
Abstract
This study aims to examine the association between different versions of a provegetarian food pattern and micronutrient adequacy in a population of children from the SENDO Project. Children aged 4–5 years old were recruited and baseline information on diet, lifestyle and socio-demographic characteristics was collected through self-administered online questionnaires completed by their parents. Scores were calculated for overall, healthful, and unhealthful provegetarian food patterns (FP) using an a priori approach. Participants were categorized into tertiles according to their scores. Micronutrient adequacy was assessed using the Estimated Average Requirement (EAR) cut-off point. Multivariate analyses were performed to evaluate the relationship between tertiles of each provegetarian FP and the risk of inadequate micronutrient intake (failing to meet ≥ 3 requirements). Despite lower intakes of certain micronutrients, children with higher scores in the healthful provegetarian FP did not exhibit a higher prevalence of inadequacy. Children in the highest tertile of this index had 0.47-fold lower odds (95%CI 0.23–0.95) of having ≥ 3 inadequate micronutrient intakes than their peers in the lowest tertile, after adjusting for potential confounders. In contrast, children in the highest tertile of the unhealthful provegetarian FP had 20.06-fold higher odds (95%CI 9.19–43.79) of having ≥ 3 inadequate micronutrient intakes compared to children in the lowest tertile.
Conclusions: Adherence to a healthful provegetarian food pattern is associated with improved nutritional adequacy in preschoolers, while following an unhealthful pattern is detrimental to micronutrient adequacy. These results suggest that moderate reductions in animal food consumption within a healthy diet may not compromise micronutrient adequacy in young children. Further research is needed to explore the impact of diets reduced in animal food intake on the health of children.
What is Known: • There's a notable trend towards plant-based diets due to health and sustainability concerns. • Research links plant-based diets in adults with lower risks of obesity, cardiovascular disease, and cancer. |
What is New: • A new study examines how different versions of a provegetarian food pattern affect micronutrient adequacy in children, using a moderate and stepwise approach. • Following a healthful provegetarian food pattern enhances nutritional adequacy in preschoolers, whereas an unhealthful pattern negatively impacts micronutrient adequacy. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In recent years, increasing sectors of the population are shifting to dietary patterns that restrict animal products, motivated by health considerations and other concerns related to the sustainability of the environment, animal welfare or religious reasons. In adults, plant-based diets such as vegetarian or vegan diets have been associated with a lower risk of obesity, cardiovascular disease, and cancer, and from an environmental perspective with a smaller ecological impact [1,2,3,4].
There is some concern as to whether diets restricted in animal-derived foods can fulfill nutritional requirements in childhood and adolescence, due to the increased needs related to rapid growth and development. However, evidence is still scarce, and debate is ongoing regarding the nutritional adequacy of dietary patterns with high or total restriction of animal-derived foods during childhood [5,6,7,8,9].
Moreover, not all plant-based diets fall under the categories of vegetarian or vegan [10, 11]. In general, plant-based diets emphasize plant products, such as wholegrains, fruits, vegetables, nuts, legumes and seeds, and limit or avoid animal products. But the amount and type of animal food restriction can vary substantially among different plant-based diets. Some authors have referred to those more flexible patterns as flexitarian, semi-vegetarian or provegetarian, but the wide spectrum of plant-based dietary patterns, with varying degrees of animal restriction, is difficult to encompass with simple definitions [10].
Thus, Martínez-González et al. proposed a provegetarian food pattern (FP) score, that weights positively plant-based foods and negatively animal-derived foods [12]. Satija et al. later developed two additional scores, a healthful and an unhealthful plant-based diet index, to account for differences in dietary choices, as not all “provegetarian” FP are necessarily healthy [13]. Recent evidence has shown that the overall provegetarian FP score and its healthful version are associated with favorable health outcomes in adults, such as lower risk of nutritional inadequacy [14], overweight and obesity [15], cardiometabolic disease [13, 16, 17], diabetes [4], specific cancers [18], and all-cause mortality [12, 16, 19].
To date, there is no study on provegetarian FPs and children’s health. Since the question of nutrient adequacy in children consuming restrictive diets is a longstanding controversy, it would be important to analyze the question under the lens of a moderate and stepwise approach, as provided by the provegetarian FP score conceptual framework [12].
Therefore, this study aims to investigate the association between different versions of a provegetarian FP (overall, healthful, and unhealthful) and micronutrient adequacy, in a population of children from the SENDO Project (Seguimiento del Niño para un Desarrollo Óptimo).
Material and methods
Study population
The SENDO Project is a dynamic, prospective cohort of Spanish children that began recruiting participants in 2015 (https://www.proyectosendo.es/). Its primary aim is to assess the effect of lifestyle and diet on the health of children and adolescents. Participants are invited to join the cohort by their pediatrician at their health care center or by the SENDO team of researchers through schools. Inclusion criteria are being a child 4 or 5 years old and residing in Spain. The sole exclusion criterion is the impossibility to access a device connected to the internet to fulfill the online questionnaires. Self-reported questionnaires are completed online by the child’s parents and collected at baseline and updated every year. The baseline questionnaire collects information related to lifestyle, diet, medical history, anthropometric and sociodemographic variables.
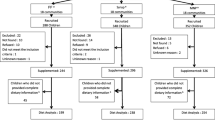
This cross-sectional study is based on baseline information of participants recruited between January 2015 and June 2023. A total of 1208 participants were recruited. We excluded 141 participants who reported extreme energy intake (< P1 or > P99) and 118 with extreme micronutrient intakes (≥ + 3 or ≤ -3 standard deviations (SD) from the mean). Lastly, 85 participants were additionally excluded for presenting incomplete questionnaires at baseline. Thus, the final sample included 864 participants.
Ethical approval
The SENDO project adheres to the rules of the Declaration of Helsinki on the ethical principles for medical research in human beings. This study was approved by the Ethics Committee for Clinical Research of Navarra (P. 2016/122). An informed consent was obtained during the recruitment from all participants’ parents.
Dietary Assessment
The usual dietary intake information was collected through a validated semi-quantitative 147-item food-frequency questionnaire (FFQ) [20] completed by the parents.
Provegetarian FP Scores
We calculated adherence to a provegetarian FP based on three scores: an overall provegetarian FP score [12] and two additional ones, that distinguish between healthful and unhealthful plant-based foods (healthful provegetarian and unhealthful provegetarian FP scores) [13]. The scoring criteria for all three scores are shown in Table 1 and has been described in previous studies [4, 12, 13, 15].
For the analysis of the overall provegetarian FP, we included 7 different plant food groups (fruits, vegetables, potatoes, nuts, legumes, grains, and olive oil) and 5 animal food groups (dairy, eggs, meat, fish and seafood, and animal fat), as originally proposed [13]. Food consumption (g/d) was adjusted for total energy intake by using the residual method. The energy-adjusted estimates were ranked into quintiles (for plant-based food groups) and reverse quintiles (for animal food groups). For plant-based food groups, a value of 1 was assigned to the first quintile, 2 to the second quintile, and so on, until 5 was assigned to the fifth quintile. For animal products quintiles were reversed (assigning a value of 5 to the first quintile, 4 to the second quintile, and so on, until a value of 1 was assigned to the fifth quintile). Final score ranged from 12 (lowest adherence) to 60 (highest adherence).
The healthful and unhealthful scores were constructed according to the criteria exposed by Satija et al. [4], by dividing plant-food groups according to their impact on health. The analysis included 17 items for both scores. Unlike the original index designed for adults, the item 'tea/coffee’ was not included in the score since our study focused on children. Food consumption was also adjusted for total energy intake (residual method) [21]. For the healthful provegetarian FP, we assigned quintile values for healthful plant food consumption and reverse quintiles values for animal food consumption and unhealthful plant food consumption. For the unhealthful provegetarian FP, we assigned quintile values for unhealthful plant food consumption and reverse quintiles values for animal food consumption and healthful plant food consumption. Final scores for both indexes ranged from 17 (lowest adherence) to 85 (highest adherence).
We also analyzed dietary intake through 16 different food groups: vegetables, fruits, legumes, grains, nuts, olive oil, potatoes, fruit juices, dairy, eggs, fish and seafood, meat, animal fat, sugar-sweetened beverages, pastries and sweets, beverages, and miscellaneous. Lastly, we separately assessed adherence to the Mediterranean diet by using the KIDMED score, which has been described previously [22].
Covariates
The participants’ sociodemographic information was reported by their parents. The questionnaire on physical activity collected information on 14 types of activities, with 10 different possible answers, ranging from never to ≥ 11 h per week. Participants indicated the average time dedicated to each activity in the previous year. Screen time was assessed by averaging the daily hours spent using screens (TV, computer, or video games). Time spent on weekdays and weekends was assessed separately.
Parental attitudes towards their child’s dietary habits were assessed with 8 yes/no questions, scored positively for healthy attitudes and given no point for unhealthy ones. Parental knowledge on dietary recommendations for children were evaluated with questions on the recommended intake frequency of 18 food groups. Both scores have been described in previous articles [23, 24]
Outcome assessment
We assessed the intake of 20 micronutrients, including vitamins A, C, D, E, B1, B2, B3, B6, B12, folic acid, Calcium (Ca), Iodine (I), Iron (Fe), Phosphorous (P), Magnesium (Mg), Selenium (Se), Zinc (Zn), Chromium (Cr), Potassium (K) and Sodium (Na). Participants were considered to have an inadequate micronutrient intake when their intake was inferior to the estimated average requirement (EAR), (or to the adequate intake (AI) if the EAR was not available), as established by the Institute of Medicine [25].
Statistical analysis
Participants were divided into tertiles according to their provegetarian FP scores, with the highest tertile representing higher adherence and the lowest tertile representing lower adherence. Participants’ sociodemographic characteristics were presented according to their adherence to the overall provegetarian FP and information on nutrient and food group intake was presented according to adherence to all three provegetarian FPs. Numbers and percentages were used for categorical variables and means and SD were used for continuous variables. Linear trend tests across tertiles of each score were calculated by assigning the median of each tertile and treating this variable as continuous in regression models. We also assessed the prevalence of inadequate intake of each micronutrient in each tertile of the three patterns.
Multivariate analyses were used to assess the relationship between each provegetarian FPs and the risk of having ≥ 3 inadequate intakes, by using the EAR cut-point method. We fitted generalized estimating equations to account for intra-cluster correlation between siblings.
Analyses were progressively adjusted, in different models, for the following potential confounding factors: 1) age (continuous), sex, and total energy intake (continuous); 2) breastfeeding duration (none, < 6 months, 6–12 months, and > 12 months), number of siblings (1, 2, 3–4, 5 or more), parental knowledge about nutritional recommendations for children (low, medium or high) and parental attitudes towards child’s dietary habits (unhealthy, average or healthy); 3) physical activity (continuous) and screen time (continuous). The first tertile was used as category of reference.
For our analysis, we calculated 1) the number of micronutrients with inadequate intake (and 95% Confidence Interval (CI)) by tertiles of provegetarian scores and 2) the Odds Ratio (OR) and 95% CI for the inadequate intake of ≥ 3 micronutrients across tertiles of the three provegetarian FPs. We also estimated the adjusted proportions of children with inadequate intake of ≥ 3 micronutrients in each tertile of the three patterns.
Lastly, different sensitivity analysis were performed to assess the robustness of our findings: 1) we included the intake of supplements to the total intake of micronutrients calculated for each participant; and 2) we changed the outcome to an inadequate intake of ≥ 4 micronutrients.
Statistical analyses were carried out using Stata version 15.0 (Stata Corp., College Station, TX, USA). All p values are two-tailed and statistical significance was settled at the conventional cut-off point of p < 0.05.
Results
This cross-sectional study included 864 participants (50.5% girls) with an average age of 5.0 years (SD: 0.8). The participants’ main characteristics according to tertiles of the overall provegetarian FP index are presented in Table 2.
Children with higher scores (T3) had slightly higher energy intakes, had been breastfed for a longer period, and were more physically active. Their parents displayed healthier attitudes towards their child’s dietary habits and had greater knowledge regarding child nutrition. On the other hand, participants with lower scores (T1) came from more numerous families.
Regarding dietary composition, as displayed in Table 3, participants with higher adherence to the overall provegetarian FP (T3) consumed proportionally more carbohydrates, and less protein and fat. They also consumed slightly less saturated fat. Lastly, they consumed more fruits and vegetables, legumes, cereal grains, potatoes and nuts but less animal products than their peers in T1.
We calculated the energy-adjusted mean intake for each micronutrient in each tertile of the three scores (Table 4). In the overall provegetarian FP, participants in T3 had higher intakes of vitamins A, C, E, B1, and B6, and folate, Fe, Mg, Cr, and K, compared to children in T1. Conversely, they had lower intakes of vitamins D, B2, and B12, and Ca, I, P, Zn and Na. Regarding the healthful provegetarian FP, participants in T3 had higher intakes of vitamins A, C, E, B1, B2, B3, B6, folate, Fe, P, Mg, Cr and K, compared to those in T1. On the contrary, they displayed lower intakes of vitamin B12, Ca, I, Se, Zn and Na. Despite these lower intakes, participants in the highest tertile of the healthful provegetarian FP score did not exhibit a higher prevalence of inadequacy of any micronutrient, compared to children in T1. Lastly, regarding the unhealthful provegetarian FP, participants in T3 had lower intakes of all micronutrients and higher prevalence of micronutrient inadequacy for vitamins A, C, and E, and folate, Ca, I, and K, compared to children in T1.
After adjusting for potential confounders, we observed that the number of micronutrients with unmet EAR in each tertile decreased as the overall provegetarian FP score improved (p < 0.001) (Fig. 1). With the healthful provegetarian FP, the tendency was more pronounced. Conversely, the number of inadequate intakes of micronutrients rises as adherence to the unhealthful provegetarian FP increases.

Number of micronutrients with inadequate intake (95% CI) in each tertiles of the overall, healthful, and unhealthful provegetarian FP scores. Adjusted for sex, age, energy intake, breastfeeding duration, number of siblings, parental knowledge about nutritional recommendations for children, parental attitudes towards child’s dietary habits, physical activity, and screen time. Number of micronutrients with inadequate intake: Overall provegetarian FP : T1: 1.71% (95% CI: 1.62%-1.81%), T2 : 1.65% (95% CI: 1.53%-1.76%), T3 : 1.53% (95% CI: 1.44%-1.62%). Healthful provegetarian FP : T1: 1.87% (95% CI: 1.76%-20.9%), T2 : 1.54% (95% CI: 1.46%-1.62%), T3 : 1.45% (95% CI: 1.35%-1.54%). Unhealthful Provegetarian FP : T1: 1.30% (95% CI: 1.22%-1.38%), T2: 1.65% (95% CI; 1.55%-1.75%); T3 : 2.03% (95% CI: 1.89%-2.16%)
Table 5 shows a significant linear trend in the odds of having ≥ 3 inadequate micronutrient intake across tertiles of the healthful provegetarian FP score. In the most adjusted model, participants in T3 had 0.47-fold lower odds (95%CI: 0.23–0.95) of having ≥ 3 inadequate intakes than those in T1 (p for trend = 0.015). An opposite trend could be observed for the unhealthful provegetarian FP score: participants in T3 had 20.06 higher odds (95%CI 9.2%-43.8%) of having ≥ 3 inadequate intakes of micronutrients (p for trend < 0.001) than their peers in T1.
The adjusted proportions of children with inadequate intake of ≥ 3 micronutrients in each tertile of the three indexes are presented in Fig. 2.

Adjusted proportions of children with ≥ 3 inadequate micronutrient intake (95% CI) in each tertile of the overall, healthful, and unhealthful provegetarian FP scores. Adjusted for sex, age, energy intake, breastfeeding duration, number of siblings, parental knowledge about nutritional recommendations for children, parental attitudes towards child’s dietary habits, physical activity and screen time. Adjusted proportions of children with ≥ 3 inadequate intakes: Overall provegetarian FP : T1: 15.7% (95% CI: 12.8%-18.6%), T2 : 13.0% (95% CI: 9.5%-16.5%), T3 : 14.8% (95% CI: 10.9%-18.8%). Healthful provegetarian FP : T1: 17.9% (95% CI: 14.8%-20.9%), T2 : 12.0% (95% CI: 8.7%-15.4%), T3 : 11.9% (95% CI: 7.7%-16.1%). Unhealthful Provegetarian FP : T1: 6.1% (95% CI: 3.9%-8.4%), T2: 15.6% (95% CI; 12.5%-18.9%); T3 : 27.1% (95% CI: 22.7%-31.6%)
Finally, these results remained significant after performing two sensitivity analyses that accounted for supplement use (Table S4) and explored the association of provegetarian FP scores with the odds of not meeting the EAR for ≥ 4 micronutrients.
Discussion
In this cross-sectional study of Spanish preschoolers we analyzed the association between provegetarian FPs and micronutrient adequacy by using an overall provegetarian FP score and two others to distinguish between healthful and unhealthful provegetarian FPs. We did not find a significant association between the overall provegetarian FP and micronutrient adequacy, though the point estimates suggested that a higher adherence to the overall provegetarian FP was associated with lower risk of inadequacy. However, we did observe an inverse association between the healthful provegetarian FP score and the number of micronutrients with unmet EAR. On the other hand, a harmful association was observed for the unhealthful provegetarian FP: higher adherence was associated with higher prevalence of micronutrient inadequacy.
Overall, our findings add evidence in favor of provegetarian FPs when they are based on healthy plant-based foods. On the contrary, the sole elimination of animal-derived foods without improving the quality of plant foods appears to be detrimental to micronutrient adequacy. In line with this, previous research has shown that low-quality diets, particularly those high in ultra processed foods, can compromise nutrient adequacy in children [26].
Notably, children with higher adherence to the healthful provegetarian FP displayed higher intakes of all micronutrients except for vitamin B12, Ca, I, Se, and Zn. It has been previously reported that consuming these micronutrients in sufficient amounts can prove to be challenging when decreasing the intake of animal foods [8, 9, 27, 28]. A recent study conducted in adults found that a greater adherence to a healthful provegetarian FP negatively affected the intakes of those same micronutrients [14]. In line with this, several authors have expressed concerns that the EAT-Lancet reference diet, a planetary flexitarian diet with low targets for animal product intake, may fall short in a similar range of micronutrients (vitamins B12 and D, Ca, I, Se, and Zn) both in adults [29, 30] and children [31]. This is particularly relevant since these critical nutrients are consumed in insufficient amounts worldwide, both by adults and children [32,33,34]. In addition, experts have pointed out that the high content in phytate of plant-based diets could further affect their status by hindering their absorption [35].
In our study, despite lower intakes of vitamin B12, Ca, I, Se, and Zn in the group with highest adherence to the healthful provegetarian FP, this did not translate to a decrease in adequacy for any micronutrient (Table 4). Nonetheless, it is important to highlight that our participants, even in the highest tertiles of all three patterns, still consumed animal-derived products in amounts that significantly exceeded the dietary targets defined by the EAT-Lancet diet [1], even if their average intake was overall lower than those reported in population-based studies in Spain [36]. These findings indicate that there is room for reduction of animal food consumption without harming nutritional adequacy in our population of preschoolers, and presumably in other similar populations with equal or higher consumption of animal-derived foods. Future studies with a broader range of provegetarian FPs among participants might further elucidate the question and provide evidence to address these concerns in future dietary guidelines.
We acknowledge that our study has limitations. First, our study is based on self-reported information which could come with measurement errors. FFQ tend to overestimate food intake, and this extends to nutrient intake, which could have led to underestimate actual micronutrient inadequacies in our participants. However, the FFQ used in this study has been previously validated [20] and we have excluded participants with extreme energy and micronutrient intakes in our analyses. Second, the participants of the SENDO cohort tend to present a better diet quality than that of the average Spanish children [37], which can be explained by the fact that our participants have highly educated parents and that most participants enrolled in cohort studies focused on nutrition tend to be more health conscious in general [38]. This particularity of our sample could have resulted in a lower number of nutrient inadequacies than those that might have shown up in other population-based studies. However, this does not in itself invalidate our conclusions as they should be generalized based on subjacent mechanisms and not on the representativeness of our sample [39]. Third, we have assessed probability of micronutrient adequacy but not actual micronutrient deficiency, which can be better assessed through biomarkers. Finally, given that our study is observational, we cannot exclude the possibility of residual confounding by unknown factors.
On the other hand, our study displays several strengths: to the best of our knowledge, this is first study to analyze the relation between provegetarian FPs and micronutrient adequacy in children. Secondly, its extensive questionnaire enabled us to adjust the data for many potential confounders. Thirdly, the FFQ has been previously validated [20]. Finally, we used GEE models to take into account the potential correlation between siblings, which is a common limitation of studies in pediatric populations.
In conclusion, our results show that adherence to a healthful provegetarian FP is associated with improved nutritional adequacy in young children. In contrast, following an unhealthful provegetarian FP proved significantly detrimental to micronutrient adequacy. Our findings suggest that the reduction of animal food consumption in pediatric populations with moderate intakes of animal foods, in the context of a healthy diet, can probably be carried without compromising micronutrient adequacy. However, our reliance on self-reported dietary data, the specific characteristics of our sample, and the focus on micronutrient adequacy rather than actual deficiency limit the generalizability of our findings. More research is needed to better understand the relationship between provegetarian FPs and micronutrient adequacy in children, with an emphasis on using biomarkers for more accurate assessment.
Data availability
Data is available on request.
Abbreviations
- AI:
-
Adequate Intake
- BMI:
-
Body Mass Index
- CI:
-
Confidence Interval
- EAR:
-
Estimated Average Requirement
- FFQ:
-
Food-Frequency Questionnaire
- FP:
-
Food pattern
- OR:
-
Odds Ratio
- SD:
-
Standard Deviation
- SENDO:
-
Seguimiento del Niño para un Desarrollo Óptimo
- T1:
-
Tertile 1
- T2:
-
Tertile 2
- T3:
-
Tertile 3
- TEI:
-
Total Energy Intake
- Ca:
-
Calcium
- I:
-
Iodine
- Fe:
-
Iron
- P:
-
Phosphorous
- M:
-
Magnesium
- Se:
-
Selenium
- Zn:
-
Zinc
- Cr:
-
Chromium
- K:
-
Potassium
- Na:
-
Sodium
References
Willett W, Rockström J, Loken B, Springmann M, Lang T, Vermeulen S et al (2019) Food in the Anthropocene: the EAT–Lancet Commission on healthy diets from sustainable food systems. The Lancet 393:447–492. https://doi.org/10.1016/S0140-6736(18)31788-4
Dybvik JS, Svendsen M, Aune D (2023) Vegetarian and vegan diets and the risk of cardiovascular disease, ischemic heart disease and stroke: a systematic review and meta-analysis of prospective cohort studies. Eur J Nutr 62:51–69. https://doi.org/10.1007/s00394-022-02942-8
Oussalah A, Levy J, Berthezène C, Alpers DH, Guéant J-L (2020) Health outcomes associated with vegetarian diets: An umbrella review of systematic reviews and meta-analyses. Clin Nutr 39:3283–3307. https://doi.org/10.1016/j.clnu.2020.02.037
Satija A, Bhupathiraju SN, Rimm EB, Spiegelman D, Chiuve SE, Borgi L et al (2016) Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med 13:e1002039. https://doi.org/10.1371/journal.pmed.1002039
Schürmann S, Kersting M, Alexy U (2017) Vegetarian diets in children: a systematic review. Eur J Nutr 56:1797–1817. https://doi.org/10.1007/s00394-017-1416-0
Desmond MA, Sobiecki JG, Jaworski M, Płudowski P, Antoniewicz J, Shirley MK et al (2021) Growth, body composition, and cardiovascular and nutritional risk of 5- to 10-y-old children consuming vegetarian, vegan, or omnivore diets. Am J Clin Nutr 113:1565–1577. https://doi.org/10.1093/ajcn/nqaa445
Weder S, Keller M, Fischer M, Becker K, Alexy U (2022) Intake of micronutrients and fatty acids of vegetarian, vegan, and omnivorous children (1–3 years) in Germany (VeChi Diet Study). Eur J Nutr 61:1507–1520. https://doi.org/10.1007/s00394-021-02753-3
Chouraqui J-P (2023) Risk Assessment of Micronutrients Deficiency in Vegetarian or Vegan Children: Not So Obvious. Nutrients 15:2129. https://doi.org/10.3390/nu15092129
Bakaloudi DR, Halloran A, Rippin HL, Oikonomidou AC, Dardavesis TI, Williams J et al (2021) Intake and adequacy of the vegan diet. A systematic review of the evidence. Clin Nutr 40:3503–21. https://doi.org/10.1016/j.clnu.2020.11.035
Kent G, Kehoe L, Flynn A, Walton J (2022) Plant-based diets: a review of the definitions and nutritional role in the adult diet. Proceed Nutr Soc 81:62–74. https://doi.org/10.1017/S0029665121003839
Hargreaves SM, Rosenfeld DL, Moreira AVB, Zandonadi RP (2023) Plant-based and vegetarian diets: an overview and definition of these dietary patterns. Eur J Nutr 62:1109–1121. https://doi.org/10.1007/s00394-023-03086-z
Martínez-González MA, Sánchez-Tainta A, Corella D, Salas-Salvadó J, Ros E, Arós F et al (2014) A provegetarian food pattern and reduction in total mortality in the Prevención con Dieta Mediterránea (PREDIMED) study. Am J Clin Nutr 100:320S-328S. https://doi.org/10.3945/ajcn.113.071431
Satija A, Bhupathiraju SN, Spiegelman D, Chiuve SE, Manson JE, Willett W et al (2017) Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S Adults. J Am Coll Cardiol. 70:411–22. https://doi.org/10.1016/j.jacc.2017.05.047
Asfura-Carrasco D, Santiago S, Zazpe I, Gómez-Donoso C, Bes-Rastrollo M, Martínez-González MÁ (2023) Healthful and unhealthful provegetarian food patterns and micronutrient intake adequacy in the SUN cohort. Public Health Nutr 26:563–574. https://doi.org/10.1017/S136898002200204X
Gómez-Donoso, Martínez-González, Martínez, Gea, Sanz-Serrano, Perez-Cueto et al (2019) A Provegetarian Food Pattern Emphasizing Preference for Healthy Plant-Derived Foods Reduces the Risk of Overweight/Obesity in the SUN Cohort. Nutrients 11:1553. https://doi.org/10.3390/nu11071553
Kim H, Caulfield LE, Garcia‐Larsen V, Steffen LM, Coresh J, Rebholz CM (2019) Plant‐Based Diets Are Associated With a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All‐Cause Mortality in a General Population of Middle‐Aged Adults. J Am Heart Assoc 8. https://doi.org/10.1161/JAHA.119.012865
Oncina-Cánovas A, Vioque J, González-Palacios S, Martínez-González MÁ, Salas-Salvadó J, Corella D et al (2022) Pro-vegetarian food patterns and cardiometabolic risk in the PREDIMED-Plus study: a cross-sectional baseline analysis. Eur J Nutr 61:357–372. https://doi.org/10.1007/s00394-021-02647-4
Oncina-Cánovas A, González-Palacios S, Notario-Barandiaran L, Torres-Collado L, Signes-Pastor A, de-Madaria E et al (2022) Adherence to Pro-Vegetarian Food Patterns and Risk of Oesophagus, Stomach, and Pancreas Cancers: A Multi Case–Control Study (The PANESOES Study). Nutrients 14:5288. https://doi.org/10.3390/nu14245288
Baden MY, Liu G, Satija A, Li Y, Sun Q, Fung TT et al (2019) Changes in Plant-Based Diet Quality and Total and Cause-Specific Mortality. Circulation 140:979–991. https://doi.org/10.1161/CIRCULATIONAHA.119.041014
Zazpe I, Santiago S, de la O V, Romanos-Nanclares A, Rico-Campà A, Álvarez-zallo N et al (2020) Validity and reproducibility of a semi-quantitative food frequency questionnaire in Spanish preschoolers — The SENDO project. Nutr Hosp. https://doi.org/10.20960/nh.03003
Willett W, Howe G, Kushi L (1997) Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr 65:1220S-1228S. https://doi.org/10.1093/ajcn/65.4.1220S
Serra-Majem L, Ribas L, Ngo J, Ortega RM, García A, Pérez-Rodrigo C et al (2004) Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 7:931–5. https://doi.org/10.1079/phn2004556
Santiago S, Benítez-Borja A, Martín-Calvo N, Romanos-Nanclares A, Moreno-Galarraga L, Zazpe I (2021) Association between parental attitudes towards their offspring’s diet and children’s actual dietary habits — The SENDO project. Nutr Hosp. https://doi.org/10.20960/nh.03649
Romanos-Nanclares A, Zazpe I, Santiago S, Marín L, Rico-Campà A, Martín-Calvo N (2018) Influence of Parental Healthy-Eating Attitudes and Nutritional Knowledge on Nutritional Adequacy and Diet Quality among Preschoolers: The SENDO Project. Nutrients 10:1875. https://doi.org/10.3390/nu10121875
National Institutes of Health USD of H and HServices. Nutrient Recommendations and Databases . https://ods.od.nih.gov/HealthInformation/nutrientrecommendations.aspx.
García-Blanco L, de la O V, Santiago S, Pouso A, Martínez-González MÁ, Martín-Calvo N (2023) High consumption of ultra-processed foods is associated with increased risk of micronutrient inadequacy in children: The SENDO project. Eur J Pediatr 182:3537–47. https://doi.org/10.1007/s00431-023-05026-9
Neufingerl N, Eilander A (2021) Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 14:29. https://doi.org/10.3390/nu14010029
Moreno LA, Meyer R, Donovan SM, Goulet O, Haines J, Kok FJ et al (2022) Perspective: Striking a Balance between Planetary and Human Health—Is There a Path Forward? Adv Nutr 13:355–375. https://doi.org/10.1093/advances/nmab139
Lassen AD, Christensen LM, Trolle E (2020) Development of a Danish Adapted Healthy Plant-Based Diet Based on the EAT-Lancet Reference Diet. Nutrients 12:738. https://doi.org/10.3390/nu12030738
Beal T, Ortenzi F, Fanzo J (2023) Estimated micronutrient shortfalls of the EAT–Lancet planetary health diet. Lancet Planet Health 7:e233–e237. https://doi.org/10.1016/S2542-5196(23)00006-2
VenegasHargous C, Orellana L, Strugnell C, Corvalan C, Allender S, Bell C (2023) Adapting the Planetary Health Diet Index for children and adolescents. Int J Behav Nutr Phys Act 20:146. https://doi.org/10.1186/s12966-023-01516-z
Passarelli S, Free CM, Allen LH, Batis C, Beal T, Biltoft-Jensen AP et al (2022) Estimating national and subnational nutrient intake distributions of global diets. Am J Clin Nutr 116:551–560. https://doi.org/10.1093/ajcn/nqac108
Stevens GA, Beal T, Mbuya MNN, Luo H, Neufeld LM, Addo OY et al (2022) Micronutrient deficiencies among preschool-aged children and women of reproductive age worldwide: a pooled analysis of individual-level data from population-representative surveys. Lancet Glob Health 10:e1590–e1599. https://doi.org/10.1016/S2214-109X(22)00367-9
Gong B, Wang C, Yang W, Shan Z (2024) Changing trends in the global, regional, and national burden of iodine deficiency among adolescents and young adults: population-based study. Eur J Pediatr 183:2855–2863. https://doi.org/10.1007/s00431-024-05545-z
Beal T, Gardner CD, Herrero M, Iannotti LL, Merbold L, Nordhagen S et al (2023) Friend or Foe? The Role of Animal-Source Foods in Healthy and Environmentally Sustainable Diets. J Nutr 153:409–425. https://doi.org/10.1016/j.tjnut.2022.10.016
Agencia Española de Consumo SA y N. Estudio ENALIA 2012–2014: Encuesta Nacional de consumo de Alimentos en población Infantil y Adolescente. Madrid; 2017. https://www.aesan.gob.es/AECOSAN/web/seguridad_alimentaria/subdetalle/enalia.htm. 2017.
Agencia Española de Consumo SA y N. Estudio ENALIA 2012–2014: Encuesta Nacional de consumo de Alimentos en población Infantil y Adolescente. Madrid; 2017.
Willett W (2012) Nutritional Epidemiology. Oxford University Press; 2012
Rothman KJ, Gallacher JE, Hatch EE (2013) Why representativeness should be avoided. Int J Epidemiol 42:1012–1014. https://doi.org/10.1093/ije/dys223
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Contributions
NMC, MAMG, IZ, EF: Conceptualization, Methodology and Software. EF: Data curation, writing of the original draft. NMC, IZ: Supervision. All authors critically reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Gregorio Milani
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fabios, E., Zazpe, I., Martínez-González, M.Á. et al. Association between provegetarian food patterns and micronutrient adequacy in preschoolers: the SENDO project. Eur J Pediatr (2024). https://doi.org/10.1007/s00431-024-05808-9
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00431-024-05808-9