
Abstract
Purpose
Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the staging of clinically node-negative breast cancer patients (BCP), demonstrating equivalent survival to ALND while resulting in reduced morbidity. ALND has remained the standard of care for the majority of BCP with clinical axillary metastases or metastases found on SLN biopsy. More recently, it is debated whether ALND could be avoided not only in SLN-negative BCP but also in selected SLN-positive disease or even in all patients. This analysis of pN+ BCP shows the impact of the number of excised lymph nodes on RFS and OAS adjusted by age, tumor size, intrinsic subtypes and adjuvant systemic therapy.
Methods
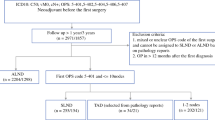
In this retrospective, multicenter cohort study, we investigated data from 2992 pN+ primary BCP recruited from 17 participating certified breast cancer centers in Germany between 2001 and 2008 within the BRENDA study group.
Results
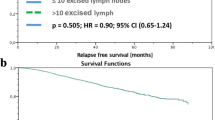
The median number of excised lymph nodes was 17. The number of excised lymph nodes was neither significant for RFS (p = 0.085) nor for OAS (p = 0.285). Adjustments were made for age, tumor size and intrinsic subtypes. The most important significant parameters for RFS were intrinsic subtypes (p < 0.001) and tumor size (p < 0.001) and for OAS age (p < 0.001) and intrinsic subtypes (p < 0.001). There were no significant differences in RFS and OAS in any subgroup stratified by the number of excised lymph nodes. Only for T3/T4 tumors, there is a very small significant advantage of ALND for RFS but not for OAS. After adjusting in addition by guideline adherence of adjuvant systemic therapy (AST), intrinsic subtypes and guideline-adherent AST are the most important significant (p < 0.001) parameters for RFS and OAS.
Conclusions
The number of excised lymph nodes of pN+ BCP neither correlates with RFS nor with OAS. Survival of pN+ BCP is primarily determined by the biology and the guideline-adherent AST based on the corresponding intrinsic subtypes. These results support the omission of a radical ALND at least for pN+ patients scheduled for breast-conserving surgery (not mastectomy), provided they receive whole breast irradiation and guideline-adherent AST.



Similar content being viewed by others

References
Atalay C (2014) New concepts in axillary management of breast cancer. World J Clin Oncol 5:895–900. doi:10.5306/wjco.v5.i5.895
Bodai BI, Tuso P (2015) Breast cancer survivorship: a comprehensive review of long-term medical issues and lifestyle recommendations. Perm J 19:48–79. doi:10.7812/TPP/14-241
Donker M, van Tienhoven G, Straver ME et al (2014) Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol 15:1303–1310. doi:10.1016/S1470-2045(14)70460-7
Engel J, Emeny RT, Hölzel D (2012) Positive lymph nodes do not metastasize. Cancer Metastasis Rev 31:235–246. doi:10.1007/s10555-011-9343-7
Erb KM, Julian TB (2009) Completion of axillary dissection for a positive sentinel node: necessary or not? Curr Oncol Rep 11:15–20. doi:10.1007/s11912-009-0004-8
Fitzal F, Galimberti V, Kühn T et al (2014) Lymph node staging in invasive breast cancer. Breast Care (Basel) 9:211–214. doi:10.1159/000365315
Galimberti V, Cole BF, Zurrida S et al (2013) Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23–01): a phase 3 randomised controlled trial. Lancet Oncol 14:297–305. doi:10.1016/S1470-2045(13)70035-4
Giuliano AE, Hunt KK, Ballman KV et al (2011) Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA 305:569–575. doi:10.1001/jama.2011.90
Giuliano AE, Morrow M, Duggal S, Julian TB (2012) Should ACOSOG Z0011 change practice with respect to axillary lymph node dissection for a positive sentinel lymph node biopsy in breast cancer? Clin Exp Metastasis 29:687–692. doi:10.1007/s10585-012-9515-z
Glechner A, Wöckel A, Gartlehner G et al (2012) Sentinel lymph node dissection only versus complete axillary lymph node dissection in early invasive breast cancer: a systematic review and meta-analysis. Eur J Cancer. doi:10.1016/j.ejca.2012.09.010
Halsted WS (1894) I. The results of operations for the cure of cancer of the breast performed at the Johns Hopkins Hospital from June, 1889, to January, 1894. Ann Surg 20:497–555
Hölzel D, Engel J (2011) Importance of lymph node dissection. Worthy of many questions. Chirurg 82:1106–1108. doi:10.1007/s00104-011-2118-4
Janni W, Kühn T, Schwentner L et al (2014) Sentinel node biopsy and axillary dissection in breast cancer: the evidence and its limits. Dtsch Arztebl Int 111:244–249. doi:10.3238/arztebl.2014.0244
Jin X, Mu P (2015) Targeting breast cancer metastasis. Breast Cancer (Auckl) 9:23–34. doi:10.4137/BCBCR.S25460
Kim T, Giuliano AE, Lyman GH (2006) Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma. Cancer 106:4–16. doi:10.1002/cncr.21568
Krakhmal NV, Zavyalova MV, Denisov EV et al (2015) Cancer invasion: patterns and mechanisms. Acta Naturae 7:17–28
Kreienberg R, Kopp I, Albert U-S et al (2012) Interdisziplinäre S3-Leitlinie und Nachsorge des Leitlinie. Ger Cancer Soc 7:32–45
Lips EH, Mulder L, de Ronde JJ et al (2013) Breast cancer subtyping by immunohistochemistry and histological grade outperforms breast cancer intrinsic subtypes in predicting neoadjuvant chemotherapy response. Breast Cancer Res Treat 140:63–71. doi:10.1007/s10549-013-2620-0
Lyman GH, Temin S, Edge SB et al (2014) Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 32:1365–1383. doi:10.1200/JCO.2013.54.1177
Olson JA, McCall LM, Beitsch P et al (2008) Impact of immediate versus delayed axillary node dissection on surgical outcomes in breast cancer patients with positive sentinel nodes: results from American College of Surgeons Oncology Group Trials Z0010 and Z0011. J Clin Oncol 26:3530–3535. doi:10.1200/JCO.2007.15.5630
Parise CA, Caggiano V (2014) Breast cancer survival defined by the ER/PR/HER2 subtypes and a surrogate classification according to tumor grade and immunohistochemical biomarkers. J Cancer Epidemiol 2014:469251. doi:10.1155/2014/469251
Ribelles N, Santonja A, Pajares B et al (2014) The seed and soil hypothesis revisited: current state of knowledge of inherited genes on prognosis in breast cancer. Cancer Treat Rev 40:293–299. doi:10.1016/j.ctrv.2013.09.010
Rui L, Wang X, Chen GY et al (2007) The prognostic role of a gene signature from tumorigenic breast-cancer cells. N Engl J Med. http://www.nejm.org/doi/full/10.1056/NEJMoa063994. Accessed 12 Sep 2015
Schmidt-Hansen M, Bromham N, Hasler E, Reed MW (2016) Axillary surgery in women with sentinel node-positive operable breast cancer: a systematic review with meta-analyses. Springerplus 5:85. doi:10.1186/s40064-016-1712-9
Sihto H, Lundin J, Lundin M et al (2011) Breast cancer biological subtypes and protein expression predict for the preferential distant metastasis sites: a nationwide cohort study. Breast Cancer Res 13:R87. doi:10.1186/bcr2944
Tanis PJ, Nieweg OE, Valdés Olmos RA et al (2001) History of sentinel node and validation of the technique. Breast Cancer Res 3:109–112
Veronesi U, Orecchia R, Zurrida S et al (2005) Avoiding axillary dissection in breast cancer surgery: a randomized trial to assess the role of axillary radiotherapy. Ann Oncol 16:383–388. doi:10.1093/annonc/mdi089
Viale G, Maiorano E, Pruneri G et al (2005) Predicting the risk for additional axillary metastases in patients with breast carcinoma and positive sentinel lymph node biopsy. Ann Surg 241:319–325. doi:10.1097/01.sla.0000150255.30665.52
von Minckwitz G, Untch M, Blohmer J-U et al (2012) Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 30:1796–1804. doi:10.1200/JCO.2011.38.8595
Acknowledgements
We express our thanks to the following persons for their contributions to the BRENDA study: Karsten Gnauert (Ostalbklinikum, Aalen), Steffen Fritz (Kreisklinik Biberach), Ulf Göretzlehner (Kreiskrankenhaus Ehingen), Hans-Walter Vollert (Städt. Krankenhaus Friedrichshafen), Peter Jakob Albert (Klinikum Heidenheim), Ricardo Felberbaum (Klinikum Kempten), Andreas Zorr (Klinikum Konstanz), Felix Flock (Klinikum Memmingen), Erik Schlicht (Stauferklinik, Mutlangen), Martina Gropp-Meier (Oberschwabenklinik Ravensburg), Gerhard Bartzke (Kreiskrankenhaus Rottweil), Andreas Rempen (Diakonie-Krankenhaus, Schwäbisch Hall), Edgar Schelble (Kreiskrankenhaus Sigmaringen), Theodor Dinkelacker (Helfenstein-Klinik Geislingen), Andreas Grüneberger (Oberschwabenklinik Wangen) and Thorsten Kühn (Städt. Kliniken, Esslingen).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that there are no potential conflicts of interest, including any financial, personal or other relationships with people or organizations that could inappropriately influence this work.
Funding source
This study was supported by the German Federal Ministry of Education and Research (BMBF-Grant-01ZP0505).
Ethical approval
This study and the BRENDA project have been approved by the ethics committee of the University of Ulm.
Rights and permissions
About this article

Cite this article
Ebner, F., Wöckel, A., Janni, W. et al. Personalized axillary dissection: the number of excised lymph nodes of nodal-positive breast cancer patients has no significant impact on relapse-free and overall survival. J Cancer Res Clin Oncol 143, 1823–1831 (2017). https://doi.org/10.1007/s00432-017-2425-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-017-2425-3