
Abstract
Purpose
Oral mucositis is a common, painful side effect of cancer treatment—be it locoregional (e.g. irradiation) or systemic (e. g. chemotherapy). Phytotherapy is often used by patients to alleviate symptoms. However, knowledge on which medical plants are recommended by literature about Traditional European Medicine (TEM), their effect(s) on symptoms and their efficacy is severely lacking. Therefore, we developed a novel approach to assess traditional knowledge of herbals used in TEM and searched the online databases for studies reporting effects of these plants.
Methods
At first, online research did not yield a satisfying number of studies (MESH terms: “mucositis” OR “stomatitis” AND “herbal” OR “herbal medicine”). Trials were labelled by the country conducting the study. In parallel, we compiled a list of 78 plants recommended for treating oral mucositis by screening 14 books on TEM. Then, a “hit list” of the plants most often mentioned was composed and used further for a second online investigation using the Latin plant designations as MESH term. Studies of both online searches were pooled for analysis.
Results
There is a gap between traditional knowledge and trials investigating medical plants used by TEM. Overall, herbal remedies alleviate oral mucositis and especially, gingivitis well. There is good evidence for using Matricaria recutita L., Salvia officinalis L., Calendula officinalis L. and Thymus spp. L. for treating oral mucositis.
Conclusion
Clinical trials investigating medical plants known in TEM are rare. However, following our research strategy, we could extrapolate four plants with good evidence for alleviating symptoms of oral mucositis and gingivitis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Oral mucositis is a common, painful side effect of cancer treatment—be it locoregional (e.g. irradiation) or systemic (e. g. chemotherapy, EGFR-inhibitors). The symptom describes the inflammation of the enoral mucosa and is -if induced by radiotherapy-often associated with xerostomia, dysgeusia or dental problems (Rubenstein et al. 2004; Barrach et al. 2015; Kato et al. 2017; Crowder et al. 2018). Patients may present with erythematous or atrophic lesions of the oral mucosa and in more severe cases with ulcers. Especially, the latter is often accompanied with pain and an increase of risk for mucosal bleeding, infections and a higher hospitalization rate (Rubenstein et al. 2004).
The rate of patients using complementary alternative medicine (CAM) in addition to the therapy regime or to alleviate side effects of cancer treatment ranges from 40 to 90% (Molassiotis et al. 2005; Micke et al. 2009; Huebner et al. 2014; Wortmann et al. 2016). However, only around 50% of these patients inform their general practitioner and 35%, their treating oncologist about using CAM. Herbal medicine is one of the most commonly used CAM therapies, yet health practitioners seem to play a minor role in providing information. Patients usually use family, friends and media as main source of information (Molassiotis et al. 2005; Huebner et al. 2014).
Herbal medicine has a long history as medical plants and were mainly used in primary care up to the eighteenth century. The knowledge of most herbs dates back to antiquity recorded by the works of Hippocrates of Kos, Galen and Dioscorides (Leonti and Verpoorte 2017). In Europe, herbal medicinal products fall under the European Medicines Agency (EMA) Guideline on Quality of Herbal Medicinal Products (EMA/CPMP/QWP/2819/00). There are three different market authorizations a company selling herbals may apply for. While the first category comprises phytopharmacological agents for which pharmaceutical quality, safety and efficacy have to be demonstrated by preclinical and clinical studies, the other categories include (I) a well-established medical use of a plant or (II) a herb in use for more than 30 years (and more than 15 years in Europe) (Fürst and Zündorf 2015). In opposite to the traditional phytopharmacy practised in Europe till the beginning of the nineteenth century, rational phytopharmacy bases on the premise that a rational phytopharmaceutical has a proven effect. The phytopharmaceutical is composed of substances responsible for the actual effect and substances that may modify stability or bioavailability (Schulz and Hänsel 2013).
There is no clear-cut definition describing TEM. According to a survey amongst experts, the following traditional branches or methods (mostly based on the antique medical traditions) are usually counted as part of TEM: ancient Greek medicine (Hippocrates of Kos: dietetics, res non naturales; Galen: humourism, nosology), medieval (monastic) medicine (Hildegard of Bingen) or naturopathic methods deviated from ancient Greek medicine during the nineteenth century. TEM does (usually) not include homeopathy and approaches which fall into the more esoteric category (e. g. demonology, astrology, alchemy and magic) (Uehleke 2007; Micke and Büntzel 2013).
As mentioned above, patients commonly use CAM additionally to standard treatment and herbals play a major role (Molassiotis et al. 2005; Wortmann et al. 2016). Several plants like Matricaria recutita L., Althaea officinalis L., Malva sylvestris L. or Calendula officinalis are known to TEM for treating oral mucositis (Büntzel et al. 2019). However, the German guideline of supportive care in oncology does only mention the first, Matricaria recutita L., citing an insufficient level of evidence due to the lack of clinical trials (or low evidence) or due to studies not really launched to German oncology practitioners (Leitlinienprogramm Onkologie|S3-Leitlinie Supportive Therapie 2017). This astonishing discrepancy between plants reported by TEM (Büntzel et al. 2019) and the obvious lack of information available in the national guidelines is alarming—considering our patients’ use of herbal remedies (Molassiotis et al. 2005). This argues against treating herbal remedies as the red-headed stepchild of supportive cancer care and for (re)assessing which plants are commonly recommended by TEM and for investigating whether these are backed up by clinical trials.
Here we show a novel approach that may help to bridge the gap between TEM and the lack of evidence described above. We chose the oral mucositis as this is a common, easily assessed side effect of (systemic) oncological treatment.
Methods
Systematic literature research
Selection of databases: we selected PubMed as medical open access database and AGRICOLA as broader open scientific database. Furthermore, we tried to include CAM-specific data pools. The database of the University of Witten-Herdecke (“CAM-base”) yielded zero hits for oral mucositis. The last update was in 2010. The Veronica-Carstens-Stiftung offers additional data pool. Unfortunately, this database focusses on homeopathy alone.
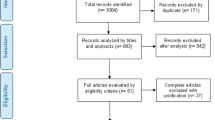
We performed a systematic literature research using the online databases PubMed (174 hits) on 17th of February 2019 and AGRICOLA (83 hits, 4th of October 2019) to assess studies investigating herbal remedies for treating oral mucositis. The following MESH terms were used: “mucositis” OR “stomatitis” AND “herbal” OR “herbal medicine”. Articles were screened for studies using medical plants (historically) known to TEM. We applied no language restrictions or filters to the search, however only abstracts written in English were included into the final screening of literature. Abstracts identified by literature search were independently screened by two investigators (Ju. B. and J. B.). Abstracts were screened for the following inclusion criteria: (I) phytopharmacon is (historically) known to TEM; (II) used in clinical trials; (III) information available in English. Reference lists of the articles meeting the inclusion criteria were then screened via hand search to identify additional studies (34 hits). In summary, we were able to identify 33 studies suitable for further analysis (Fig. 1, Table 1). These were assessed for (I) plants reported for treating oral mucositis and (II) the country performing the research.

PRISMA flow diagram, first systematic literature research. Qualitative synthesis: Studies included investigating a plant for treating oral mucositis and describing an effect. Quantitative synthesis: Studies measuring or recording the effect, e.g., bleeding score gingivitis, and statistically comparing control/standard of care with the intervention group
A second literature research was performed using 14 German books (listed in Table 2) on traditional medical plants and herbal remedies to assess, which plants were reported for treating mucositis/gingivitis or pharyngitis. We included books addressing different groups of interest: specialists (specialist literature, four books), laymen (popular science, five books) and users of wild growing edible or medical plants (plant identification books, five books). If a plant was reported to alleviate oral symptoms, we recorded it as known herbal remedy (Table 3). A resulting “hit list” of medical plants was generated by recording every report per plant and book screened. Each plant mentioned ≥ 6 times was included into a final “hit list” of the most common plants (Table 3).
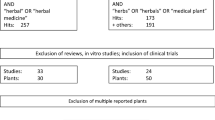
We used these for a second systematic literature research on PubMed on the 10th March 2019 and on AGRICOLA on the 4th of October 2019. Latin designations of plants were used as MESH terms. We performed literature research separately for each plant. Reviews and in vitro or animal studies were excluded. Then, abstracts of clinical trials were screened for studies investigating “pain”, “inflammation” or “infection”. In a third step, we finally extracted studies focusing on “mucositis”, “stomatitis”, “gingivitis”, “periodontitis” or “pharyngitis” (for research strategy also refer to Fig. 2). Subsequently, we merged studies reporting clinical trials for plants of our “hit list” from our first research on PubMed and AGRICOLA with studies of our second systematic literature research. After removing duplicates we identified 24 clinical trials for further analysis (listed in Table 4). In summary, we developed a five step strategy to assess literature:
-
1.
Initial use of online databases focusing on the symptom and plants chosen by the investigators for treatment.
-
2.
Assessment of plants recommended by TEM literature referring to a balanced mixture of specialists’ and laymen’s literature. This step tries to represent, what plants have the highest probability to be used by our patients as the plants of our “hit list” are the ones which are most often recommended.
-
3.
Merging the two first steps under the premise that the plants found in step (2) are the most commonly used and known plants for treating mucositis in Germany. Studies investigating these plants are included into further analysis.
-
4.
Using Latin designations of plants of the “hit list” of step (2) as MESH terms on PubMed and AGRICOLA; manual screening and filtering for clinical trials investigating the symptom “oral mucositis”.
-
5.
Studies extracted under (3) and (4) are now used for further analysis.

Synopsis, PRISMA flow diagram, second systematic literature research. Qualitative synthesis: Studies included investigating a plant for treating oral mucositis and describing an effect. Quantitative synthesis: Studies measuring or recording the effect, e.g. bleeding score gingivitis, and statistically comparing control/standard of care with the intervention group
A graphic overview of all steps of our research strategy is presented in Fig. 3.

Overview over search strategy used for identifying plants and relevant studies included
Qualitative analysis
The quality of studies that were later on included into semi-quantitative analysis, was assessed as following: The evidence level of the clinical trials included was evaluated according to the Oxford criteria (Oxford Centre for Evidence-based Medicine 2009). Trial quality was assessed according to the Jadad-Score. This validated score ranges from zero (very poor quality) to five (high quality) (Jadad et al. 1996, 2000).
Assessment of the effect of medical plants on symptoms of oral mucositis
Studies extracted were sorted by symptoms as followed: mucositis/stomatitis, gingivitis/periodontitis and pharyngitis. Studies investigated the effect of “medical plant vs. placebo/ control remedy/baseline”. The p value describes the probability of error of the existing effect. We extracted p values for each medical plant compared to the control remedy. Afterwards, we used a simplified p value score for semi-quantitative analysis to describe the effect of herbal medicine on alleviating symptoms. The (p value based) score is shown in Table 5.
Figures and illustrations
The free software “Inkscape” and/or Microsoft Office Powerpoint were used for generating all figures presented.
Results
Few studies investigate medical plants recommended for treating oral mucositis by TEM
The first search yielded 33 studies (Table 1). Here, Matricaria recutita L. and Zingiber officinale ROSCOE were the most investigated plants (nine studies each), followed by Glycyrrhiza glabra L. and Punica granatum L. (four studies). In summary, we compiled a list 17 different plants known to TEM reported by studies of our first systematic literature research. Next, we sorted studies according to the country performing the clinical trial. Astonishingly, only a small minority of studies (9.1%) was initiated in Europe. The majority (33.3%) was conducted in Iran. Japanese studies were mainly added, as these did also reported clinical trials on ginger—a plant already mentioned in the “De Materia Medica” of Dioscorides [first century AD, (Dioscorides and Berendes 2019)].
To get an overview about TEM remedies, we conducted our second search using books on herbal remedies. Out of 14 books, we were able to list 78 herbs. Subsequently, we compiled a “hit list” of 18 plants that were recommended ≥ 6 times (Table 3, Fig. 4). Out of all plants Matricaria recutita L. (mentioned 13 times), Salvia officinalis et sclarea L. (mentioned 12 times), Althaea officinalis L. and Malva sylvestris L. et neglecta WALLER (mentioned 11 times) were the most often recommended medicinal herbs.

Hit-list of plants, overview over the 18 most commonly recommended herbal remedies. 100% = plant is mentioned in every herbal medicine book screened
Afterwards, the overall list of plants found in our second literature research (books) was compared with plants found during our first systematic literature review. Finally, we found an overlap of 12 plants, meaning out of the 78 plants recommended by TEM only 15.3% of these were investigated by clinical trials. Furthermore, we found only clinical evidence for three medical plants out of the 18 herbal remedies of our “hit list” of most commonly recommended medical herbs.
In summary, we have an enormous gap/imbalance between medical plants recommended by TEM and clinical trials investigating these.
To overcome this imbalance we have performed a second online search as described above.
Search results and characteristics of included studies
24 studies published between 1996 and 2018 meeting the inclusion criteria were included into the following analysis (Table 4). The number of patients participating in these clinical trials ranged from 14 to 286, we could include a total of 1725 patients. Out of all studies included four were controlled clinical trials, ten randomized clinical trials (RCT) and ten placebo randomized controlled trials, a total of 13 studies was blinded. The majority of studies had a high level of evidence (17/24 evidence level IB, refer to Table 4). 50.0% of studies were conducted in an oncological context (chemotherapy, radiotherapy or radio-chemotherapy). Studies investigated a total of 17 plants; out of these, seven herbs were part of our “hit list”. However, three herbs of the remaining plants investigated were mentioned by traditional TEM (Aloe L.: 1 hit; Zingiber officinalis ROSCOE: 1 hit; Commiphora myrrha NES.: 6 hits, refer also to Table 3).
Results of semi-quantitative analysis on the overall impact of medical plants on treating oral mucositis
22 of the 24 studies listed statistically compared the investigated plant with a control group and were thus included into semi-quantitative analysis (score). Seven studies found no difference between the effects of plants used versus the control. However, eight studies were positive and seven even highly positive for the effect of the plant investigated. Of the seven studies not being positive for herbal medicine, three studies compared the herbal remedy used to placebo, and four studies to conventional treatment (eg. chlorhexidine mouth wash (Cabrera-Jaime et al. 2018)) or ice cube (Dos Reis et al. 2016). In summary, there is evidence for using herbal remedies to alleviate oral mucositis (Fig. 5).

Semi-quantitative analysis on the overall impact of medical plants on treating oral mucositis using the semi-quantitative scoring system. A score ≥ 1 signifies a probability of error of < 5%. A score < 1 shows that no significant effect exists
Results of semi-quantitative analysis of the impact of medical plants on treating oral mucositis and stomatitis
16 studies investigated the impact of herbal medicine on mucositis (oral cavity) and stomatitis. However, only 14 quantified their results and were consequently used for semi-quantitative analysis. Six studies reported no difference between the plant investigated and control. It should be noted, that three of these studies compared the effect of the medical plant to standard of care/other remedies (Saller et al. 2001; Steinmann et al. 2012; Dos Reis et al. 2016). Notably three studies were highly positive for the medical plant investigated, while four showed a (weaker) positive effect (Fig. 6a). Taking all studies in account, we calculated an average score of 0.86. Conclusively, we found positive evidence for using medical plants. In following sub-analysis (Fig. 6b), we investigated studies also recording the effect on pain experienced during treatment of oral mucositis. Six out of seven studies reported that the herbal remedy investigated alleviated pain. Only Cabrera-Jaime et al. testing Plantago major L. for effects reported a negative outcome. The three studies reporting for a highly positive effect of the plant investigated compared Matricaria recutita L. against placebo. Other plants investigated were: Aloe vera L., Calendula officinalis L. and Mentha × piperita L. The overall score for alleviating pain was 1.29. Hence, we conclude that herbal medicine is quite effective for treating pain.

Impact of medical plants on treating oral mucositis and stomatitis, a semi-quantitative analysis of the effect on mucositis/stomatitis, b relieving pain, c pharyngitis and d gingivitis/periodontitis; semi-quantitative scoring system. A score ≥ 1 signifies a probability of error of < 5%. A score < 1 shows that no significant effect exists
Results of semi-quantitative analysis on the impact of medical plants on treating pharyngitis
Only two studies investigated medical plants, mainly Salvia officinalis L., for treating pharyngitis. One reported a positive outcome (Hubbert et al. 2006) while the other (Schapowal et al. 2009) described no difference to the control (Fig. 6c). However, the latter—Schapowal et al.—compared Salvia officinalis L. and Echinacea MOENCH to chlorhexidine/lidocaine spray, concluding that the combination of Salvia officinalis L. and Echinacea MOENCH was as effective as the standard of care. Taking this into account, we conclude that Salvia officinalis L. may be an effective alternative treatment to standard care.
Results of semi-quantitative analysis on the impact of medical plants on treating gingivitis and periodontitis
Seven studies investigated the effect of medical plants on gingivitis or periodontitis, six were included for semi-quantitative analysis. All reported a positive or even strongly positive effect of the plant(s) used (Fig. 6d). Studies used bleeding on probing and/or gingival index and/or plaque index for assessing the symptom. The following plants were investigated: Calendula officinalis L., Cymbopogon flexuosus NEES EX STEUD., Eucalyptus L’HER, Matricaria recutita L., Commiphora myrrha (NEES) ENGL., Polygonum aviculare L., Rosmarinus officinalis L., Salvia officinalis L., Thymus zygs L., Vaccinium myrtillus L. and Zingiber officnale ROSCOE. The overall core was 1.5, indicating good evidence for treating gingivitis or periodontitis with herbal remedies mentioned above.
Results of sub-group analyses for the evidence of single plants for treating oral mucositis
Seven plants included in this analysis were mentioned at least twice by different studies. Hence, we initiated a sub-group analysis to investigate their (individual) impact on treating mucositis. Plants and corresponding studies are listed in Table 4. Eleven studies investigated the effect of Matricaria recutita L.; three studies did not report any difference between the plant’s effect compared to placebo or control. However, Matricaria recutita L. was superior to placebo or control in the other eight studies included; the overall score for chamomile was 1.2 (Fig. 7a). Conclusively, treatment with chamomile seems to be a valuable and effective measure against oral mucositis. Out of these eleven studies, seven studies investigated the effect of Matricaria recutita L. alone without being combined with another medical plant. We used these for sub-group analysis. Here chamomile had an overall p value score of 1.1 (Fig. 8), indicating the plant is indeed effective. All studies had an evidence level IB and show a consistent, favourable effect of Matricaria recutita L., resulting in a Grade A recommendation, Oxford Criteria (Oxford Centre for Evidence-based Medicine 2009).

Impact of medical plants on treating oral mucositis, a semi-quantitative analysis of Matricaria recutita L., bSalvia officinalis L., cCalendula officinalis L. and dThymus spp. L.; semi-quantitative scoring system. A score ≥ 1 signifies a probability of error of < 5%. A score < 1 shows that no significant effect exists

Impact of Matricaria recutita L. on treating oral mucositis, semi-quantitative analysis of studies only using chamomile; semi-quantitative scoring system. A score ≥ 1 signifies a probability of error of < 5%. A score < 1 shows that no significant effect exists
Salvia officinalis L. was investigated by six studies of which three did not report a difference between control and herbal remedy. Yet, the studies of Steinmann et al., Schapowal et al. and Saller et al. compared Salvia officinalis to Traumeel S, chlorhexidine/lidocaine and acyclovir respectively. All authors described Salvia officinalis as effective as the drug tested against. It should be taken into consideration that Saller et al. reported that a mixture of Salvia officinalis L. and Rheum L. was more effective than the application of Salvia officinalis L. alone (Saller et al. 2001). In summary, despite a lower score of 0.8 (Fig. 7b), we found evidence for using Salvia officinalis L. to treat oral mucositis. Due to George et al. being only a level IIB study and using a combination of herbs, we extrapolated data and were only able to give a Grade C recommendation, Oxford Criteria (Oxford Centre for Evidence-based Medicine 2009)).
Calendula officinalis L. was investigated by three studies; all used the plant in combination with other medical herbs. Marucci et al. did not detect any difference in grade III mucositis when testing Calendula officinalis against placebo. However, Mahyari et al. and Bardellini et al. reported a positive effect on gingivitis and stomatitis respectively. The overall score was 1.0 (Fig. 7c). There is some evidence for using Calendula officinalis L. (Grade B recommendation, Oxford Criteria]) for treating oral mucositis, but the small number of studies included should be taken into account.
We summarized studies investigating thyme under Thymus spp. L. as trials used two different sub-species of thyme (Thymus vulgaris L., Thymus zygis L.). All studies showed a positive effect of the plant, two were even highly positive (p value < 0.01). Studies were compared against controls. The overall score was 1.7 (Fig. 7d). Despite the small study number, we found good evidence for using Thymus spp. L. for treating oral mucositis as all studies consistently demonstrated the favourable effect of this herbal remedy, Grade B recommendation, Oxford Criteria (Oxford Centre for Evidence-based Medicine 2009).
Aloe vera L., Mentha × piperita L. and Rosmarinus officinalis L. were investigated in combination with other plants by two studies each showing scores of 0.5, 1.5 and 1.5 respectively. Due to the small study number, we hesitate to judge the role these plants might play for treating oral mucositis. Plants investigated by ≤ 2 trials are also listed in Table 6.
Discussion
Oral mucositis is a common side effect of cancer treatment (Rubenstein et al. 2004; Barrach et al. 2015). More than half of our patients use CAM additionally to standard of care and here herbals play a major role (Molassiotis et al. 2005; Huebner et al. 2014). 39% of head neck cancer patients are searching for complimentary approaches. 25% of those are using medical herbs (Büntzel et al. 2018). However, information on the type and evidence of medical plants used by our patients is rare. Yet, popular science books on TEM regularly (and rightly) advise the user to ask the treating physician for advice [for example (Malm and Möbus 2018)]. This poses a problem -where to look at for reliable data? Our first online research revealed a total of 33 studies investigating the effect of medical plants on oral mucositis. Taken together, we did not get an abundant amount of studies; furthermore, the plants most often investigated (with the exception of Matricaria recutita L.)—Zingiber officinale (ginger) ROSCOE, Glycyrrhiza glabra L. (liquorice) and Punica granatum L. (pomegranate)—might not represent the herbals typically used or recommended in Germany. However, the composition of this list of plants is not that astonishing, considering that out of these 33 studies only three were initiated in Europe. Most of these trials were conducted by Iranian study groups. This overlap of both medical systems is understandable. The usage of similar plants is explained by shared history: Arabic culture translated, preserved and developed the Greek/Roman knowledge on medical plants, which was later transmitted back to medieval Europe e. g. via the first medical schools of Salerno or al-Andalus (Leonti and Verpoorte 2017).
But how to assess which plants are the most commonly recommended in (popular) science literature in Germany? We took a leap back and screened several phytopharmacy/TEM books available on the German market for herbal remedies against oral mucositis/gingivitis and were surprised by the huge variety of plants (78 plants) recommended. However, only 12 plants of these were tested by studies found during first online literature research. This first part of our review shows an imbalance between research and daily life of our patients. It also describes a gap between scientific knowledge and clinical real-life.
Therefore, we compiled a list of the most often mentioned herbs and initiated a second online literature research using Latin plant designations as MESH terms. This might restrict the output of studies, as some authors may use common names—e.g. chamomile instead of Matricaria recutita L.—but is necessary, as we appreciate the huge variety of possible designations for one plant- be it in German or in English. So we here present an innovative approach to (1) get an impression which plants are the most commonly recommended herbals by TEM (and thus might have the highest probability to be used by our patients) and to (2) maximize the study count for later (semi-) quantitative analysis.
Despite having found 24 studies during qualitative analysis, we decided against calculating hazard ratios for meta-analysis as it would have severely reduced the study number available. We chose a compromise developing the score based on the p value (refer to Table 5) for semi-quantitative analysis of the 22 studies finally included. Herbal remedies are suitable to alleviate oral mucositis. A positive effect is described for most plants, excluding Plantago major L. While study number is too small to assess the value of plants against pharyngitis, we could describe a positive effect of most herbs on oral mucositis and gingivitis. Overall, chamomile was the most often investigated plant and also the herb at the top of our “hit list” of plants. Here, we show that Matricaria recutita L. has a good effect on mucositis: Out of the seven studies investigating the influence of herbals on oral pain (Fig. 6b), four studies used Matricaria recutita L. (no combinations with other plants) and reported all a positive effect on alleviating symptoms. Therefore, we propose to revaluate the national guidelines of supportive care management in oncology, where chamomile is excluded from recommendation due to a low level of evidence/missing studies (Leitlinienprogramm Onkologie|S3-Leitlinie Supportive Therapie 2017). Other plants should also be reconsidered for treating oral mucositis: Salvia officinalis L. and Thymus spp. L. did show a positive effect on oral mucositis. Both plants contain essential oils that have been shown to have an antimicrobial activity against multidrug-resistant S. aureus (Tardugno et al. 2018; Kot et al. 2018).
Conclusively, we hereby present an approach to evaluate herbal plants used and offered by TEM and to assess the evidence for these recommendations of TEM. The role of herbals should be reassessed for evidence as they are commonly used by our patients (Molassiotis et al. 2005). It would be a step to improve physician’s counselling role. Furthermore it could be a step forward to higher quality of information platforms and websites as it was mentioned by Ciarlo et al (2018).
References
Abdollahzadeh Sh, Mashouf RY, Mortazavi H et al (2011) Antibacterial and antifungal activities of Punica granatum peel extracts against oral pathogens. J Dent Tehran Iran 8:1–6
Ahmed KM (2013) The effect of olive leaf extract in decreasing the expression of two pro-inflammatory cytokines in patients receiving chemotherapy for cancer. A randomized clinical trial. Saudi Dent J 25:141–147. https://doi.org/10.1016/j.sdentj.2013.09.001
Ahmed KM, Talabani N, Altaei T (2013) Olive leaf extract as a new topical management for oral mucositis following chemotherapy: a microbiological examination, experimental animal study and clinical trial. Pharm Anal Acta 4:1–18. https://doi.org/10.4172/2153-2435.1000269
Andishe Tadbir A, Pourshahidi S, Ebrahimi H et al (2015) The effect of Matricaria chamomilla (chamomile) extract in Orabase on minor aphthous stomatitis, a randomized clinical trial. J Herb Med 5:71–76. https://doi.org/10.1016/j.hermed.2015.05.001
Aoyama T, Nishikawa K, Takiguchi N et al (2014) Double-blind, placebo-controlled, randomized phase II study of TJ-14 (hangeshashinto) for gastric cancer chemotherapy-induced oral mucositis. Cancer Chemother Pharmacol 73:1047–1054. https://doi.org/10.1007/s00280-014-2440-x
Azad MF, Schwiertz A, Jentsch HFR (2016) Adjunctive use of essential oils following scaling and root planing—a randomized clinical trial. BMC Complement Altern Med 16:171. https://doi.org/10.1186/s12906-016-1117-x
Babaee N, Mansourian A, Momen-Heravi F et al (2010) The efficacy of a paste containing Myrtus communis (Myrtle) in the management of recurrent aphthous stomatitis: a randomized controlled trial. Clin Oral Investig 14:65–70. https://doi.org/10.1007/s00784-009-0267-3
Bardellini E, Amadori F, Conti G, Majorana A (2016) Clinical efficacy of a solution composed by sodium bicarbonate and alginate, Aloe vera, propoli, chamomile, calendula and honey, in the treatment of minor recurrent aphthous stomatitis in children. Minerva Pediatr 68:507–509
Barrach RH, de Souza MP, da Silva DPC et al (2015) Oral changes in individuals undergoing hematopoietic stem cell transplantation. Braz J Otorhinolaryngol 81:141–147. https://doi.org/10.1016/j.bjorl.2014.04.004
Braga FTMM, Santos ACF, Bueno PCP et al (2015) Use of Chamomilla recutita in the prevention and treatment of oral mucositis in patients undergoing hematopoietic stem cell transplantation: a randomized, controlled, Phase II clinical trial. Cancer Nurs 38:322–329. https://doi.org/10.1097/NCC.0000000000000194
Büntzel J, Micke O, Mücke R et al (2018) CAM usage, cardiovascular risk behavior, and treatment compliance of long-term head and neck cancer survivors. Trace Elem Electrolytes 35:105–108
Büntzel J, Hübner J, Büntzel J (2019) Komplementärmedizinische Behandlungsansätze bei oraler Mukositis und Xerostomie. Onkol 25:269–274. https://doi.org/10.1007/s00761-019-0521-5
Cabrera-Jaime S, Martínez C, Ferro-García T et al (2018) Efficacy of Plantago major, chlorhexidine 0.12% and sodium bicarbonate 5% solution in the treatment of oral mucositis in cancer patients with solid tumour: a feasibility randomised triple-blind phase III clinical trial. Eur J Oncol Nurs Off J Eur Oncol Nurs Soc 32:40–47. https://doi.org/10.1016/j.ejon.2017.11.006
Oxford Centre for Evidence-based Medicine, (2009) Oxford centre for evidence-based medicine—levels of evidence (March 2009). In: CEBM. https://www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/. Accessed 31 Jul 2019
Charalambous A, Lambrinou E, Katodritis N et al (2017) The effectiveness of thyme honey for the management of treatment-induced xerostomia in head and neck cancer patients: a feasibility randomized control trial. Eur J Oncol Nurs Off J Eur Oncol Nurs Soc 27:1–8. https://doi.org/10.1016/j.ejon.2017.01.001
Ciarlo G, Rudolph I, Keinki C et al (2018) Information needs in cancer care—a comparison of patients’ and professionals’ needs. Trace Elem Electrolytes 35:109–116
Crowder SL, Douglas KG, Yanina Pepino M et al (2018) Nutrition impact symptoms and associated outcomes in post-chemoradiotherapy head and neck cancer survivors: a systematic review. J Cancer Surviv Res Pract 12:479–494. https://doi.org/10.1007/s11764-018-0687-7
Das D, Agarwal SK, Chandola HM (2011) Protective effect of Yashtimadhu (Glycyrrhiza glabra) against side effects of radiation/chemotherapy in head and neck malignancies. Ayu 32:196–199. https://doi.org/10.4103/0974-8520.92579
Dioscorides P, Berendes J (2019) Arzneimittellehre in Fünf Büchern. WENTWORTH Press, Sydney
Dos Reis PED, Ciol MA, de Melo NS et al (2016) Chamomile infusion cryotherapy to prevent oral mucositis induced by chemotherapy: a pilot study. Support Care Cancer Off J Multinatl Assoc Support Care Cancer 24:4393–4398. https://doi.org/10.1007/s00520-016-3279-y
Fidler P, Loprinzi CL, O’Fallon JR et al (1996) Prospective evaluation of a chamomile mouthwash for prevention of 5-FU-induced oral mucositis. Cancer 77:522–525. https://doi.org/10.1002/(SICI)1097-0142(19960201)77:3%3c522:AID-CNCR14%3e3.0.CO;2-6
Fürst R, Zündorf I (2015) Evidence-based phytotherapy in Europe: where do we stand? Planta Med 81:962–967. https://doi.org/10.1055/s-0035-1545948
Gavanji S, Larki B, Bakhtari A (2014) The effect of extract of Punica granatum var. pleniflora for treatment of minor recurrent aphthous stomatitis. Integr Med Res 3:83–90. https://doi.org/10.1016/j.imr.2014.03.001
George J, Hegde S, Rajesh KS, Kumar A (2009) The efficacy of a herbal-based toothpaste in the control of plaque and gingivitis: a clinico-biochemical study. Indian J Dent Res 20:480–482. https://doi.org/10.4103/0970-9290.59460
Ghalayani P, Zolfaghary B, Farhad AR et al (2013) The efficacy of Punica granatum extract in the management of recurrent aphthous stomatitis. J Res Pharm Pract 2:88–92. https://doi.org/10.4103/2279-042X.117389
Ghorbani A, Sadrzadeh A, Habibi E, et al. (2018) Efficacy of Camellia sinensis extract against Candida species in patients with denture stomatitis. Curr Med Mycol 4:15–18. 10.18502/cmm.4.3.174.
Goes P, Dutra CS, Lisboa MRP et al (2016) Clinical efficacy of a 1% Matricaria chamomile L. mouthwash and 0.12% chlorhexidine for gingivitis control in patients undergoing orthodontic treatment with fixed appliances. J Oral Sci 58:569–574. https://doi.org/10.2334/josnusd.16-0280
González Begné M, Yslas N, Reyes E et al (2001) Clinical effect of a Mexican sanguinaria extract (Polygonum aviculare L.) on gingivitis. J Ethnopharmacol 74:45–51
Haghpanah P, Moghadamnia AA, Zarghami A, Motallebnejad M (2015) Muco-bioadhesive containing ginger officinale extract in the management of recurrent aphthous stomatitis: a randomized clinical study. Casp J Intern Med 6:3–8
Hatakeyama H, Takahashi H, Oridate N et al (2015) Hangeshashinto improves the completion rate of chemoradiotherapy and the nutritional status in patients with head and neck cancer. ORL J Oto-Rhino-Laryngol Its Relat Spec 77:100–108. https://doi.org/10.1159/000381026
Hubbert M, Sievers H, Lehnfeld R, Kehrl W (2006) Efficacy and tolerability of a spray with Salvia officinalis in the treatment of acute pharyngitis—a randomised, double-blind, placebo-controlled study with adaptive design and interim analysis. Eur J Med Res 11:20–26
Huebner J, Micke O, Muecke R et al (2014) User rate of complementary and alternative medicine (CAM) of patients visiting a counseling facility for CAM of a German comprehensive cancer center. Anticancer Res 34:943–948
Jadad AR, Moore RA, Carroll D et al (1996) Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin Trials 17:1–12. https://doi.org/10.1016/0197-2456(95)00134-4
Jadad AR, Haynes RB, Hunt D, Browman GP (2000) The Internet and evidence-based decision-making: a needed synergy for efficient knowledge management in health care. CMAJ 162:362–365
Kato S, Saito A, Matsuda N et al (2017) Management of afatinib-induced stomatitis. Mol Clin Oncol 6:603–605. https://doi.org/10.3892/mco.2017.1184
Kono T, Satomi M, Chisato N et al (2010) Topical application of Hangeshashinto (TJ-14) in the treatment of chemotherapy-induced oral mucositis. World J Oncol 1:232–235. https://doi.org/10.4021/wjon263w
Kot B, Wierzchowska K, Piechota M et al (2018) Antimicrobial activity of five essential oils from lamiaceae against multidrug-resistant Staphylococcus aureus. Nat Prod Res. https://doi.org/10.1080/14786419.2018.1486314
Leonti M, Verpoorte R (2017) Traditional Mediterranean and European herbal medicines. J Ethnopharmacol 199:161–167. https://doi.org/10.1016/j.jep.2017.01.052
Mahyari S, Mahyari B, Emami SA et al (2016) Evaluation of the efficacy of a polyherbal mouthwash containing Zingiber officinale, Rosmarinus officinalis and Calendula officinalis extracts in patients with gingivitis: a randomized double-blind placebo-controlled trial. Complement Ther Clin Pract 22:93–98. https://doi.org/10.1016/j.ctcp.2015.12.001
Malm L, Möbus M (2018) Antibiotische Heilpflanzen: Über 50 Pflanzen und ihre Wirkung, 2nd edn. Bassermann Verlag
Martin MD, Sherman J, van der Ven P, Burgess J (2008) A controlled trial of a dissolving oral patch concerning glycyrrhiza (licorice) herbal extract for the treatment of aphthous ulcers. Gen Dent 56:206–210 (quiz 211–212, 224).
Marucci L, Farneti A, Di Ridolfi P et al (2017) Double-blind randomized phase III study comparing a mixture of natural agents versus placebo in the prevention of acute mucositis during chemoradiotherapy for head and neck cancer. Head Neck 39:1761–1769. https://doi.org/10.1002/hed.24832
Matsuda C, Munemoto Y, Mishima H et al (2015) Double-blind, placebo-controlled, randomized phase II study of TJ-14 (Hangeshashinto) for infusional fluorinated-pyrimidine-based colorectal cancer chemotherapy-induced oral mucositis. Cancer Chemother Pharmacol 76:97–103. https://doi.org/10.1007/s00280-015-2767-y
Micke O, Büntzel J (2013) Traditionelle Europäische Heilsysteme in der komplementären Onkologie. Onkol 19:125–131. https://doi.org/10.1007/s00761-012-2384-x
Micke O, Bruns F, Glatzel M et al (2009) Predictive factors for the use of complementary and alternative medicine (CAM) in radiation oncology. Eur J Integr Med 1:19–25. https://doi.org/10.1016/j.eujim.2009.02.001
Miranzadeh S, Adib-Hajbaghery M, Soleymanpoor L, Ehsani M (2015) Effect of adding the herb Achillea millefolium on mouthwash on chemotherapy induced oral mucositis in cancer patients: a double-blind randomized controlled trial. Eur J Oncol Nurs 19:207–213. https://doi.org/10.1016/j.ejon.2014.10.019
Molassiotis A, Fernández-Ortega P, Pud D et al (2005) Use of complementary and alternative medicine in cancer patients: a European survey. Ann Oncol 16:655–663. https://doi.org/10.1093/annonc/mdi110
Moriyama S, Hinode D, Yoshioka M et al (2018) Impact of the use of Kampo medicine in patients with esophageal cancer during chemotherapy:a clinical trial for oral hygiene and oral condition. J Med Investig 65:184–190. https://doi.org/10.2152/jmi.65.184
Mutluay Yayla E, Izgu N, Ozdemir L et al (2016) Sage tea-thyme-peppermint hydrosol oral rinse reduces chemotherapy-induced oral mucositis: a randomized controlled pilot study. Complement Ther Med 27:58–64. https://doi.org/10.1016/j.ctim.2016.05.010
Nasry SA, El Shenawy HM, Mostafa D, Ammar NM (2016) Different modalities for treatment of recurrent aphthous stomatitis. A Randomized clinical trial. J Clin Exp Dent 8:e517–e522. https://doi.org/10.4317/jced.52877
Nishikawa K, Aoyama T, Oba MS et al (2018) The clinical impact of Hangeshashinto (TJ-14) in the treatment of chemotherapy-induced oral mucositis in gastric cancer and colorectal cancer: analyses of pooled data from two phase II randomized clinical trials (HANGESHA-G and HANGESHA-C). J Cancer 9:1725–1730. https://doi.org/10.7150/jca.24733
Leitlinienprogramm Onkologie | S3-Leitlinie Supportive Therapie, 2017 Leitlinienprogramm Onkologie: Supportive Therapie. https://www.leitlinienprogramm-onkologie.de/leitlinien/supportive-therapie/. Accessed 11 Nov 2018
Puataweepong P, Dhanachai MDM, Dangprasert S, et al (2009) The efficacy of oral Aloe vera juice for radiation induced mucositis in head and neck cancer patients: a double-blind placebo-controlled study
Rubenstein EB, Peterson DE, Schubert M et al (2004) Clinical practice guidelines for the prevention and treatment of cancer therapy—induced oral and gastrointestinal mucositis. Cancer 100:2026–2046. https://doi.org/10.1002/cncr.20163
Saller R, Büechi S, Meyrat R, Schmidhauser C (2001) Combined herbal preparation for topical treatment of Herpes labialis Forsch Komplementarmedizin Klass Naturheilkunde. Res Complement Nat Class Med 8:373–382. https://doi.org/10.1159/000057255
Schapowal A, Berger D, Klein P, Suter A (2009) Echinacea/sage or chlorhexidine/lidocaine for treating acute sore throats: a randomized double-blind trial. Eur J Med Res 14:406–412. https://doi.org/10.1186/2047-783x-14-9-406
Schulz V, Hänsel R (2013) Rationale Phytotherapie: Ratgeber für die ärztliche Praxis. Springer-Verlag, New York
Seyyedi S-A, Sanatkhani M, Pakfetrat A, Olyaee P (2014) The therapeutic effects of chamomilla tincture mouthwash on oral aphthae: a randomized clinical trial. J Clin Exp Dent 6:e535–538. https://doi.org/10.4317/jced.51472
Shabanloei R, Ahmadi F, Vaez J, Ansarin K, Hajizadeh E, Javadzadeh Y, Dolathkah R, Gholchin M (2009) Alloporinol, chamomile and normal saline mouthwashes for the prevention of chemotherapy-induced stomatitis. J Clin Diagn Res 3:1537–1542
Shrivastava R, John GW (2006) Treatment of Aphthous Stomatitis with topical Alchemilla vulgaris in glycerine. Clin Drug Investig 26:567–573. https://doi.org/10.2165/00044011-200626100-00003
Steinmann D, Eilers V, Beynenson D et al (2012) Effect of Traumeel S on pain and discomfort in radiation-induced oral mucositis: a preliminary observational study. Altern Ther Health Med 18:12–18
Su CK, Mehta V, Ravikumar L et al (2004) Phase II double-blind randomized study comparing oral Aloe vera versus placebo to prevent radiation-related mucositis in patients with head-and-neck neoplasms. Int J Radiat Oncol Biol Phys 60:171–177. https://doi.org/10.1016/j.ijrobp.2004.02.012
Tardugno R, Pellati F, Iseppi R et al (2018) Phytochemical composition and in vitro screening of the antimicrobial activity of essential oils on oral pathogenic bacteria. Nat Prod Res 32:544–551. https://doi.org/10.1080/14786419.2017.1329730
Tavakoli Ardakani M, Ghassemi S, Mehdizadeh M et al (2016) Evaluating the effect of Matricaria recutita and Mentha piperita herbal mouthwash on management of oral mucositis in patients undergoing hematopoietic stem cell transplantation: a randomized, double blind, placebo controlled clinical trial. Complement Ther Med 29:29–34. https://doi.org/10.1016/j.ctim.2016.08.001
Tiemann P, Toelg M, Ramos FMH (2007) Administration of Ratanhia-based herbal oral care products for the prophylaxis of oral mucositis in cancer chemotherapy patients: a clinical trial. Evid-Based Complement Altern Med 4:361–366. https://doi.org/10.1093/ecam/nel070
Uehleke B (2007) Naturheilverfahren und «Traditionelle Europäische Medizin» TEM: Ergebnisse einer Experten-Umfrage (Delphi-Methode). Schweiz Z Für Ganzheitsmed Swiss J Integr Med 19:199–203. https://doi.org/10.1159/000283795
Widén C, Coleman M, Critén S et al (2015) Consumption of bilberries controls gingival inflammation. Int J Mol Sci 16:10665–10673. https://doi.org/10.3390/ijms160510665
Wortmann JK, Bremer A, Eich H et al (2016) Use of complementary and alternative medicine by patients with cancer: a cross-sectional study at different points of cancer care. Med Oncol 33:78. https://doi.org/10.1007/s12032-016-0790-4
Yamashita T, Araki K, Tomifuji M et al (2015) A traditional Japanese medicine–Hangeshashinto (TJ-14)–alleviates chemoradiation-induced mucositis and improves rates of treatment completion. Support Care Cancer 23:29–35. https://doi.org/10.1007/s00520-014-2315-z
Acknowledgements
Open Access funding provided by Projekt DEAL. We thank Dr. Julia Koenig for lively discussions and addressing methodical questions.
Funding
During 2019 Ju. B. was supported by the “Göttinger Kolleg für Translationale Medizin” (Ministry for Culture and Science, Lower Saxony, Germany), a program which funds clinician scientists.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors (Ju. B., C. B., J.B.) have no conflict of interests.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Buentzel, J., Bauer, C. & Buentzel, J. How to bridge the gap? European medical plants used for treating oral mucositis: on the search for evidence. J Cancer Res Clin Oncol 146, 985–1001 (2020). https://doi.org/10.1007/s00432-020-03124-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-020-03124-x