
Abstract
Purpose
Proper management of subcentimeter thyroid nodules remains challenging for both clinicians and patients. Conducting extensive sonographic research using a safe and inexpensive tool for identifying thyroid nodules is necessary. The aim of this study was to identify whether having the highest-risk ultrasound (US) characteristic suggests that US-guided fine-needle aspiration (FNA) biopsy of subcentimeter nodules is more appropriate for the identification of malignancy than active surveillance (AS) or surgery.
Methods
The data of patients with highly suspicious subcentimeter thyroid nodules and US characteristic data who underwent surgery were retrospectively examined.
Results
Among a total of 556 subcentimeter nodules, 223 (40.1%) were benign, and 333 (59.9%) were malignant, with a mean maximal nodule size of 8.1 mm. In addition to age younger than 45 years, several US features were significantly associated with malignancy: irregular margins, the presence of microcalcifications, and taller-than-wide shapes (P < 0.001). Multivariate analysis also revealed that a taller-than-wide shape (OR = 8.988, P = 0.0015) was an independent factor associated with malignancy in subcentimeter thyroid nodules. The diagnostic performance of preoperative FNA was classified as a malignancy, with a sensitivity of 98.4%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 76.9%.
Conclusions
This is one of the few reports based on actual data of the most suspicious US features in subcentimeter thyroid nodules. A taller-than-wide shape US feature is most significantly associated with malignancy. FNA is a simple, accurate, and reliable preoperative method for diagnosing malignant subcentimeter thyroid nodules with highly suspicious US characteristics. AS was less appropriate than FNA for subcentimeter nodules with a taller-than-wide shape, especially in patients ≤ 45 years of age.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The widespread use of ultrasound (US) screenings and US-guided fine-needle aspiration (FNA) biopsies has led to a rapid increase in the number of identified thyroid malignancies in recent decades. This in turn has led to an increasing trend of overdiagnosis and overtreatment of small papillary thyroid carcinoma (PTC) (Vaccarella et al. 2015; Furuya-Kanamori et al. 2016). The revised American Thyroid Association (ATA) guidelines, published in 2015 (Haugen et al. 2015), recommend FNA biopsy only for nodules > 1 cm in size with US feature patterns that appear intermediately and are highly suspicious. However, FNA biopsy can also be used to assess nodules in the subcentimeter range that exhibit highly suspicious US features. Furthermore, a large percentage of thyroid nodules that do not meet the FNA indications are aspirated in medical practice (Jeong et al. 2020), reflecting risk aversion among clinicians who are concerned about missing malignancies.
Active surveillance (AS) is a possible alternative to surgical treatment for subcentimeter PTC, especially when cytopathological findings (refer to the Bethesda System) (Ali et al. 2023) are convincing and there is no evidence of local invasion, metastasis, or aggressive disease (Haugen et al. 2015). As the rates of disease-specific mortality and disease recurrence are minimal and thyroid surgery for the treatment of subcentimeter PTC has no proven benefits, the ATA (2015), ACR (2017) (Tessler et al. 2017), and European Thyroid Association (2017) guidelines (Russ et al. 2017) (Table 1) recommend the management of subcentimeter thyroid nodules with AS. However, while AS can be used to avoid the complications and adverse events associated with surgery, patients who are concerned about tumours remaining untreated or metastasizing are at risk of experiencing psychological stress (Yeh et al. 2015), especially when US reveals thyroid nodules that are highly suspicious of malignancy. Therefore, as reported in a previous study, the number of FNA biopsies or surgeries has increased rather than decreased because of the frequent detection of nodules in the subcentimeter range that appear highly suspicious on US. Moreover, patients with malignant subcentimeter nodules generally opt for surgery rather than AS (Jeong et al. 2020).
The revised ATA guidelines define highly suspicious US features as a solid or mainly solid hypoechoic nodule with at least one of the following characteristics: microcalcifications, taller-than-wide dimensions, rim calcifications with a noticeable soft-tissue component, irregular margins, or extrathyroidal extension (ETE) (Haugen et al. 2015). The American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) assigns three points to microcalcifications or taller-than-wide dimensions (Tessler et al. 2017). Thus, both guidelines define high-risk US characteristics of malignancy similarly.
In this study, we investigated whether the presence of relatively high-risk US characteristics indicates that subcentimeter nodule FNA is more appropriate for the identification of malignancy than AS or surgery to help clinicians evaluate benign or malignant subcentimeter nodules during follow-up.
Materials and methods
Study design and patient population
We retrospectively assessed the data of patients with thyroid nodules in the subcentimeter range exhibiting highly suspicious characteristics on US who had undergone surgery at our hospital from July 2018 to December 2019. We applied the following inclusion criteria: (1) preoperative US showing features highly suggestive of malignancy, (2) surgical treatment, and (3) diagnosis via pathological examination after surgery. The exclusion criteria were as follows: (1) incomplete preoperative US data, (2) thyroid nodules not confirmed via pathological examination, and (3) previous thyroid surgery.
Assessment
Two physicians experienced in thyroid US performed the examinations. US nodule features, clinical characteristics, US features (nodule size, content, echogenicity, margins, calcification, shape, and presence of cervical lymph nodes), and histopathology results after surgery were recorded. Patients with solitary thyroid lesions showing no involvement of the nodes underwent hemithyroidectomy, and those with multifocality, ETE, or lateral lymph node metastasis were treated with total thyroidectomy. Routine central neck dissection (bilateral or ipsilateral) was performed prophylactically during partial and total thyroidectomy, and the levels of free triiodothyronine, free thyroxine, thyroid-stimulating hormone, thyroid peroxidase antibodies, and thyroglobulin were assessed before surgery.
In this study, a total of 609 subcentimeter thyroid nodules in 601 patients were assessed, and the remaining 556 nodules in 556 patients had US features that were classified as highly suspicious; 223 nodules (40.1%) were benign, and 333 (59.9%) were malignant (Fig. 1).

Flow chart of the study
Ethical approval
The Institutional Review Board of the First Affiliated Hospital of Xiamen University approved the study protocol (2020-No.035).
Statistical analysis
Categorical variables were analysed using Chi-square tests or Fisher's exact test, while rank-sum tests or independent t tests were applied to continuous variables. Clinical factors and US features with significant differences were evaluated using multivariate logistic regression analysis to identify characteristics that are independently associated with malignant thyroid nodules and their invasive biological behaviours (cervical lymph node metastasis).
We applied the following criteria to the cytopathology results of subcentimeter nodules that had undergone preoperative FNA to determine the sensitivity, specificity, positive and negative predictive value (PPV, NPV), and diagnostic accuracy. Nodules were determined to be FNA-positive when they had been given the label “suspicious for malignancy” or “malignancy” (both corresponding to a highly suspicious ultrasonographic pattern according to the ATA guidelines); those labelled “benign” were considered FNA-negative. Statistical analyses were conducted using SAS version 9.3, and a P value < 0.05 was considered to indicate statistical significance. The 95% confidence intervals are displayed for all the results.
Results
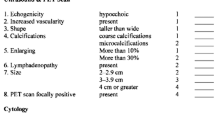
In the present study, the mean maximal nodule size was 8.1 mm. Table 2 lists the detailed characteristics of all the nodules. The following malignancies were diagnosed: papillary carcinoma (n = 331), medullary carcinoma (n = 1), and follicular carcinoma (n = 1). Univariate analysis revealed that irregular margins, microcalcifications, taller-than-wide dimensions, and age < 45 years were factors associated with malignancy (P < 0.001) (Table 1), and rim calcification with small extrusive soft tissue components and extrathyroidal extensions were not observed in the subcentimeter nodules included in our study. Furthermore, there was no difference in sex between patients with benign and malignant thyroid nodules. Multivariate analysis revealed that taller-than-wide dimensions (OR = 8.988, P = 0.0015) were independently associated with malignancy in thyroid nodules in the subcentimeter range (Table 3).
The 333 subcentimeter malignant nodules were classified according to US characteristics and clinical features—lymph node metastasis was identified in 57 nodules (17.1%). According to the univariate analysis, taller-than-wide dimensions on US were significantly associated with lymph node metastasis (P < 0.01), while age younger than 45 years was also identified as a significant risk factor (P < 0.05). However, calcifications, irregular margins, and patient sex did not significantly predict subcentimeter thyroid malignant nodules with lymph node metastasis (Table 4). We found that all 223 histologically benign nodules had the following highly suspicious US features: irregular margins (30.49%, n = 68), microcalcifications (17.94%, n = 40), and taller-than-wide shapes (9.49%, n = 21). FNA cytopathology was performed on 162 of the 556 subcentimeter nodules before surgery (Table 5). The diagnostic performance of the preoperative FNA for correctly classifying a nodule as “malignant” was high, with a sensitivity of 98.4%, a specificity of 100%, a PPV of 100%, and an NPV of 76.9%.
Discussion
Proper management of subcentimeter thyroid nodules remains a great challenge for both clinicians and patients. Extensive research on ultrasonography, which is a safe and inexpensive tool for identifying thyroid nodules, is therefore important. While the 2015 ATA guidelines estimated a 70–90% malignancy risk for thyroid nodules > 1 cm in size that appear highly suspicious on US, data for subcentimeter nodules are still lacking. In our sample, 59.9% of highly suspicious thyroid nodules in the subcentimeter range were classified as malignant on postoperative pathological examination. We found that the characteristic US finding of taller-than-wide dimensions allows for the best prediction of malignancy; similar to the results of Frates et al. (2005) and Lee et al. (2011), when this feature was present, the risk of having a malignant tumour was approximately nine times greater than when it was absent. Other studies have also suggested that a taller-than-wide shape on US predicts malignancy with the highest specificity (Ito et al. 2007; Ahn et al. 2010). Specifically, the anteroposterior diameter of the thyroid cancer nodule is usually larger than the transverse diameter, which may be related to the fact that tumour cells in the anteroposterior direction are in the division phase, while those in other directions are relatively static (Moon et al. 2011).
The sensitivity of microcalcification for subcentimeter malignant nodule detection in our sample was low; a previous study reported a sensitivity of 15.2% (Popowicz et al. 2009). Furthermore, we did not observe rim calcifications with ETE or noticeable soft-tissue components, which indicates that these two US features are rarely expressed in subcentimeter thyroid nodules. Earlier studies have investigated risk factors for poor prognoses in patients with papillary thyroid microcarcinoma (PTMC) and have reported that ETE, capsular invasion, and neck lymph node metastasis are independently associated with distant metastasis and nodal recurrence (Mercante et al. 2009; Pisanu et al. 2015). However, the treating physician does not have easy access to such results when assessing patients for subcentimeter nodules before an intervention, which can lead to a poor prognosis. In addition, PTMC is no longer recognized by the WHO 5th edition as an independent histological subtype. This was also the case in this study, where we observed no capsular invasion or ETE and identified only 3 patients with suspicious neck lymph nodes before preoperative US, but lymph node metastases were observed in 57 of 333 malignant nodules by postoperative pathology confirmation. However, we also found that both the characteristic US findings of a taller-than-wide shape and age younger than 45 years were significant risk factors for subcentimeter malignant thyroid nodules with lymph node metastasis and the invasive biological behaviour of malignant tumours. These results are consistent with those of Baier et al. (2009) and Rago et al. (2010).
The presence of highly suspicious US findings helps determine which thyroid nodules require FNA biopsy and reduces the likelihood of over- or misdiagnosis. According to the usual guidelines, FNA should be performed when nodules are > 1 cm in size and have highly suspicious features. However, for thyroid nodules less than 1 cm, existing guidelines generally recommend AS. However, there is no clear documentation for follow-up management. Thus, there is a gap in the literature regarding the appropriate treatment for subcentimeter nodules. In other words, the available guidelines provide clear recommendations regarding thyroid biopsy, and they do not offer a clear and suitable management approach for patients who do not undergo a biopsy. Some studies found a significantly greater frequency of AS in patients with benign biopsy results (83%) than in those without suspicious nodule cytopathology (36%) (Genere et al. 2020). Interestingly, more than 80% of nodules with benign results were still recommended for continued AS. This may stem from the hesitation of clinicians to dismiss the suspicious appearance of a nodule and diagnose it as cytologically benign due to the high probability of malignancy (Brito et al. 2014). The use of AS also reflects a lack of confidence in being able to rule out malignancies. In addition, patients can feel psychologically burdened by concerns about tumours remaining untreated or metastasizing (Yeh et al. 2015) and might want to take future quality of life outcomes into account when making treatment decisions. This study clearly shows that many patients with subcentimeter thyroid nodules that appear highly suspicious on US choose to undergo surgery in our region as well as in China in general. Before performing FNA in such patients, the clinician needs to determine which nodules are most at risk of malignancy.
The results of this study suggest that subcentimeter thyroid nodules that appear highly suspicious on US, particularly those with taller-than-wide dimensions, the most suspicious ultrasound feature, may be recommended for FNA; however, regarding the choice between AS and surgery, because of this patient population’s greater risk (approximately nine times) of having a malignant tumour, the patient’s preference needs to be taken into account. The diagnostic accuracy of FNA in our sample was greater than expected, with high sensitivity and specificity and a 100% PPV. FNA is therefore a simple, accurate, and reliable preoperative diagnostic method for detecting thyroid nodules in the subcentimeter range that appear highly suspicious on US. It can also help in diagnosis and has proven clinical value. If a patient is younger than 45 years and has a nodule with a diameter < 1 cm and a taller-than-wide shape, AS should not be considered for management. Instead, FNAs or surgical interventions could be selected according to the patient's preference, and patients experiencing fear or anxiety related to the progression of their disease should be offered additional support.
We found that one specific malignant US feature alone cannot be used to determine the malignancy risk of a thyroid nodule; this must be done based on a combination of multiple signs. An increase in the number of suspicious features thus suggests a subsequent increase in the risk of malignancy. Because of the limited number of patients with two or more suspicious features on US, we did not conduct further research, which may have reduced the statistical power for identifying differences. The risk of malignancy increases with the accumulation of highly suspicious US features, reaching 97.9% if all highly suspicious US features are present (Jin Young et al. 2011).
The current study has the following advantages. (1) There was a large sample size. (2) Compared with those in other studies, all subcentimeter nodules with suspicious features within our cohort were diagnosed by pathological examination, with relatively few nodules undergoing puncture cytopathology and postoperative pathology. (3) Our separate analysis of the correlations between single US features and pathological properties of subcentimeter thyroid nodules may provide useful reference data for clinical management.
Limitations of the study
A limitation of this study is its single-centre retrospective observational cohort design. We excluded patients who had not undergone surgery or who were potentially missing many highly suspicious nodule US features that were not confirmed pathologically but were benign. Additionally, some enrolled patients exhibited two to three highly suspicious US features, thus increasing the likelihood of malignancy. This may have resulted in a bias towards the ‘A’ malignancy rate of 59.9% in this study. Furthermore, we were not able to comprehensively correct for some potentially confounding factors. For example, the patient's family history, occupational factors (i.e., radiation exposure), body mass index, and eating habits (i.e., excessive iodine intake) have been associated with an increased risk of thyroid cancer (Babić Leko et al. 2023). Prospective studies are warranted to further verify the results of this study. Health-related quality-of-life questionnaires, the Thyroid Cancer-Specific Quality of Life questionnaire, and the Fear of Disease Progression Questionnaire may also be useful in determining a patient's status when deciding between surgical and nonsurgical treatment. The presence of features in each of the categories in Table 5 was associated with a greater risk of malignancy (ROM) than expected according to the 2023 Bethesda System for Reporting Thyroid Cytopathology. We selected to puncture subcentimeter nodules with highly suspicious US features, which may have led to a greater proportion of postoperative pathological malignancies. In addition, the limited number of patients who underwent FNA may bias the results, and in our future research, more subcentimeter nodules need to be punctured before surgery.
Conclusions
This is one of the few reports based on actual data of the most suspicious US features in subcentimeter thyroid nodules. Our multivariate analysis revealed that a taller-than-wide shape is the US feature most significantly associated with malignancy. FNA biopsies and surgical operations are often performed in clinical settings, especially for subcentimeter nodules. Moreover, AS may not be the best choice for subcentimeter nodules with taller-than-wide dimensions on US, especially for patients younger than 45 years of age. This was also identified as a significant risk factor for subcentimeter nodules because of the high malignancy rate and often aggressive behaviour.
Data availability
No datasets were generated or analysed during the current study.
References
Ahn SS, Kim EK, Kang DR, Lim SK, Kwak JY, Kim MJ (2010) Biopsy of thyroid nodules: comparison of three sets of guidelines. AJR Am J Roentgenol 194(1):31–37. https://doi.org/10.2214/AJR.09.2822
Ali SZ, Baloch ZW, Cochand-Priollet B et al (2023) The 2023 Bethesda System for reporting thyroid cytopathology [J]. Thyroid 33(9):1039–1044
Babić Leko M, Jureško I, Rozić I, Pleić N, Gunjača I, Zemunik T (2023) Vitamin D and the thyroid: a critical review of the current evidence [J]. Int J Mol Sci. https://doi.org/10.3390/ijms24043586
Baier ND, Hahn PF, Gervais DA, Samir A, Halpern EF, Mueller PR, Harisinghani MG (2009) Fine-needle aspiration biopsy of thyroid nodules: experience in a cohort of 944 patients. AJR Am J Roentgenol 193(4):1175–1179. https://doi.org/10.2214/AJR.08.1840
Brito JP, Gionfriddo MR, Al Nofal A, Boehmer KR, Leppin AL, Reading C, Callstrom M, Elraiyah TA, Prokop LJ, Stan MN, Murad MH (2014) The accuracy of thyroid nodule ultrasound to predict thyroid cancer: systematic review and meta-analysis. J Clin Endocrinol Metab 99(4):1253–1263. https://doi.org/10.1210/jc.2013-2928
Frates MC, Benson CB, Charboneau JW, Cibas ES, Clark OH, Coleman BG, Cronan JJ, Doubilet PM, Evans DB, Goellner JR, Hay ID, Hertzberg BS, Intenzo CM, Jeffrey RB, Langer JE, Larsen PR, Mandel SJ, Middleton WD, Reading CC, Sherman SI, Tessler FN, Society of Radiologists in Ultrasound (2005) Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology 237(3):794–800. https://doi.org/10.1148/radiol.2373050220
Furuya-Kanamori L, Bell KJL, Clark J, Glasziou P (2016) Prevalence of differentiated thyroid cancer in autopsy studies over six decades: a meta-analysis. J Clin Oncol 34(30):3672–3679. https://doi.org/10.1200/JCO.2016.67.7419
Genere N, Hurtado MD, Cortes T, Athimulam S, Al Ward R, Callstrom MR, Stan MN, Morris JC, Brito JP (2020) Drivers of the decision to biopsy and follow-up of small suspicious thyroid nodules. Endocr Pract 26(8):857–868. https://doi.org/10.4158/EP-2019-0590
Haugen BRM, Alexander EK, Bible KC et al (2015) American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid 26(1):1–133. https://doi.org/10.1089/thy.2015.0020
Ito Y, Amino N, Yokozawa T, Ota H, Ohshita M, Murata N, Morita S, Kobayashi K, Miyauchi A (2007) Ultrasonographic evaluation of thyroid nodules in 900 patients: comparison among ultrasonographic, cytological, and histological findings. Thyroid 17(12):1269–1276. https://doi.org/10.1089/thy.2007.0014
Jeong C, Kim H, Lee J, Ha J, Kim MH, Kang MI, Lim DJ (2020) Fine-needle aspiration of subcentimeter thyroid nodules in the real-world management. Cancer Manag Res 12:7611–7618. https://doi.org/10.2147/CMAR.S263451
Jin Young K, Kyung Hwa H, Jung Hyun Y, Hee Jung M, Eun Ju S, So Hee P (2011) Thyroid imaging reporting and data system for US features of nodules: a step in establishing better stratification of cancer risk [J]. Int J Med Radiol 260(3):892. https://doi.org/10.1148/radiol.11110206
Lee EJ, Song KH, Kim DL, Jang YM, Hwang TS, Kim SK (2011) The BRAF(V600E) mutation is associated with malignant ultrasonographic features in thyroid nodules. Clin Endocrinol (oxf) 75(6):844–850. https://doi.org/10.1111/j.1365-2265.2011.04154.x
Mercante G, Frasoldati A, Pedroni C, Formisano D, Renna L, Piana S, Gardini G, Valcavi R, Barbieri V (2009) Prognostic factors affecting neck lymph node recurrence and distant metastasis in papillary microcarcinoma of the thyroid: results of a study in 445 patients. Thyroid 19(7):707–716. https://doi.org/10.1089/thy.2008.0270
Moon HJ, Kwak JY, Kim EK et al (2011) A taller-than-wide shape in thyroid nodules in transverse and longitudinal ultrasonographic planes and the prediction of malignancy [J]. Thyroid 11:21. https://doi.org/10.1089/thy.2010.0372
Pisanu A, Saba A, Podda M, Reccia I, Uccheddu A (2015) Nodal metastasis and recurrence in papillary thyroid microcarcinoma. Endocrine 48(2):575–581. https://doi.org/10.1007/s12020-014-0350-7
Popowicz B, Klencki M, Lewiński A, Slowinska-Klencka D (2009) The usefulness of sonographic features in selection of thyroid nodules for biopsy in relation to the nodule’s size. Eur J Endocrinol 161(1):103–111. https://doi.org/10.1530/EJE-09-0022
Rago T, Fiore E, Scutari M, Santini FE, Di Coscio G, Romani R, Piaggi PA, Ugolini C, Basolo FU, Miccoli PA, Pinchera AL (2010) Male sex, single nodularity, and young age are associated with the risk of finding a papillary thyroid cancer on fine-needle aspiration cytology in a large series of patients with nodular thyroid disease. Eur J Endocrinol 162(4):763–770. https://doi.org/10.1530/EJE-09-0895
Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L (2017) European Thyroid Association Guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: the EU-TIRADS [J]. Eur Thyroid J 6(5):225–237
Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, Teefey SA, Cronan JJ, Beland MD, Desser TS, Frates MC, Hammers LW, Hamper UM, Langer JE, Reading CC, Scoutt LM, Stavros AT (2017) ACR thyroid imaging, reporting and data system (ti-rads): white paper of the ACR TI-RADS committee. J Am Coll Radiol 14(5):587–595. https://doi.org/10.1016/j.jacr.2017.01.046
Vaccarella S, Dal Maso L, Laversanne M, Bray F, Plummer M, Franceschi S (2015) The impact of diagnostic changes on the rise in thyroid cancer incidence: a population-based study in selected high-resource countries. Thyroid 25(10):1127–1136. https://doi.org/10.1089/thy.2015.0116
Yeh MW, Bauer AJ, Bernet VA, Ferris RL, Loevner LA, Mandel SJ, Orloff LA, Randolph GW, Steward DL, American Thyroid Association Surgical Affairs Committee Writing Task Force (2015) American Thyroid Association statement on preoperative imaging for thyroid cancer surgery. Thyroid 25(1):3–14. https://doi.org/10.1089/thy.2014.0096
Acknowledgements
We would like to thank all doctors, nurses, technicians, and patients involved in their dedication to the study.
Funding
This article was funded by National Natural Science Foundation of Xiamen, China (Grant no. 3502Z20227336).
Author information
Authors and Affiliations
Contributions
PH, LH, and FZ designed the study. XS and FX designed the clinical questionnaire. TL, LW, and JZ collated the data. PH and XL performed statistical data analyses. JZ and PH contributed to drafting the manuscript. PH and LH contributed equally to this work. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, P., Han, L., Shi, X. et al. Predictive value of the single most suspicious ultrasound feature in subcentimeter thyroid nodules: a retrospective observational cohort study. J Cancer Res Clin Oncol 150, 384 (2024). https://doi.org/10.1007/s00432-024-05895-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00432-024-05895-z