
Abstract
Purpose
Statin treatment has been shown in certain population studies and meta-analyses to improve survival of patients with pancreatic ductal adenocarcinoma (PDAC). This study assessed if patients with statin treatment had better overall survival (OS) and disease-free survival (DFS) after upfront pancreatoduodenectomy for PDAC.
Methods
Consecutive PDAC patients were retrospectively collected from three centers in Europe and USA (study period: 2000–2017). Adult patients who underwent upfront pancreatoduodenectomy and survived the first 90 postoperative days were included. Patients with metastasis at diagnosis or with macroscopic incomplete resection were excluded. Patients were considered under statin if started at least one month before pancreatoduodenectomy. Survival rates were calculated using Kaplan–Meier method and compared with log-rank test.
Results
A total of 496 patients were included. Median age was 67 years (IQR 59–75), 48% (n = 236) were women, and 141 patients (28%) received statin treatment already preoperatively. Patients with and without statin treatment were comparable in terms of demographics and pre-/intraoperative characteristics, except for age and pre-existing diabetes. Median OS and DFS were similar in patients with and without statin treatment (OS: 29, 95% CI 22–36 vs. 27 months, 95% CI 22–32, p = 0.370, DFS: 18, 95% CI 14–22 vs. 16 months, 95% CI 14–18, p = 0.430). On multivariable Cox regression, lymph node involvement (HR 1.9, 95% CI 1.6–2.2, p < 0.001), tumor differentiation (HR 1.3, 95% CI 1.1–1.6, p = 0.003), and postoperative chemotherapy (HR 0.5, 95% CI 0.4–0.7, p < 0.001) were predictors of OS, whereas statin treatment was not a prognostic factor (HR 0.9, 95% CI 0.7–1.2, p = 0.376).
Conclusion
In this international cohort of PDAC patients, statin treatment did not influence survival after upfront pancreatoduodenectomy. Nodal involvement, tumor differentiation, and postoperative chemotherapy were independent predictors of OS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is the most common form of pancreatic cancer, one of the most lethal cancers with a 5-year survival rate of less than 10% (Fristrup et al. 2016). Radical surgical resection represents the backbone of any curative approach. However, surgical interventions, such as pancreatoduodenectomy (PD) are complex and its associated postoperative morbidity is still high. Despite recent advances in surgical techniques and perioperative care, the long-term outcomes for patients with pancreatic cancer remain dismal (Conroy et al. 2018). There is a need to find novel approaches that could improve survival rates by reducing early cancer recurrence.
Statins are nowadays widely used drugs to lower serum cholesterol levels and to reduce the risk of cardiovascular disease by a direct inhibition of the enzyme HMG (hydroxymethylglutaryl)-CoA-reductase. Recently, there has been growing interest in the potential anti-tumor effects of statins (Yuan et al. 2022). Several preclinical and clinical studies have suggested that statins may inhibit the growth and dissemination of pancreatic cancer cells (Tamburrino et al. 2020). However, the impact of statin use on long-term outcomes in patients undergoing PD for pancreatic cancer is not well established.
The aim of this cross-sectional study was to evaluate whether preoperative statin use is associated with improved long-term survival and reduced cancer recurrence in patients undergoing upfront PD for ductal adenocarcinoma of the pancreatic head.
Methods
Patients
Inclusion criteria were patients > 18 years old and who underwent upfront PD for ductal adenocarcinoma proven on histopathology from January 2000 to December 2017. Exclusion criteria were absence of consent to research, macroscopic incomplete resection (R2 resection), perioperative death within 90 postoperative days, or metastasis at time of diagnosis. Patients with neoadjuvant treatment were not considered.
Patients were issued from 3 international tertiary and referral centers: Edouard-Herriot Hospital (Lyon, France), Carolinas Medical Center (Charlotte, USA), and Lausanne University Hospital CHUV (Lausanne, Switzerland). Postoperative complications were defined according to the Clavien classification (Dindo et al. 2004), and the Comprehensive Complication Index (CCI) was calculated (Slankamenac et al. 2013). Delayed gastric emptying, pancreatic fistula, and hemorrhage were based on the International Study Group for Pancreatic Surgery definitions (Bassi et al. 2005; Wente et al. 2007a, b). Surgical-site infection was defined according to the Centers for Disease Control and Prevention (Horan et al. 1992).
Objectives and endpoints
The main objective was to compare the survival rates of patients with versus without statin treatment. The primary endpoint was the overall survival in months (OS).
Secondary objectives were to evaluate if patients with statin treatment presented less recurrence. Secondary endpoints were disease-free survival (DFS) and recurrence rate.
Statin treatment
Patients were considered under a preoperative statin treatment if the statin intake was started at least one month before PD. Only statin treatments were considered. Other anti-lipid drugs such as fibrates were not taken into account. All subclasses of statin were included.
Statistics
Continuous data were summarized using median and interquartile range (IQR), and categorical data were summarized with number and percentage. Mann–Whitney U tests were used to compare parametric continuous data, while chi-square tests were performed for categorical data. Survival curves (OS and DFS) were calculated using Kaplan-Maier method and compared with the log-rank test. Median follow-up was calculated using the inverse Kaplan-Maier method. Predictive factors of survival were calculated using uni- and multivariable Cox regression analyses. Continuous variables were dichotomized for the Cox regression analyses: age (> 60 vs. ≤ 60), body-mass index (> 25 kg/m2 vs. ≤ 25 kg/m2), American Society of Anesthesiologists score (I/II vs. III/IV), tumor size (T1-2 vs. T3-4), and CA19-9 (> 42 U/ml vs. ≤ 42 U/ml)(Shimagaki et al. 2023). Only factors with p < 0.1 on univariable analysis were included in the multivariable analysis. A two-tailed p-value < 0.05 was considered significant. SPSS© 28.0 Statistics for Mac was used for all statistical analyses (IBM Corp., Armonk, NY, USA).
Results
Patients
A total of 496 patients were included with a median age of 67 years (IQR 59–75). Forty-eight percent of the patients (236/496) were women. The overall morbidity rate was 64% (319/496) and the median CCI was 8.7 (IQR 0–27.6). Median OS and DFS were 27 months (95% CI 23–31) and 17 months (95% CI 15–19), respectively.
There were 141 patients (28%) who had a preoperative statin treatment. Preoperative characteristics, pathological results, and surgical details of patients are summarized in Table 1. Patients with and without preoperative statin treatment presented similar characteristics and intraoperative details, except for age and the incidence of pre-existing diabetes mellitus that were higher in the statin group. Postoperative outcomes of both groups are displayed in Table 2. No difference was found in terms of morbidity and length of hospital stay between both groups.
Survival and recurrence
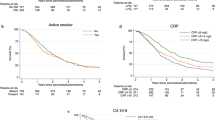
Median OS of patients with statin treatment was 29 months (95% CI 22–36) and 27 months (95% CI 22–32) for patients without preoperative statin treatment (p = 0.370). Median DFS were similar in the groups with and without statin treatment (18 months, 95% CI 14–22 vs. 16 months, 95% CI 14–18, p = 0.430). Kaplan–Meier curves comparing OS and DFS of patients with and without statin treatment are shown in Fig. 1 and Fig. 2. No gender-related median difference of OS between patients with and without statin treatment was found, respectively (women: 34 months, 95% CI 21–47 vs. 30 months, 95% CI 23–37, p = 0.406 and men: 26 months, 95% CI 17–35 vs. 24 months, 95% CI 19–29, p = 0.578). Within a median follow-up of 50 months (95% CI 45–55), the recurrence rates were 75/141 (53%) in the statin group and 200/355 (56%) in the group without statin treatment (p = 0.525). In the statin and non-statin groups, 75% (105/141) and 78% (277/355) of patients received postoperative chemotherapy, respectively (p = 0.395).

Kaplan–Meier curves of overall survival (OS) of patient with and without preoperative statin treatment (median OS: statin, 29 months, 95% CI 22–36 vs. no statin, 27 months, 95% CI 22–32, p = 0.370)

Kaplan–Meier curves of disease-free survival (DFS) of patient with and without preoperative statin treatment (median DFS: statin, 18 months, 95% CI 14–22 vs. no statin, 16 months, 95% CI 14–18, p = 0.430)
Prognostic factors of survival
On univariable Cox regression, preoperative statin treatment was not found as a predictor of OS (HR 0.9, 95% CI 0.7–1.2, p = 0.376). On multivariable analysis, lymph node involvement (HR 1.9, 95% CI 1.6–2.2, p < 0.001), tumor differentiation (HR 1.3, 95% CI 1.1–1.6, p = 0.003), and postoperative chemotherapy (HR 0.5, 95% CI 0.4–0.7, p < 0.001) were identified as prognostic factors of OS. Table 3 summarizes the uni- and multivariable analyses for predictors of OS.
Discussion
The present study assessing the impact of perioperative statin treatment on the long-term outcomes after surgery for PDAC did not find a difference in OS and DFS in this cohort. Independent predictors of OS were lymph node involvement, tumor differentiation, and adjuvant chemotherapy.
It has been hypothesized that statin had anti-cancer properties. Via the inhibition of HMG-CoA-reductase, statins block the transformation of HMG-CoA to geranyl-pyrophosphate and farnesyl-pyrophosphate (Di Bello et al. 2020). This blockage has an effect on decreasing not only cholesterol, but also inflammation, tissue remodeling, angiogenesis, and cell proliferation, as well as inducing apoptosis (Di Bello et al. 2020). The latter effects explain the potential anti-cancer properties of statins. Some studies have shown that patients with statin treatment had better survival in several types of solid cancers. Meta-analyses confirmed these findings for example in gastric and colorectal cancers (Cai et al. 2015; Yuan et al. 2022). In pancreas cancer, a 2019 systematic review and meta-analysis of 27 studies showed that statin users had a reduced risk of developing PDAC compared to patients without statin treatment (OR 0.70, 95% CI 0.60–0.82, p < 0.0001)(Archibugi et al. 2019). Moreover, a recent Norwegian study based on a nationwide registry found that patients under statin medication (n = 621) had better OS than non-statin users (n = 1993, HR: 0.87, 95% CI 76–97) (Støer et al. 2021). A 2018 meta-analysis found similar results with an improved survival in pancreatic cancer patients under statin treatment (HR: 0.75, 95% CI 0.59–0.90) (Jian-Yu et al. 2018). Significant heterogeneity between included studies was noticed. A 2020 meta-analysis even found that the positive effect on survival was more important among surgically resected pancreatic cancer patients (HR 0.5, 95% CI 0.32–0.76) (Tamburrino et al. 2020). It is important to bear in mind that observational studies might have selection and immortal-time biases, so the preceding findings need to be interpreted cautiously. A large study using the SEER-Medicare database (n = 17,372) and the inverse-probability weighting method to eliminate immortal-time bias showed that statin treatment initiated within 6 months after cancer diagnosis did not improve 3-year OS (Emilsson et al. 2018).
The present study assessed survival in patients who have been operated on, which is different from most of the observational studies on statins in cancer, where only non-operated patients are included, or a heterogeneous cohort of operated and non-operated patients is evaluated. In the studied specific cohort of PDAC patients operated upfront, it is interesting to hypothesize why no survival difference was found. First, it corroborates other studies on operated and non operated PDAC patients suggesting that statin treatment has no effect on long-term survival. For instance, a similar cross-sectional study by Tamburrino et al. including 430 patients who underwent pancreatic resection showed that DFS and disease-specific survival (DSS) were not influenced by a statin treatment (median DSS: statin, 37 vs. no statin, 34 months, p = 0.878)(Tamburrino et al. 2021). Of note, in the previously cited study, not all patients underwent pancreatoduodenectomy (69%) and 39% of the patients had neoadjuvant chemotherapy, which is different from the present study. The high rate of adjuvant chemotherapy after PDAC resection in this cohort (77%) might be another explanation, as adjuvant chemotherapy has been shown to improve OS of pancreatic cancer patients, such as in the present cohort. Other potential hypotheses are that the treatment duration and the therapeutic adherence to the statin treatment are important determinants. Unfortunately, these details were not available in this cohort. A final hypothesis pertains to the type of statin treatment. A meta-analysis by Tamburrino et al. found that rosuvastatin was associated with better outcomes in pancreas cancer patients, on the contrary of other statin types (Tamburrino et al. 2020). The present study included different statin subtypes without restriction.
In the present cohort, only patients who were operated upfront were included. The reason for not including patients who underwent neoadjuvant chemotherapy and for including only patients with PDAC of the pancreatic head was to have a cohort as homogeneous as possible. If such patients were included, it would have been necessary to take into account this supplementary element in the multivariable analysis or perform a subgroup analysis. Moreover, as neoadjuvant treatment was only recently implemented in the centers included in this study and various chemotherapy regimens were used, the number of patients with neoadjuvant would have been relatively small compared to the rest of the cohort and the heterogeneity more important.
Some limitations of this study should be mentioned. Data on the subtype of statin treatment (e.g., atorvastatine, simvastatine, others) were not available. Furthermore, the duration of the statin treatment was not known at time of data analysis. It was only known if patients had the statin treatment for more than a month prior to surgery. Another potential important information is the compliance to the statin treatment that was not available in the chart review. The retrospective design of the study has inherent limitations, such as errors during collection data or missing data.
This exploratory study suggests that using statin as an anti-cancer treatment for PDAC patients might not be useful in patients who undergo upfront surgery. Results might be different in a population of PDAC patients who benefit from neoadjuvant chemotherapy or in a patient cohort of borderline or locally advanced PDAC. This would be interesting to evaluate in future cohort or cross-sectional studies if statins impact survival in these subtypes of pancreatic cancer patients. Moreover, results of this study cannot be generalized to overall cancer patients, in particular patients who did not have surgery as upfront oncological treatment.
In summary, this international multicentric cross-sectional study did not identify preoperative statin treatment as a prognostic factor of survival in patients who underwent upfront surgery for PDAC. Factors predictive of OS were related to the biology of the tumor and adjuvant chemotherapy.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Archibugi L, Arcidiacono PG, Capurso G (2019) Statin use is associated to a reduced risk of pancreatic cancer: a meta-analysis. Dig Liver Dis 51:28–37. https://doi.org/10.1016/j.dld.2018.09.007
Bassi C, Dervenis C, Butturini G et al (2005) Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 138:8–13. https://doi.org/10.1016/j.surg.2005.05.001
Cai H, Zhang G, Wang Z et al (2015) Relationship between the use of statins and patient survival in colorectal cancer: a systematic review and meta-analysis. PLoS ONE 10:e0126944. https://doi.org/10.1371/journal.pone.0126944
Conroy T, Hammel P, Hebbar M et al (2018) FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med 379:2395–2406. https://doi.org/10.1056/NEJMoa1809775
Di Bello E, Zwergel C, Mai A, Valente S (2020) The innovative potential of statins in cancer: new targets for new therapies. Front Chem 8:516. https://doi.org/10.3389/fchem.2020.00516
Dindo D, Demartines N, Clavien P-A (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Emilsson L, García-Albéniz X, Logan RW et al (2018) Examining bias in studies of statin treatment and survival in patients with cancer. JAMA Oncol 4:63–70. https://doi.org/10.1001/jamaoncol.2017.2752
Fristrup C, Detlefsen S, Hansen CP, Ladekarl M (2016) Danish Pancreatic Cancer Database. Clin Epidemiol 8:645–648. https://doi.org/10.2147/CLEP.S99471
Horan TC, Gaynes RP, Martone WJ et al (1992) CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol 13:606–608
Jian-Yu E, Graber JM, Lu S-E et al (2018) Effect of metformin and statin use on survival in pancreatic cancer patients: a systematic literature review and meta-analysis. Curr Med Chem 25:2595–2607. https://doi.org/10.2174/0929867324666170412145232
Shimagaki T, Sugimachi K, Mano Y et al (2023) A new scoring system with simple preoperative parameters as predictors of early recurrence of pancreatic ductal adenocarcinoma. PLoS ONE 18:e0288033
Slankamenac K, Graf R, Barkun J et al (2013) The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann Surg 258:1–7. https://doi.org/10.1097/SLA.0b013e318296c732
Støer NC, Bouche G, Pantziarka P et al (2021) Use of non-cancer drugs and survival among patients with pancreatic adenocarcinoma: a nationwide registry-based study in Norway. Acta Oncol 60:1146–1153. https://doi.org/10.1080/0284186X.2021.1953136
Tamburrino D, Crippa S, Partelli S et al (2020) Statin use improves survival in patients with pancreatic ductal adenocarcinoma: a meta-analysis. Dig Liver Dis 52:392–399. https://doi.org/10.1016/j.dld.2020.01.008
Tamburrino D, Guarneri G, Pagnanelli M et al (2021) Chemopreventive agents after pancreatic resection for ductal adenocarcinoma: legend or scientific evidence? Ann Surg Oncol 28:2312–2322. https://doi.org/10.1245/s10434-020-09097-y
Wente MN, Bassi C, Dervenis C et al (2007a) Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 142:761–768. https://doi.org/10.1016/j.surg.2007.05.005
Wente MN, Veit JA, Bassi C et al (2007b) Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 142:20–25. https://doi.org/10.1016/j.surg.2007.02.001
Yuan M, Han S, Jia Y et al (2022) Statins are associated with improved survival of patients with gastric cancer: a systematic review and meta-analysis. Int J Clin Pract 2022:4938539. https://doi.org/10.1155/2022/4938539
Funding
Open access funding provided by University of Lausanne. The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
Conception/Design: GRJ, MS. Data acquisition: GRJ, SGF, IL, DV, JP. Analysis/Interpretation: all authors. Drafting of the manuscript: GRJ, MS. Critical revision: all authors. Final approval of the manuscript to be published: all authors. Agreement to be accountable for all aspects of the work: all authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Vaud Ethics Committee (CER-VD, 18.06.2019, n°2017–01169).
Consent to participate
Informed consent was obtained from all individuals included in the study.
Consent to publish
Patients signed informed consent regarding publishing their data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Joliat, GR., Gaspar-Figueiredo, S., Labgaa, I. et al. Impact of preoperative statin medication on long-term outcomes after pancreatoduodenectomy for ductal adenocarcinoma: an international multicentric cross-sectional study. J Cancer Res Clin Oncol 149, 17007–17014 (2023). https://doi.org/10.1007/s00432-023-05426-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-023-05426-2