functional metabolism can be used to accurately diagnose malignant tumors at an early stage. In recent years, 18F-FDG PET/CT has become a widely and frequently used imaging method in the diagnosis and staging of NSCLC (Werutsky et al. 2019; Ohno et al. 2020; Zhang et al. 2023). A study of Volpi et al. reviewed the impact of 18F-FDG PET/CT on patient staging and management in NSCLC, the results showed that 18F-FDG PET/CT changed 25.3%–62.0% of the TNM stages of NSCLC, which led to changes in the clinical decision-making of 19.0%–52.0% of patients (Volpi et al. 2018). At present, 18F-FDG PET/CT has been recommended in many international guidelines for clinical TNM staging of NSCLC (Volpi et al. 2018; Ohno et al. 2020; Zhang et al. 2023).
Similar to 18F-FDG, the hydroxyl group of glucosamine C2 is replaced by an amino group. Glucosamine and glucose share a common metabolic pathway, and their amino groups play a dual role as coordination sites and functional targets (Feng et al. 2019; Zhang et al. 2018; Yang et al. 2003). Studies have shown that glucosamine retains the metabolic activities of Gluts and HK even in the case of large coordination groups, and 99mTc-labeled glucosamine is also located in the nucleus through the biosynthesis path of hexosamine (Yang et al. 2012). To date, 99mTc-ethylenedicystine deoxyglucosamine (ECDG) and 99mTc-CNDG are the most representative, and 99mTc-ECDG has entered a phase III clinical study (Zhang et al. 2018). A preliminary clinical study of 99mTc-ECDG SPECT/CT in early evaluation of the response of nine patients with locally advanced head and neck squamous cell carcinoma after radiochemotherapy showed that 99mTc-ECDG SPECT/CT accurately predicted the treatment response of 7 patients (77.8%) (Ginat et al. 2017). Recently, (Dai et al. (2018) reported a clinical study of 17 patients with NSCLC confirmed by biopsy, in which 99mTc-ECDG SPECT/CT was used to detect and stage the tumor. The results showed that although the tumor uptake of 99mTc-ECDG was low and the blood background was high compared with 18F-FDG, the coincidence rate of 99mTc-ECDG in detecting the primary tumor and metastatic lesion reached 100% and 70%, respectively, and the diagnostic efficiencies of 99mTc-ECDG SPECT/CT for primary tumor and metastatic lesions of lung cancer were not inferior to those of 18F-FDG PET/CT. Studies have confirmed that unlike 18F-FDG and other 99mTc-labeled glucose derivatives, the uptake of 99mTc-CNDG by malignant tumor cells is related not only to Gluts but also to the hydrophilic cation characteristics of CNDG, which increase its uptake by malignant tumor cells through its transmembrane negative potential (Zhang et al. 2018; Zhou and Liu 2011). Preclinical animal experiments showed that the tumor uptake rate and T/NT of 99mTc-CNDG were significantly higher than those of previous various glucose derivatives labeled with 99mTc, which can clearly display malignant tumors with a diameter of 3 mm (Zhang et al. 2018). Recently, Wang et al. (Wang et al. 2021) prospectively studied the diagnostic efficiencies of 99mTc-CNDG SPECT/CT and CECT in 95 patients with lung cancer. The results showed that the sensitivity, specificity and accuracy of 99mTc-CNDG SPECT/CT in diagnosing lung cancer were higher than those of CECT (97.5%, 76.5%, 93.8% vs. 87.5%, 41.2%, 79.4%, respectively), and the differences in sensitivity and accuracy were statistically significant (all P < 0.05). Wang et al. (2023) another recent study investigated the value of 99mTc-CNDG SPECT/CT in the diagnosis of regional lymph node metastasis in NSCLC. The study found the sensitivity, specificity, accuracy, positive predictive value and negative predictive value of 99mTc-CNDG SPECT/CT in the diagnosis of regional lymph node metastasis were significantly higher than those of CECT (84.6%, 93.2%, 92.1%, 64.7% and 97.6% vs. 46.2%, 84.1%, 79.2%, 30.0% and 91.4%, respectively), there were significant differences in specificity and accuracy between the two groups (χ2 = 6.40, 9.94, both P < 0.05). The accuracy of 99mTc-CNDG SPECT/CT in diagnosing N-stage of NSCLC patients was significantly higher than that of CECT (81.0% vs. 52.4%; P = 0.031).The authors concluded that It was more effective to precisely validate regional lymph node metastasis of NSCLC by using 99mTc-CNDG SPECT/CT than by using CECT, 99mTc-CNDG SPECT/CT could provide a better basis for preoperative staging and treatment decision making of NSCLC.
In this study, the sodium pertechnetium solution used in 99mTc-CNDG SPECT/CT was supplied from the inside of a molybdenum technetium generator, while CNDG allowed for the supplyment to be available in kit form. The preparation of 99mTc-CNDG was simple and effective. This research proved that 99mTc-CNDG SPECT/CT imaging had the advantages of good quality, low price, convenient method and technically wide accessibility. In this study, the efficacy of 99mTc-CNDG SPECT/CT and CECT in TNM staging of NSCLC was compared for the first time. The study showed that 99mTc-CNDG SPECT/CT could accurately distinguish the boundary between atelectasis, obstructive pneumonia and malignant lung tumors and accurately diagnose abnormal nodular radioactivity increases in lung metastases and tumor invasion to the pleura and pericardium. The study showed that 99mTc-CNDG SPECT/CT could be used to accurately diagnose metastatic and nonmetastatic lymph nodes in NSCLC, especially normal size metastatic lymph nodes and enlarged nonmetastatic lymph nodes. The study also showed that 99mTc-CNDG SPECT/CT could diagnose bone metastases early without pathological bone density abnormalities and osteoclastic bone metastases without abnormal radioactivity increases by 99mTc-MDP bone imaging and correct the diagnosis of patients who were misdiagnosed with bone metastases by CT bone density abnormalities. The accurate diagnosis of 99mTc-CNDG SPECT/CT on the invasion range of the primary tumor, regional lymph node metastasis and distant metastasis made it better than CECT in accurately evaluating the potential resectability of NSCLC. Accurate staging of NSCLC TNM by 99mTc-CNDG SPECT/CT was helpful for clinical treatment decision and improvement of patient's prognosis. However, there were some problems in 99mTc-CNDG SPECT/CT, including the inherent limitation of image resolution and the detection sensitivity of SPECT/CT, higher peripheral blood background, higher bone joint uptake and higher distribution of liver and kidney, which would be expected to be solved in the future with the development of cadmium zinc telluride digital detection technology, image postprocessing technology and further research of CNDG. We believed that 99mTc-CNDG SPECT/CT would show better value in tumor diagnosis and staging with the new digital SPECT/CT entering clinical research and CNDG biochemical design improving the specific targeting of tumor uptake.
The limitations of this study include the following. (1) This study was a single-center study with a small sample size and had selection bias in patient collection. (2) There was no 18F-FDG PET/CT in our hospital, so there was no comparative study with 18F-FDG PET/CT in the same period. (3) The research reference standard was not the pathological TNM staging in all lesions, and there was a deviation in the evaluation of imaging diagnostic performance. (4) The imaging range of this study was limited to the clavicular area to the upper abdomen, and the potential value of 99mTc-CNDG SPECT/CT in diagnosing brain metastasis was not evaluated. A 74 year male patient with left upper lung adenocarcinoma who was not included in this study underwent brain 99mTc-CNDG SPECT/CT without completing upper abdomen 99mTc-CNDG SPECT/CT. The brain 99mTc-CNDG SPECT/CT clearly showed multiple obviously abnormal hyperuptake foci in the occipital lobe of the brain, and the low normal brain background which were potentially superior to 18F-FDG PET/CT. The diagnosis was confirmed by brain MR.
Conclusions
This preliminary clinical study shows that 99mTc-CNDG SPECT/CT is of great value for accurate clinical staging of NSCLC compared with conventional CECT and that 99mTc-CNDG SPECT/CT can significantly improve the accuracy of resectability diagnosis of NSCLC. 99mTc-CNDG SPECT/CT is helpful for clinical treatment decision-making and improving prognosis of patients with NSCLC.99mTc-CNDG SPECT/CT not only has the advantages of low price, convenient methodology and popular technology but also has broad-spectrum features for tumor imaging and a unique mechanism for tumor uptake. Further confirmation of clinical research on 99mTc-CNDG SPECT/CT is expected to bring new prospects for tumor glucose metabolism imaging in nuclear medicine.
Data availability
The data that support the findings of this study are available on request from the corresponding author upon reasonable request.
References
Dai D, Rollo FD, Bryant J et al (2018) Noninferiority of 99mTc-ethylenedicysteine-glucosamine as an alternative analogue to 18F-fluorodeoxyglucose in the detection and staging of non-small cell lung cancer. Contrast Media Mol Imaging 2018:8969714
Detterbeck FC, Boffa DJ, Kim AW et al (2017) The eighth edition lung cancer stage classification. Chest 151(1):193–203
Feng H, Wang X, Chen J et al (2019) Nuclear imaging of glucose metabolism: beyond 18F-FDG. Contrast Media Mol Imaging 26(5):7954854
Gan Q, Zhang X, Ruan Q et al (2021) 99mTc-CN7DG: a highly expected SPECT imaging agent of cancer with satisfactory tumor uptake and tumor-to-nontarget ratios. Mol Pharm 18(3):1356–1363
Ginat DT, Westiin C, Brisson RJ et al (2017) Pilot study of 99mTc-labeled ethylene dicysteine deoxyglucose SPECT-CT imaging in treatment response evaluation in patients with locally advanced head and neck cancer. Cureus 9(4):e1152
Kandathil A, Kay FU, Butt YM et al (2018) Role of FDG PET/CT in the eighth edition of TNM staging of non-small cell lung cancer. Radiographics 38(7):2134–2149
Leiro-Fernández V, Fernández-Villar A (2021) Mediastinal staging for non-small cell lung cancer. Transl Lung Cancer Res 10(1):496–505
Meng L, Xiu Y, Li Y et al (2015) Investigations of (99m)Tc-labeled glucarate as a SPECT radiotracer for non-small cell lung cancer (NSCLC) and potential tumor uptake mechanism. Nucl Med Biol 42(7):608–613
Ohno Y, Takeshi Y, Takenaka D et al (2020) Comparison of diagnostic accuracy for TNM stage among whole-body MRI and Coregistered PET/MRI using 1.5-T and 3-T MRI systems and integrated PET/CT for non-small cell lung cancer. AJR Am J Roentgenol 215(5):1191–1198
Reckzeh ES, Waldmann H (2020) Small-molecule inhibition of glucose transporters GLUT-1-4. ChemBioChem 21(1–2):45–52
Rusch VW, Asamura H, Watanabe H et al (2009) Members of IASLC staging committee. The IASLC lung cancer staging project: a proposal for a new international lymph node map in the forthcoming seventh edition of the TNM classification for lung cancer. J Thorac Oncol 4(5):568–577
Travis WD, Brambilla E, Noguchi M et al (2011) International association for the study of lung cancer/American thoracic society/European respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol 6(2):244–285
Vansteenkiste J, De Ruysscher D, Eberhardt WE et al (2013) ESMO guidelines working group. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 24(Suppl 6):89–98
Volpi S, Ali JM, Tasker A et al (2018) The role of positron emission tomography in the diagnosis, staging and response assessment of non-small cell lung cancer. Ann Transl Med 6(5):95
Wang QF, Qin JJ, Xu YZ et al (2021) Clinical Research on 99Tcm-isonitrile deoxyglucosamine single photon emission computed tomography/computed tomography for lung cancer diagnosis. Chin J Clin Oncol 48(21):1125–1128
Wang QF, Qin JJ, Xu YZ et al (2023) Clinical research on 99mTc-isonitrile deoxyglucosamine SPECT/CT for diagnosis of regional lymph node metastasis in NSCLC. Chin J of Medical Imaging 31(6):606–610
Werutsky G, Hochhegger B, de Figueiredo L, Pinto JA et al (2019) PET-CT has low specificity for mediastinal staging of non-small-cell lung cancer in an endemic area for tuberculosis: a diagnostic test study (LACOG 0114). BMC Cancer 19(1):5
Yang DJ, Kim CG, Schechter NR et al (2003) Imaging with 99mTc ECDG targeted at the multifunctional glucose transport system: feasibility study with rodents. Radiology 226(2):465–473
Yang DJ, Kong FL, Oka T et al (2012) Molecular imaging kits for hexosamine biosynthetic pathway in oncology. Curr Med Chem 19(20):3310–3314
Zhang X, Ruan Q, Duan X et al (2018) Novel 99mTc-labeled glucose derivative for single photon emission computed tomography: a promising tumor imaging agent. Mol Pharm 15(8):3417–3424
Zhang X, Ruan Q, Jiang Y et al (2021) Evaluation of 99mTc-CN5DG as a broad-spectrum SPECT probe for tumor imaging. Transl Oncol 14(1):100966
Zhang C, Liang Z, Liu W et al (2023) Comparison of whole-body 18F-FDG PET/CT and PET/MRI for distant metastases in patients with malignant tumors: a meta-analysis. BMC Cancer 23(1):37
Zhou Y, Liu S (2011) 64Cu-labeled phosphonium cations as PET radiotracers for tumor imaging. Bioconjug Chem 22(8):1459–1472
Funding
This work was partially supported by Sanya medical and health technology innovation project (grants 2019YW05).
Author information
Authors and Affiliations
Contributions
Author 1: Ideas, Methodology, Management; Author 2: Patient enrollment, surgical treatment; Author 3: Program, Patient follow-up; Author 4: Radiochemotherapy, Validation; Author 5: Image analysis, Oversight and consult; Author 6: Data/evidence collection, image acquisition, quality control.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Q., Deng, Z., Lu, C. et al. A prospective study to compare the diagnostic accuracy of 99mTc-CNDG SPECT/CT and contrast-enhanced CT in staging of non-small cell lung cancer. J Cancer Res Clin Oncol 150, 430 (2024). https://doi.org/10.1007/s00432-024-05953-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00432-024-05953-6