
Abstract
Background
Many cancer patients suffer from problems concerning nutrition and physical activity (PA) during and after their treatment. Forwarding reliable health information could help to alleviate severe symptoms. The present study aimed to examine cancer patients’ commonly used information sources on nutrition and PA.
Methods
An anonymous questionnaire was developed and distributed to German cancer patients in different settings. In total, 90 questionnaires have been completed between October 2021 and March 2022. For analysis, descriptive statistics were used and associations between information sources and patients’ lifestyle behaviour explored utilising Spearman’s Rho, Mann–Whitney U, and Pearson’s Chi Square tests.
Results
The cancer patients received information on nutrition and PA most frequently from physicians (70.9%), family and friends (68%) and browsing the internet (61.3%). Half of the patients (51.1%) had questions concerning these topics during the time of their disease. The majority of those patients (81.8%) reported that their questions were answered. The topics were addressed primarily with outpatient oncologists (60.0%) and in rehabilitation clinics (53.3%). Just about half of the patients (55.3%) felt satisfactorily informed on nutrition and PA in their cancer disease, more so if they talked to their oncologist or family physician (Z = − 2.450, p = 0.014 and Z = − 3.425, p = 0.001 resp.).
Conclusion
Cancer patients receive information on nutrition and PA predominantly after their initial treatment. Since they might be missing significant information to alleviate severe symptoms during their treatment, the importance of nutrition and PA should be emphasised by clinicians early on in treatment.
Trial registration
Trial Registration Number (May 7, 2021): 2021-2149-Bef.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
A cancer diagnosis sets many cancer patients off on an arduous journey. Managing their disease, treatment, and daily live is a straining endeavour that can leave patients overwhelmed and helpless. Additionally, their information needs are extensive and ever-changing over the course of their treatment (Rutten et al. 2005). Recurring topics during and post-treatment are nutrition and physical activity (PA). In some respects, both lifestyle topics are intertwined with one another. For example, they share similar molecular mechanisms preventing cancer development and progress, contribute to weight gain or loss, and are modifiable by the patients themselves (Wiseman 2019). Furthermore, patients who are physically more active also tend to adhere to a healthier diet, strengthening their association in practice (Grosso et al. 2017; Schlesinger et al. 2014). In cancer patients, nutrition and PA can be negatively affected by both the disease and its treatments. Malnutrition is reported to occur in up to 80% of cancer patients, leading to adverse consequences such as poor survival, functional status, and reduced quality of life (QoL) (Capuano et al. 2010; Datema et al. 2011; Jager-Wittenaar et al. 2011; Lim et al. 2012; Montoya et al. 2010; Mouri et al. 2018; Norman et al. 2010; Pressoir et al. 2010; Wie et al. 2010). Additionally, more than fifty percent of cancer patients report symptoms impacting their nutrition and PA, e.g., early satiety, dysphagia, xerostomia, nausea, vomiting, exercise intolerance, dyspnoea, and fatigue (Deftereos et al. 2021; Maddocks 2020; Trajkovic-Vidakovic et al. 2012). On the other hand, nutrition and PA are modifiable by the patients and in turn allow them to more actively alleviate severe symptoms and side effects and ameliorate their prognosis (Arends et al. 2017; Avancini et al. 2020; Brown et al. 2009, 2012; Bye et al. 2020; Cormie et al. 2017; Edvardsen et al. 2015; Hilfiker et al. 2018; Lee et al. 2016; Maddocks 2020; McTiernan et al. 2019; Montagnese et al. 2020; Mouri et al. 2018; Sarwer et al. 2009; Scott and Tharmalingam 2019; Uster et al. 2018). By providing health information on such topics, patients can be empowered to raise their self-care management skills and engage more actively in shared decision-making (Jung 2014).
In the spirit of patient-centred care, it is desirable to provide patient information that is tailored to their needs to improve healthcare quality (Institute of Medicine (US) Commitee on Quality of Health Care in America 2001). To forward reliable information, it is important to understand where patients receive information from, and whether they are satisfied with the information acquired. Assessing which sources of information cancer patients utilise can help to identify sources with potentially harmful health information. For example, recommendation of one-sided diets as can be found on the internet can lead to malnutrition, harming the patient (Huebner et al. 2014; Suarez-Lledo and Alvarez-Galvez 2021). On the other hand, understanding which sources are preferably utilised by cancer patients, they can be referred specifically to information sources containing reliable information. Previous studies have assessed information needs and sources for cancer patients, but data focussing on information sources with respect to nutrition and PA are lacking (Clarke et al. 2016; Johnston et al. 2021; Lewis et al. 2012; Moldovan-Johnson et al. 2014; Rutten et al. 2005). We aimed at closing this knowledge gap by surveying which information channels on nutrition and PA cancer patients use. Since nutrition and PA are interrelated and often covered in parallel, e.g., in guidelines, booklets, and interventional studies, we examined information sources of both topics simultaneously (Bye et al. 2020; Manneh-Vangramberen 2018; Rock et al. 2022). Furthermore, we wanted to assess with whom they talked about nutrition and PA ever since their cancer diagnosis. Finally, we wanted to assess their self-reported satisfaction regarding their coverage with information.
Participants and methods
Questionnaire
We chose to conduct a cross-sectional questionnaire study. A pilot questionnaire was developed in collaboration with physicians, cancer patients, and statisticians. The pilot version was tested for length and comprehension among three cancer patients with different types of cancer. The final questionnaire consisted of 45 questions divided into seven sections in four main categories:
-
Demographic data including the cancer diagnosis and time since the diagnosis.
-
Assessment of the patient’s lifestyle behaviour (nutrition and PA) and self-efficacy.
-
Information sources on nutrition and PA utilised by cancer patients.
-
Questions, contact persons (i.e., with whom they talked about nutrition and PA; e.g., physicians, other healthcare practitioners, family and friends), and self-reported satisfaction regarding information on nutrition and PA.
We primarily used closed questions with lists of possible answers in form of Likert scales. Semi-open questions offered the participants space to add and elaborate answers. We utilised the sections Diet and Exercise of the validated Simple Lifestyle Indicator Questionnaire (SLIQ) by Godwin et al. to assess the patients’ dietary and physical lifestyle behaviour (Godwin et al. 2013). The patients’ self-efficacy was assessed using the validated Short Scale for Measuring General Self-Efficacy Beliefs (ASKU) by Beierlein and colleagues (Beierlein et al. 2012). The CROSS guidelines were utilised to report on the findings (Sharma et al. 2021).
Patients
Adult German-speaking patients with a cancer diagnosis were eligible to participate. The questionnaire was passed on to a convenience sample of three hospitals (20 questionnaires), four rehabilitation clinics (110 questionnaires), two oncological (40 questionnaires) and two general practices (30 questionnaires) predominantly located in the Federal States of North Rhine-Westphalia and Thuringia, Germany, between October 2021 and March 2022. The participants had the option to complete the survey online, accessible via Soscisurvey over the same period. Participation was voluntarily and anonymous.
Ethical vote
This study was approved by the Ethics Commission of the University Hospital of Jena (Reg.-Nr. 2021-2149-Bef). All participants gave their consent before enrolling in the study.
Data preparation and analysis
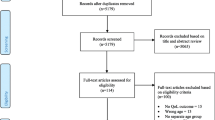
Out of 200 print versions sent, 90 completed questionnaires were returned (response rate 45%). Additionally, 17 questionnaires have been answered online. Answer forms with more than 25% missing data or missing the type of cancer have been excluded. In total, 90 questionnaires were included in the analysis. Data was collected and analysed using IBM SPSS Statistics 27. During analysis, missing values were excluded listwise.
The analysis focussed on the following main items:
-
Information sources: How often do you utilise media (e.g., print media, television, internet-websites) or persons (e.g., physicians, family and friends) to inform yourself on nutrition and physical activity?
-
Contact persons: Did you talk to someone about nutrition and physical activity regarding your cancer treatment and follow-up care? If so, who did you talk to? When were these topics addressed? How did you feel when these topics have been addressed?
-
Information coverage: How satisfied are you with the information you received which covered nutrition and physical activity during and after your cancer treatment?
We explored whether associations between these items emerged, which could indicate diverse preferences among patient-subgroups. Additionally, we gathered data on demographics, dietary behaviour, physical activity, and patients’ self-efficacy, and assessed associations with either of the main items. To analyse correlations between at least ordinal-scaled items, Spearman’s Rho (effect size ρ) was calculated. Mann–Whitney U tests were performed to analyse differences in central tendencies between two groups and significances tested asymptotically (Z: standardised score, effect size r =|Z| /√n). Associations between nominal variables were analysed utilising Pearson’s Chi Square (X2) tests (df: degrees of freedom, Cramér’s V: effect size). Effect sizes of correlations and associations were estimated to be small (0.1), medium (0.3) or large (0.5) according to Cohen (Cohen 1988). For all analyses, p values smaller than 0.05 were considered significant.
Results
Sample
In total, 90 questionnaires have been completed and analysed. Female and male cancer patients participated equally (51.1% or 48.9%), their ages ranging from 18 to 90 years (mean value 58.55 ± 15.74 years, median 60.5 years). The most prevalent types of cancer were leukaemia and lymphomas (23.3%), followed by breast (21.1%) and lung cancer (15.6%). The demographic data are shown in Table 1.
Lifestyle behaviour and self-efficacy
The dietary behaviour as reported by the cancer patients is depicted in Fig. 1, while their self-reported PA is subject to Fig. 2. As suggested by the SLIQ, higher consumption of salat, fruit, and high-fibre cereal, as well as higher physical activity indicated a healthier lifestyle (Godwin et al. 2013). Sixty-one percent (61.1%, n = 55) of the respondents did not report changes in their dietary behaviour as compared to the time before their cancer disease. Twenty-nine percent (28.9, n = 26) consumed aforementioned foods more often, and 10.0% (n = 9) less often.

Dietary behaviour of cancer patients as indicated by healthy food-consumption (n = 86)

Physical Activity (at least 30 min at a time) of cancer patients (n = 80)
Utilising the ASKU to score cancer patients’ self-efficacy beliefs ranging from 1 (lowest self-efficacy belief) to 5 (highest self-efficacy belief), on average the cancer patients scored 3.84 (± 0.83, median 4, n = 87) (Beierlein et al. 2012).
Information sources on nutrition and physical activity
Cancer patients reported to receive information on nutrition and PA more frequently by physicians, family and friends or through media. Browsing the internet was reported to be the most common medial information source on these topics. Social media, however, was hardly ever utilised. Figure 3 contains the patients’ responses.

Information sources on nutrition and PA utilised by cancer patients
Significant correlations between demographics and information sources are presented in Table 2. There was a negative association between the patient’s age and importance of information from internet (ρ = − 0.375, p = 0.001) and social media (ρ = − 0.546, p < 0.001). Patients receiving health information through social media also reported a healthier diet (ρ = 0.310, p = 0.011). The frequency of receiving information from print media was associated with information from television (ρ = 0.611, p < 0.001). Receiving information from family and friends correlated positively with a healthier lifestyle, i.e., a healthier diet and higher PA (ρ = 0.362, p = 0.004).
Patient questions and their contact persons
Half of the patients (51.1%, n = 45) reported having questions on nutrition and PA with respect to the cancer disease. Most (81.8%, n = 36) reported that these questions had been answered, mainly by physicians, dietitians, and sometimes through media like the internet and books.
Seventy-one percent (71.4%, n = 60) talked with someone on nutrition and PA. Their contact persons are listed in Fig. 4. The topics were addressed most frequently in an outpatient clinic by an oncologist or during a stay at a rehabilitation clinic, rather less during a stay in a hospital (see Fig. 5). Twenty percent (20.3%, n = 12) felt relieved when nutrition and PA were addressed, whereas 11.9% (n = 7) felt rather tense.

Reference persons of cancer patients concerning nutrition and PA (cases n = 60, multiple answers possible). *Separate question with cases n = 88

Time and place nutrition and PA have been addressed (cases n = 60, multiple answers possible)
A significant association was found between the institution the patient received the questionnaire from, and whom they talked to on nutrition and PA (X2 = 9.930, df = 4, 0.042). Men talked significantly more to oncologists than women (Z = − 1.996, r = 0.258, p = 0.046) whereas women and younger patients talked more often with family and friends (Z = − 2.740, r = 0.354, p = 0.006 and Z = − 2.306, r = 0.303, p = 0.021 resp.).
Self-reported satisfaction with information coverage
More than half of the patients (55.3%, n = 47) felt satisfactorily informed on nutrition and PA regarding their cancer disease, whereas 16.5% (n = 14) did not feel sufficiently informed.
Patients reported to feel more satisfied with information on nutrition and PA when receiving them from oncologists or family physicians (oncologists: Z = − 2.450, r = 0.325, p = 0.014; family physicians: Z = − 3.425, r = 0.378, p = 0.001). In contrast, no associations occurred for other persons and information sources.
Discussion
Complementary to studies assessing cancer patients’ information needs and sources, to our knowledge this is the first study focussing on their information sources addressing nutrition and PA since the time of modern communication techniques (Chua et al. 2021; Finney Rutten et al. 2016; Hoh et al. 2018; Rutten et al. 2005; Wieldraaijer et al. 2019). The results indicate that patients commonly have questions concerning nutrition and PA in context of their cancer disease. They usually receive information on these topics from physicians, family and friends, and the internet.
Information sources
The cancer patients reported that they received information on the topics nutrition and PA more often by physicians than by media. This corresponds to the findings of Rutten et al. in their systematic review from 2005 regarding information sources of cancer patients (Rutten et al. 2005). Since then, the internet has become more readily available and is utilised more often (Chua et al. 2021). However, healthcare practitioners remain the preferred source of information among cancer patients (Adjei Boakye et al. 2018; Chua et al. 2021; Finney Rutten et al. 2016). In our sample, browsing the internet was the premier medial source of information, and a medium negative correlation with the patient’s age has been found. This association has been observed in other studies as well and could be explained by a higher familiarity of younger patients with the internet (Adjei Boakye et al. 2018; Soto-Perez-de-Celis et al. 2018). A large negative association with the patient’s age emerged concerning social media as source of information, while a large positive correlation between browsing the internet and social media formed. These correlations reflect the fact that younger patients use social media, which is part of the internet, more frequently (Auxier and Anderson 2021). All in all, cancer patients rarely acquired health information via social media channels. Contrary to other studies, no association between information sources and demographic factors other than age were found in our patient sample (Finney Rutten et al. 2016; Kelly et al. 2010; Soto-Perez-de-Celis et al. 2018).
The importance of family and friends as psychosocial support for cancer patients to cope is well established (Lee et al. 2018; Luszczynska et al. 2013; Newton et al. 2021; Rose 1990; Ruiz-Rodríguez et al. 2021). Our study adds an informational role to these contact persons as patients reported to receive information on nutrition and PA from them more often than by media. Interestingly, receiving information from family and friends was correlated positively with a healthier lifestyle regarding nutrition and PA. This finding is in line with data showing higher fruit and vegetable consumption among cancer patients who seek health information from family and friends (Lewis et al. 2012). Support by family and friends furthermore encourages exercise (Lee et al. 2018). They take an active role in the patient’s treatment as they establish the environment in which the patient recovers. Improving lifestyle habits within the patient’s environment would make it easier for the patient to adopt beneficial lifestyle modifications. Thus, family and friends should be included when conveying information to cancer patients.
Contact persons and information coverage
Half of the cancer patients had questions concerning nutrition and PA regarding their disease, and the majority was answered by healthcare providers. The most common contact persons were oncologists and physicians in rehabilitation clinics, while these topics were rarely brought up visiting their family physician. Information related to rehabilitation such as nutrition and PA are more prevalent post-treatment than during diagnosis and treatment (Rutten et al. 2005). However, they are highly important during cancer therapy as well as many cancer patients experience severe side effects caused by cancer and its treatments (Hébuterne et al. 2014). Many side effects are amendable to PA and nutritional lifestyle modifications, such as cachexia and malnutrition, nausea and vomiting, loss of endurance and loss of power, resulting in improved outcomes and QoL (Arends et al. 2017; Avancini et al. 2020; Brown et al. 2012, 2009; Bye et al. 2020; Cormie et al. 2017; Edvardsen et al. 2015; Hilfiker et al. 2018; Laviano et al. 2018; Lee et al. 2016; Maddocks, 2020; McTiernan et al. 2019; Montagnese et al. 2020; Mouri et al. 2018; Sarwer et al. 2009; Scott and Tharmalingam 2019; Uster et al. 2018). If patients don’t get to know the importance of nutrition and PA, they may be left satisfied because they don’t know what beneficial information they are missing out on. To improve this point, nutrition and PA should become an integral part of cancer diagnosis and treatment. Structured treatment programmes are needed to reliably implement counselling on nutrition and PA in cancer patients and putting advice into practice.
Cancer patients who talked about these topics to their oncologist or family physician expressed significantly higher satisfactions with information received. Whereas they spend time in rehabilitation clinics only temporarily, regular consultations with their oncologist and family physician allow to build trust that is required to improve adherence to a healthy lifestyle and leave the patient satisfied (Baker et al. 2003; Chen et al. 2020; Hendren and Kumagai 2019). While many actors should be part of lifestyle education, one approach is to integrate these physicians in structured treatment programmes to emphasize the opportunities nutrition and PA present.
Limitations
A higher participation of institutions interested in conveying information on nutrition and PA may have recruited patients who are better informed and more satisfied than the general cancer population. Since most questionnaires were returned from patients in rehabilitation clinics and oncological practices, a recency effect could have biased some items. For example, asking to whom the patients talked to, contact persons other than rehabilitation physicians and oncologists might be underrepresented as they recall their last contact person easier than previous ones.
For the sources of information or reasons for dissatisfaction on these lifestyle topics, we did not differentiate between nutrition and PA, to avoid making the questionnaire too long. We cannot exclude that there are differences between both but have reason to believe that the results are representative since the two topics are interrelated. To provide an overview of information sources utilised by cancer patients, we assessed different types of sources. Since we did not ask for specific sources such as certain websites or books, we cannot assess whether the patients received reliable information. Moreover, we did not ascertain whether the patients put their gathered information into practice.
This study does hardly capture the information sources of patients with advanced cancer, but rather of cancer survivors, resulting in a survivorship bias. Furthermore, we acquired a relatively small number of participants. Therefore, especially sub-items generated very small sample sizes and, at best, produced tendencies. This might compromise generalisability. Finally, socially desired answers cannot be excluded.
Future research should aim to acquire a larger sample size. A longitudinal approach could improve understanding the associations between receiving information from different information sources and changes in cancer patients’ lifestyle behaviour. Information sources should be specified (e.g., which websites cancer patients utilise) and their credibility should be ascertained.
Conclusion
The transfer of information on nutrition and PA in cancer patients primarily takes place post-treatment, where they receive post-treatment lifestyle advice. This can be problematic as many patients experience nutritional and physical issues already during cancer therapy. Just about half of them are content with the information they received, but they are still potentially missing important information to alleviate severe symptoms by exercise and dietary means. Not receiving this information from healthcare practitioners might entice patients to search for information online, which yields potentially harmful advice. Hence, it is meaningful to forward reliable information as early as possible by credible sources. Clinicians and family physicians should be involved as early in the treatment process as possible. This could be realised as part of structured treatment programmes to emphasize the opportunities nutrition and PA present in cancer treatment. Finally, family and friends should receive the same information to create a favourable environment for the patient to adapt beneficial lifestyle modifications.
Data availability
Data available on request from the authors. The data that support the findings of this study are available on request from the corresponding author, S. J. Boesenecker, upon reasonable request.
References
Adjei Boakye E, Mohammed KA, Geneus CJ, Tobo BB, Wirth LS, Yang L, Osazuwa-Peters N (2018) Correlates of health information seeking between adults diagnosed with and without cancer. PLoS ONE 13(5):e0196446. https://doi.org/10.1371/journal.pone.0196446
Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, Fearon K, Hütterer E, Isenring E, Kaasa S, Krznaric Z, Laird B, Larsson M, Laviano A, Mühlebach S, Muscaritoli M, Oldervoll L, Ravasco P, Solheim T et al (2017) ESPEN guidelines on nutrition in cancer patients. Clin Nutr 36(1):11–48. https://doi.org/10.1016/j.clnu.2016.07.015
Auxier B, Anderson M (2021) Social Media Use in 2021. https://www.pewresearch.org/internet/2021/04/07/social-media-use-in-2021/#:~:text=Some%2084%25%20of%20adults%20ages,45%25)%20report%20doing%20this
Avancini A, Sartori G, Gkountakos A, Casali M, Trestini I, Tregnago D, Bria E, Jones LW, Milella M, Lanza M, Pilotto S (2020) Physical activity and exercise in lung cancer care: will promises be fulfilled? Oncologist 25(3):e555–e569. https://doi.org/10.1634/theoncologist.2019-0463
Baker R, Mainous Iii AG, Gray DP, Love MM (2003) Exploration of the relationship between continuity, trust in regular doctors and patient satisfaction with consultations with family doctors. Scand J Prim Health Care 21(1):27–32. https://doi.org/10.1080/0283430310000528
Beierlein C, Kovaleva A, Kemper CJ, Rammstedt B (2012) Ein Messinstrument zur Erfassung subjektiver Kompetenzerwartungen: Allgemeine Selbstwirksamkeit Kurzskala (ASKU) [Short Scale for Measuring General Self-efficacy Beliefs (ASKU)] (Vol. 2012/17). GESIS - Leibniz-Institut für Sozialwissenschaften. https://nbn-resolving.org/urn:nbn:de:0168-ssoar-292351
Brown T, Avenell A, Edmunds LD, Moore H, Whittaker V, Avery L, Summerbell C (2009) Systematic review of long-term lifestyle interventions to prevent weight gain and morbidity in adults. Obes Rev 10(6):627–638. https://doi.org/10.1111/j.1467-789X.2009.00641.x
Brown JC, Winters-Stone K, Lee A, Schmitz KH (2012) Cancer, physical activity, and exercise. Compr Physiol 2(4):2775–2809. https://doi.org/10.1002/cphy.c120005
Bye A, Sandmael JA, Stene GB, Thorsen L, Balstad TR, Solheim TS, Pripp AH, Oldervoll LM (2020) Exercise and nutrition interventions in patients with head and neck cancer during curative treatment: a systematic review and meta-analysis. Nutrients 12(11):3233. https://doi.org/10.3390/nu12113233
Capuano G, Gentile PC, Bianciardi F, Tosti M, Palladino A, Di Palma M (2010) Prevalence and influence of malnutrition on quality of life and performance status in patients with locally advanced head and neck cancer before treatment. Support Care Cancer 18(4):433–437. https://doi.org/10.1007/s00520-009-0681-8
Chen W, Feng Y, Fang J, Wu J, Huang X, Wang X, Wu J, Zhang M (2020) Effect of trust in primary care physicians on patient satisfaction: a cross-sectional study among patients with hypertension in rural China. BMC Fam Pract 21(1):196. https://doi.org/10.1186/s12875-020-01268-w
Chua GP, Ng QS, Tan HK, Ong WS (2021) Cancer survivors: what are their information seeking behaviours? J Cancer Educ 36(6):1237–1247. https://doi.org/10.1007/s13187-020-01756-8
Clarke MA, Moore JL, Steege LM, Koopman RJ, Belden JL, Canfield SM, Meadows SE, Elliott SG, Kim MS (2016) Health information needs, sources, and barriers of primary care patients to achieve patient-centered care: a literature review. Health Informatics J 22(4):992–1016. https://doi.org/10.1177/1460458215602939
Cohen J (1988) Statistical Power Analysis for the Behavioral Sciences. L. Erlbaum Associates. https://books.google.de/books?id=gA04ngAACAAJ
Cormie P, Zopf EM, Zhang X, Schmitz KH (2017) The impact of exercise on cancer mortality, recurrence, and treatment-related adverse effects. Epidemiol Rev 39(1):71–92. https://doi.org/10.1093/epirev/mxx007
Datema FR, Ferrier MB, Baatenburg de Jong RJ (2011) Impact of severe malnutrition on short-term mortality and overall survival in head and neck cancer. Oral Oncol 47(9):910–914. https://doi.org/10.1016/j.oraloncology.2011.06.510
Deftereos I, Yeung JMC, Arslan J, Carter VM, Isenring E, Kiss N, On Behalf Of The Nourish Point Prevalence Study, G (2021) Assessment of nutritional status and nutrition impact symptoms in patients undergoing resection for upper gastrointestinal cancer: results from the multi-centre NOURISH point prevalence study. Nutrients 13(10):3349. https://doi.org/10.3390/nu13103349
Edvardsen E, Skjønsberg OH, Holme I, Nordsletten L, Borchsenius F, Anderssen SA (2015) High-intensity training following lung cancer surgery: a randomised controlled trial. Thorax 70(3):244–250. https://doi.org/10.1136/thoraxjnl-2014-205944
Finney Rutten LJ, Agunwamba AA, Wilson P, Chawla N, Vieux S, Blanch-Hartigan D, Arora NK, Blake K, Hesse BW (2016) Cancer-related information seeking among cancer survivors: trends over a decade (2003–2013). J Cancer Educ 31(2):348–357. https://doi.org/10.1007/s13187-015-0802-7
Godwin M, Pike A, Bethune C, Kirby A, Pike A (2013) Concurrent and convergent validity of the simple lifestyle indicator questionnaire. ISRN Family Med 2013:529645. https://doi.org/10.5402/2013/529645
Grosso G, Bella F, Godos J, Sciacca S, Del Rio D, Ray S, Galvano F, Giovannucci EL (2017) Possible role of diet in cancer: systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr Rev 75(6):405–419. https://doi.org/10.1093/nutrit/nux012
Hébuterne X, Lemarié E, Michallet M, de Montreuil CB, Schneider SM, Goldwasser F (2014) Prevalence of malnutrition and current use of nutrition support in patients with cancer. JPEN J Parenter Enteral Nutr 38(2):196–204. https://doi.org/10.1177/0148607113502674
Hendren EM, Kumagai AK (2019) A matter of trust. Acad Med 94(9):1270–1272. https://doi.org/10.1097/acm.0000000000002846
Hilfiker R, Meichtry A, Eicher M, Nilsson Balfe L, Knols RH, Verra ML, Taeymans J (2018) Exercise and other non-pharmaceutical interventions for cancer-related fatigue in patients during or after cancer treatment: a systematic review incorporating an indirect-comparisons meta-analysis. Br J Sports Med 52(10):651–658. https://doi.org/10.1136/bjsports-2016-096422
Hoh JC, Schmidt T, Hubner J (2018) Physical activity among cancer survivors-what is their perception and experience? Support Care Cancer 26(5):1471–1478. https://doi.org/10.1007/s00520-017-3977-0
Huebner J, Marienfeld S, Abbenhardt C, Ulrich C, Muenstedt K, Micke O, Muecke R, Loeser C (2014) Counseling patients on cancer diets: a review of the literature and recommendations for clinical practice. Anticancer Res 34(1):39–48. https://ar.iiarjournals.org/content/anticanres/34/1/39.full.pdf
Institute of Medicine (US) Commitee on Quality of Health Care in America. (2001) Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK222274/pdf/Bookshelf_NBK222274.pdf
Jager-Wittenaar H, Dijkstra PU, Vissink A, van der Laan BF, van Oort RP, Roodenburg JL (2011) Malnutrition and quality of life in patients treated for oral or oropharyngeal cancer. Head Neck 33(4):490–496. https://doi.org/10.1002/hed.21473
Johnston EA, van der Pols JC, Ekberg S (2021) Needs, preferences, and experiences of adult cancer survivors in accessing dietary information post-treatment: a scoping review. Eur J Cancer Care 30(2):e13381. https://doi.org/10.1111/ecc.13381
Jung M (2014) Determinants of health information-seeking behavior: implications for post-treatment cancer patients. Asian Pac J Cancer Prev 15(16):6499–6504. https://doi.org/10.7314/apjcp.2014.15.16.6499
Kelly B, Hornik R, Romantan A, Schwartz JS, Armstrong K, DeMichele A, Fishbein M, Gray S, Hull S, Kim A, Nagler R, Niederdeppe J, Ramirez AS, Smith-McLallen A, Wong N (2010) Cancer information scanning and seeking in the general population. J Health Commun 15(7):734–753. https://doi.org/10.1080/10810730.2010.514029
Laviano A, Di Lazzaro L, Koverech A (2018) Nutrition support and clinical outcome in advanced cancer patients. Proc Nutr Soc 77(4):388–393. https://doi.org/10.1017/s0029665118000459
Lee JLC, Leong LP, Lim SL (2016) Nutrition intervention approaches to reduce malnutrition in oncology patients: a systematic review. Support Care Cancer 24(1):469–480. https://doi.org/10.1007/s00520-015-2958-4
Lee MK, Park SY, Choi GS (2018) Association of support from family and friends with self-leadership for making long-term lifestyle changes in patients with colorectal cancer. Eur J Cancer Care 27(3):e12846. https://doi.org/10.1111/ecc.12846
Lewis N, Martinez LS, Freres DR, Schwartz JS, Armstrong K, Gray SW, Fraze T, Nagler RH, Bourgoin A, Hornik RC (2012) Seeking cancer-related information from media and family/friends increases fruit and vegetable consumption among cancer patients. Health Commun 27(4):380–388. https://doi.org/10.1080/10410236.2011.586990
Lim SL, Ong KC, Chan YH, Loke WC, Ferguson M, Daniels L (2012) Malnutrition and its impact on cost of hospitalization, length of stay, readmission and 3-year mortality. Clin Nutr 31(3):345–350. https://doi.org/10.1016/j.clnu.2011.11.001
Luszczynska A, Pawlowska I, Cieslak R, Knoll N, Scholz U (2013) Social support and quality of life among lung cancer patients: a systematic review. Psychooncology 22(10):2160–2168. https://doi.org/10.1002/pon.3218
Maddocks M (2020) Physical activity and exercise training in cancer patients. Clin Nutr ESPEN 40:1–6. https://doi.org/10.1016/j.clnesp.2020.09.027
Manneh-Vangramberen I (2018) Living well during cancer treatment. In: The European Cancer Patient Coalition (Ed.). Belgium
McTiernan A, Friedenreich CM, Katzmarzyk PT, Powell KE, Macko R, Buchner D, Pescatello LS, Bloodgood B, Tennant B, Vaux-Bjerke A, George SM, Troiano RP, Piercy KL (2019) Physical activity in cancer prevention and survival: a systematic review. Med Sci Sports Exerc 51(6):1252–1261. https://doi.org/10.1249/mss.0000000000001937
Moldovan-Johnson M, Martinez L, Lewis N, Freres D, Hornik RC (2014) The role of patient-clinician information engagement and information seeking from nonmedical channels in fruit and vegetable intake among cancer patients. J Health Commun 19(12):1359–1376. https://doi.org/10.1080/10810730.2014.906521
Montagnese C, Porciello G, Vitale S, Palumbo E, Crispo A, Grimaldi M, Calabrese I, Pica R, Prete M, Falzone L, Libra M, Cubisino S, Poletto L, Martinuzzo V, Coluccia S, Esindi N, Nocerino F, Minopoli A, Grilli B et al (2020) Quality of life in women diagnosed with breast cancer after a 12-month treatment of lifestyle modifications. Nutrients 13(1):136. https://doi.org/10.3390/nu13010136
Montoya JE, Domingo F Jr, Luna CA, Berroya RM, Catli CA, Ginete JK, Sanchez OS, Juat NJ, Tiangco BJ, Jamias JD (2010) Nutritional status of cancer patients admitted for chemotherapy at the National Kidney and Transplant Institute. Singapore Med J 51(11):860–864
Mouri T, Naito T, Morikawa A, Tatematsu N, Miura S, Okayama T, Omae K, Takayama K (2018) Promotion of behavioral change and the impact on quality of life in elderly patients with advanced cancer: a physical activity intervention of the multimodal nutrition and exercise treatment for advanced cancer program. Asia Pac J Oncol Nurs 5(4):383–390. https://doi.org/10.4103/apjon.apjon_21_18
Newton JC, O’Connor M, Saunders C, Moorin R, Ali S, Nowak AK, Halkett GKB (2021) The role of psychosocial support in the experiences of people living with advanced cancer: a qualitative exploration of patients’ perspectives. Psychooncology 30(3):287–295. https://doi.org/10.1002/pon.5569
Norman K, Stobäus N, Smoliner C, Zocher D, Scheufele R, Valentini L, Lochs H, Pirlich M (2010) Determinants of hand grip strength, knee extension strength and functional status in cancer patients. Clin Nutr 29(5):586–591. https://doi.org/10.1016/j.clnu.2010.02.007
Pressoir M, Desné S, Berchery D, Rossignol G, Poiree B, Meslier M, Traversier S, Vittot M, Simon M, Gekiere JP, Meuric J, Serot F, Falewee MN, Rodrigues I, Senesse P, Vasson MP, Chelle F, Maget B, Antoun S, Bachmann P (2010) Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br J Cancer 102(6):966–971. https://doi.org/10.1038/sj.bjc.6605578
Rock CL, Thomson CA, Sullivan KR, Howe CL, Kushi LH, Caan BJ, Neuhouser ML, Bandera EV, Wang Y, Robien K, Basen-Engquist KM, Brown JC, Courneya KS, Crane TE, Garcia DO, Grant BL, Hamilton KK, Hartman SJ, Kenfield SA et al (2022) American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J Clin 72(3):230–262. https://doi.org/10.3322/caac.21719
Rose JH (1990) Social support and cancer: adult patients’ desire for support from family, friends, and health professionals. Am J Community Psychol 18(3):439–464. https://doi.org/10.1007/bf00938117
Ruiz-Rodríguez I, Hombrados-Mendieta I, Melguizo-Garín A, Martos-Méndez MJ (2021) The association of sources of support, types of support and satisfaction with support received on perceived stress and quality of life of cancer patients. Integr Cancer Ther 20:1534735421994905. https://doi.org/10.1177/1534735421994905
Rutten LJ, Arora NK, Bakos AD, Aziz N, Rowland J (2005) Information needs and sources of information among cancer patients: a systematic review of research (1980–2003). Patient Educ Couns 57(3):250–261. https://doi.org/10.1016/j.pec.2004.06.006
Sarwer DB, von Sydow Green A, Vetter ML, Wadden TA (2009) Behavior therapy for obesity: where are we now? Curr Opin Endocrinol Diabetes Obes 16(5):347–352. https://doi.org/10.1097/MED.0b013e32832f5a79
Schlesinger S, Walter J, Hampe J, von Schönfels W, Hinz S, Küchler T, Jacobs G, Schafmayer C, Nöthlings U (2014) Lifestyle factors and health-related quality of life in colorectal cancer survivors. Cancer Causes Control 25(1):99–110. https://doi.org/10.1007/s10552-013-0313-y
Scott BR, Tharmalingam S (2019) The LNT model for cancer induction is not supported by radiobiological data. Chem Biol Interact 301:34–53. https://doi.org/10.1016/j.cbi.2019.01.013
Sharma A, Minh Duc NT, Luu Lam Thang T, Nam NH, Ng SJ, Abbas KS, Huy NT, Marušić A, Paul CL, Kwok J, Karbwang J, de Waure C, Drummond FJ, Kizawa Y, Taal E, Vermeulen J, Lee GHM, Gyedu A, To KG et al (2021) A consensus-based checklist for reporting of survey studies (CROSS). J Gen Intern Med 36(10):3179–3187. https://doi.org/10.1007/s11606-021-06737-1
Soto-Perez-de-Celis E, Perez-Montessoro V, Rojo-Castillo P, Chavarri-Guerra Y (2018) Health-related information-seeking behaviors and preferences among mexican patients with cancer. J Cancer Educ 33(3):505–509. https://doi.org/10.1007/s13187-018-1334-8
Suarez-Lledo V, Alvarez-Galvez J (2021) Prevalence of health misinformation on social media: systematic review. J Med Internet Res 23(1):e17187. https://doi.org/10.2196/17187
Trajkovic-Vidakovic M, de Graeff A, Voest EE, Teunissen SC (2012) Symptoms tell it all: a systematic review of the value of symptom assessment to predict survival in advanced cancer patients. Crit Rev Oncol Hematol 84(1):130–148. https://doi.org/10.1016/j.critrevonc.2012.02.011
Uster A, Ruehlin M, Mey S, Gisi D, Knols R, Imoberdorf R, Pless M, Ballmer PE (2018) Effects of nutrition and physical exercise intervention in palliative cancer patients: a randomized controlled trial. Clin Nutr 37(4):1202–1209. https://doi.org/10.1016/j.clnu.2017.05.027
Wie GA, Cho YA, Kim SY, Kim SM, Bae JM, Joung H (2010) Prevalence and risk factors of malnutrition among cancer patients according to tumor location and stage in the National Cancer Center in Korea. Nutrition 26(3):263–268. https://doi.org/10.1016/j.nut.2009.04.013
Wieldraaijer T, Duineveld LAM, Bemelman WA, van Weert H, Wind J (2019) Information needs and information seeking behaviour of patients during follow-up of colorectal cancer in the Netherlands. J Cancer Surviv 13(4):603–610. https://doi.org/10.1007/s11764-019-00779-5
Wiseman MJ (2019) Nutrition and cancer: prevention and survival. Br J Nutr 122(5):481–487. https://doi.org/10.1017/S0007114518002222
Acknowledgements
We thank all patients for their time and patience to complete the questionnaires. Thank you to all physicians who distributed the questionnaires. Many thanks to the statisticians and everyone who contributed to construct the questionnaire.
Funding
Open Access funding enabled and organized by Projekt DEAL. No funding.
Author information
Authors and Affiliations
Contributions
SJB and JH conceived of the presented idea. SJB designed the questionnaires in cooperation with JH. SJB analysed the survey data with support from JH. SJB wrote the manuscript with support from JH, VM and JB. JH supervised the project. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Boesenecker, S.J., Mathies, V., Buentzel, J. et al. Nutrition and physical activity in cancer patients: a survey on their information sources. J Cancer Res Clin Oncol 149, 3823–3833 (2023). https://doi.org/10.1007/s00432-022-04282-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-022-04282-w