
Abstract
This study assessed HRQoL and emotional and behavioral difficulties (EBD) and associated variables in children with first onset SSNS. While relapsing steroid-sensitive nephrotic syndrome (SSNS) in children is associated with lower health-related quality of life (HRQoL), little is known about first onset. Four weeks after onset, children (2–16 years) and/or their parents who participated in a randomized placebo-controlled trial, completed the Pediatric Quality of Life Inventory 4.0 (PedsQL) and Strengths and Difficulties Questionnaire (SDQ) to measure HRQoL and EBD, respectively. Total and subscale scores and the proportion of children with impaired HRQoL (> 1 SD below the mean of the reference group) or SDQ clinical scores (< 10th and > 90th percentile) were compared to the Dutch general population (reference group). Regression analyses were used to identify associated variables. Compared to the reference group, children 8–18 years reported significantly lower total HRQoL, and physical and emotional functioning. A large proportion (> 45%) of these children had impaired HRQoL. There were no differences in HRQoL between children 2–7 years and the reference group, except for higher scores on social functioning (5–7 years). Similar proportions of SSNS and reference children scored within the clinical range of SDQ subscales. Age, sex, and steroid side-effects were negatively associated with HRQol and/or EBD.
Conclusion: This study showed that HRQoL and EBD are affected in children of different ages with first onset SSNS. This calls for more awareness from healthcare providers and routinely monitoring of HRQoL and EBD in daily clinical care to prevent worsening of symptoms.
Clinical trial registry: Netherlands Trial Register (https://trialsearch.who.int/; NTR7013), date of registration: 02 June 2018.
What is Known: • Health-related quality of life (HRQoL) is lower and emotional and behavioral difficulties (EBD) is more affected in children with frequently-relapsing and steroid-dependent nephrotic syndrome. | |
What is New: • HRQoL and EBD are affected in children with first onset steroid-sensitive nephrotic syndrome compared to a reference group of the Dutch general population. • To what extent HRQoL and EBD are affected depends on the age of the patient. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
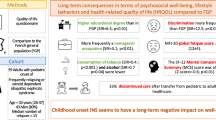
Idiopathic nephrotic syndrome (INS) is a rare glomerular disease in children that is characterized by the triad of profound edema, proteinuria, and hypoalbuminemia [1]. The first episode of INS is treated with a long course of high-dose corticosteroids [2,3,4,5], often leading to substantial side-effects, including Cushing symptoms, binge eating, hypertension, mood swings, and changed behavior [6]. Despite the good initial response – more than 85% of INS patients achieve complete remission (steroid-sensitive nephrotic syndrome (SSNS)) within 4 weeks of prednisolone – the risk for relapse is high: around 80% of children experience at least one relapse within 2 years after first onset [7,8,9]. Half of these patients experience multiple relapses per year (frequently relapsing nephrotic syndrome (FRNS)) or relapse during or shortly after steroid treatment (steroid-dependent nephrotic syndrome (SDNS)) [5].
Health-related quality of life (HRQoL) is the perception of one’s position in life when put in terms of physical symptoms, functional status, and disease impact on psychological and social functioning [10, 11], whereas psychosocial functioning is a person's ability to perform daily tasks and to interact with others and with society in a mutually satisfying manner [12, 13]. To measure HRQoL and psychosocial functioning focusing on emotional and behavioral difficulties (EBD), patient-reported outcome measures (PROMs, i.e. questionnaires) are used.
The relapsing–remitting behavior of SSNS and the marked side-effects of treatment negatively impact HRQoL in children with SSNS. Previous studies have shown that HRQoL in INS patients is lower compared to their peers [14,15,16,17], but better than in children with other chronic illnesses [18, 19]. However, these studies focused on relapsing SSNS (SDNS and/or FRNS). Studies about HRQoL and EBD in the first weeks of confirmed SSNS are lacking. Therefore, this study aims to determine the HRQoL and EBD and their association with sociodemographic and clinical variables of children between 2 and 16 years of age four weeks after onset of SSNS.
Methods
Study design
This is a prospective, cross-sectional, multicenter, observational study that is part of the LEARNS randomized, placebo-controlled trial studying the efficacy and safety of alternate day levamisole added to standard corticosteroid therapy to prevent relapses of SSNS [20]. Children were followed until 2 years after first onset. PROMs were collected at randomization before start of study medication (week 4), after discontinuation of study medication (week 28), at the primary endpoint (year 1), and at the end of the study (year 2). For this study, only the PROMs completed at week 4 were used for analysis to evaluate the effect of diagnosis and initial treatment at first onset on HRQoL and EBD.
PROMs were completed online using the KLIK PROM portal (www.hetklikt.nu); designed for monitoring patient outcomes in daily clinical practice and research [21]. After online registration, PROMs had to be completed within 14 days. After 7 days, participants received a reminder.
Study participants
Children (aged 2–16 years) with first onset SSNS were screened for eligibility. SSNS was defined as the presence of proteinuria (urinary protein-creatinine ratio (uPCR) > 200 mg/mmol creatinine), hypoalbuminemia (serum albumin < 25 g/L), and edema achieving complete remission (uPCR < 50 mg/mmol) within 4 weeks of standard prednisolone therapy [5, 20]. All subjects received an 18-week prednisolone tapering schedule [2].
Data collection and measures
Clinical data of the children were prospectively collected by trained clinicians using a standardized electronic case report form (Castor EDC), including age at onset (years), sex (male/female), cumulative prednisolone dose (mg/m2), time-to-remission (days), medical history of the past 4 weeks, school absence in the past 4 weeks, the presence of steroid side-effects (pre-specified: Cushingoid features, mood changes, binge eating, behavioral problems, hypertension, weight gain, skin abnormalities, and other), and concomitant medication use. Behavioral problems included aggression, bad attitude, anger, impatience, or change in and/or other problematic behavior according to parents.
Parents completed a survey on sociodemographics (age, sex, family situation, marital status, education). For Belgian children, versions appropriate for language (Flemish or French) were available. Two PROMs (Pediatric Quality of Life Inventory and Strengths and Difficulties Questionnaire) with appropriate versions for different age groups, were used to measure HRQoL and EBD.
Pediatric quality of life inventory (PedsQL) generic scale, version 4.0
The Dutch version of the PedsQL Generic Scale version 4.0 was used to measure HRQoL in children of different age categories (2–4 years, 5–7 years, 8–12 years, and 13–17 years) [22]. Children ≥ 8 years completed the PROM themselves (self-report). For children aged 2–7 years, we used proxy-report. The PedsQL consists of 21 (2–4 years) or 23 items (5–17 years) divided over four subscales: physical (n = 8), emotional (n = 5), social (n = 5), and school (n = 3/n = 5) functioning. Total HRQoL is the summary score of all subscales, while psychosocial functioning is that of emotional, social, and school functioning. Each item was scored on a 5-point Likert-scale. Items were reverse-scored and transformed to a 0–100 scale. Higher scores indicate better HRQoL. The PedsQL has a short completion time, and good feasibility, validity, and reliability [22, 23]. Reference data from the Dutch general population (n = 1286) are available and were stratified for key demographics, including age, sex, and education level, used as reference group [24, 25]. In our study, Cronbach’s alphas ranged between 0.64 and 0.93.
Strengths and difficulties questionnaire (SDQ)
The SDQ is a brief screening questionnaire developed for assessing EBD in children and adolescents [26]. Twenty-five items describe positive and negative attributes of children divided over 5 subscales (Emotional symptoms, Conduct problems, Hyperactivity-inattention, Peer problems, and Prosocial behavior). Items were scored on a 3-point scale and summed up to a 0–10 scale score. Higher scores on Prosocial behavior reflect strength, higher scores on all other scales reflect difficulties. The Total difficulties score is the sum of scales reflecting difficulties (range 0–40), the Internalizing problems score is the sum of Emotional symptoms and Conduct problems, and Externalizing problems is the sum of Hyperactivity-inattention and Peer problems (range 0–20). Scores > 90th (for difficulties) or < 10th (for Prosocial behavior) percentile are considered ‘clinical’ [26, 27]. The SDQ has both parent-reported (children 2–3 and 4–17 years old) and self-reported (11–17 years old) versions. The Dutch SDQ has acceptable to good psychometric properties [28]. Reference data for parent- and self-reported scores are available and were used as reference group [29, 30]. Due to low internal consistency within the reference data [29], scores for several subscales of the 2–3 and 4–5 years age groups were not presented. Cronbach’s alphas in our sample ranged between 0.32 and 0.94.
Statistical analysis
Continuous data were presented as the mean ± standard deviation (SD) or median (range), according to distribution. Normal distribution was tested using histograms and QQ-pots. Discrete data were presented as frequencies and proportions (%).
Total and subscale PedsQL scores were calculated for each age category. Differences between children with SSNS (SSNS group) and reference group were tested by an independent t test. The proportion (%) of children with impaired HRQoL, based on a score of ≥ 1 SD below the mean of the reference group, were compared by Fisher’s exact test. Individual items scores were presented as proportions (%). For each SDQ (summary) subscale, scores were calculated per age group. SDQ scores of the SSNS and reference group were compared using a one-sample t test. To quantify the differences, effect sizes (Cohen’s d) were calculated with 95% confidence intervals (CIs). Effect size was calculated as the difference in mean scores between the SSNS and reference group divided by the pooled SD. Effect sizes of 0.2, 0.5, and 0.8 were considered small, moderate, and large, respectively [31]. For each subscale of the PedsQL and the SDQ, the Cronbach’s alpha (α) was calculated. Scores of a scale with an α < 0.50 were not presented.
Multiple linear regression models were used to identify associated variables with PedsQL and SDQ scores. First, the following variables were tested by univariate analyses: child’s age and sex, older age ate onset (above median), parent’s country of birth (Netherlands/Belgium versus other) and educational level (low, intermediate, or high), time-to-remission, late remission (above median), illness in the past 4 weeks, school absence in the past 4 weeks, > 1 week of illness, > 1 week of school absence, the presence of any and pre-specified steroid side-effects (if present in ≥ 25% of the children), and the use and number of medications. Variables with a P < 0.05 in at least one of the scales were included simultaneously in the multiple linear regression model. Correlation between variables was tested for multicollinearity. A correlation of > 0.8 was considered too high, which was not the case for any of the variables. To express the association between variables and outcome, standardized regression coefficients (β) were reported. For continuous variables, β were considered small if 0.1, medium if 0.3, and large if 0.5, while for dichotomous variables, β were considered small if 0.2, medium if 0.5, and large if 0.8 [31].
Data were analyzed using IBM SPSS Statistics for Windows [32] and R Studio [33, 34]. A P < 0.05 was considered statistically significant.
Results
From April 25th, 2018 to December 10th, 2021, a total of 46 patients were included in the LEARNS study. Four weeks after first onset, 40 (87%) children and/or their parent(s) completed the PROMs. As a result of the design of the KLIK PROM portal (questions cannot be skipped), there were no missing data. Median age of the SSNS group was 6.3 (range 2.6–15.5) years. At least one side-effect of prednisolone was present in the majority of children (> 80%), binge eating (62.5%) and moon face (55.0%) being most prevalent. Table 1 shows the baseline characteristics.
Health-related quality of life
The results are shown in Table 2. No differences between the SSNS and reference group in age or sex were found in each age group. In children with SSNS aged 2–4 years, no significant differences in HRQoL scores were found, but moderate effect sizes were found in physical (d = 0.69, 95% CI 0.04–1.06) and school functioning (d = 0.73, 95% CI 0.22–1.24). Social functioning was significantly higher in children with SSNS aged 5–7 years compared to reference group (95.8 ± 6.7 vs. 86.4 ± 16.7, P < 0.001), with a moderate effect size d -0.57 (95% CI -1.13- -0.01). The HRQoL scores of children with SNSS aged 8–17 years were significantly lower compared to reference group on total (75.4 ± 14.4 vs. 84.9 ± 12.6, P = 0.013), physical (73.0 ± 20.8 vs. 91.6 ± 12.4, P = 0.014) and emotional functioning (63.6 ± 23.5 vs. 79.3 ± 18.4, P = 0.005) with moderate to large effect sizes (d ≥ 0.75).
Compared to the reference group, HRQoL was more often impaired in children aged 2–4 years on all subscales except social functioning (Fig. 1a). In children aged 5–7 years, psychosocial functioning was significantly less often impaired (0% vs. 17%) (Fig. 1b). A significantly larger proportion of children aged 8–17 years reported impaired total (46% vs. 15%), physical (55% vs. 13%) and emotional functioning (46% vs. 17%) compared to the reference group (Fig. 1c). On the individual items of the PedsQL, older children with SNSS reported to experience more pain, lower energy levels, trouble sleeping, feeling angry, and worrying than their peers (Online Resource I – Table S1c).

Proportions (%) of children with impaired HRQoL based a score of ≥ 1SD below the mean of the Dutch norm population for ages a 2–4 years (proxy-report), b 5–7 years (proxy-report), and c 8–17 years (self-report). * = P < 0.05; ** = P < 0.01
Emotional and behavioural difficulties
The results of the SDQ are presented in Online Resource I – Table S2. Compared to the reference group, more children with SSNS (2–17 years, parent-reported) scored within ‘clinical’ range (15.6 vs. 9.8%) of Emotional functioning (Fig. 2), but this difference was not significant. However, significantly lower mean scores on Conduct, Peer and Internalizing problems, and Total difficulties were reported by parents of 6–11-year-olds with SSNS, indicating fewer difficulties than their peers. They also scored higher on Prosocial behavior, indicating more strengths. Parents of children with SSNS aged 12–17 years (also proxy-report) indicated that their child had more Emotional symptoms, but better Prosocial behavior than the reference group (Online Resource I – Table S2).

Proportions (%) of children with clinical scores, defined as a score < 10th (strengths) or > 90th percentile (difficulties) of the mean score of Dutch norm population for all parent-reported age groups (2–17 years) combined (N = 39). None of the SSNS children had clinical scores for Conduct problems
Associated variables with HRQoL and psychosocial functioning
Age and time-to-remission were included in the multiple regression analysis of the PedsQL, while age, male sex, school absence, binge eating and behavioral problems were included in multiple regression analysis of the SDQ (Online Resource I – Table S3). Multiple regression identified that higher age (β = -0.34) was negatively associated with the emotional functioning subscale of the PedsQL (Table 3a). Higher age was also associated with better Prosocial behavior scale on the SDQ (β = 0.48). Boys reported more Peer problems on the SDQ (β = 0.32) than girls. When behavioral problems from steroids were present, parents reported higher Hyperactivity-inattention (β = -0.34) and Externalizing problems (β = 0.36) scores, while binge eating was associated with less Emotional symptoms on the SDQ (β = -0.34) (Table 3b).
Discussion
The results of this study show that at first onset of SSNS, HRQoL and EBD are already affected in children of different ages (2–16 years) compared to a reference group of the Dutch general population. However, not all age groups were equally affected. The effect was more profound in older children (≥ 8 years) than in younger children, with children aged 5–7 years scoring even better on social functioning.
Total HRQOL, physical and emotional functioning were significantly affected in children aged 8–17 years. Physical functioning can be impacted by limitations in daily activities, while mood disturbances – whether caused by steroids – can affect emotional functioning. More specifically, on the individual items, children with SNSS indicated that they experienced more pain, lower energy levels, and trouble sleeping (physical functioning), and feeling angry and worrying (emotional functioning) than their peers. Older children may be more aware of their condition than younger children, who scored comparable to their peers. Social functioning was not affected in any age group. Children 5–7 years scored even better on social functioning than reference and reported having fewer problems with getting along with peers or making friends. This could be explained by the fact that they may fare well by the attention received from family, friends, and schoolmates. Although children in our study have only been ill for four weeks, this is in line with previous studies, in which social functioning was also unaffected in children with a chronic illness [25, 35, 36].
This is the first study in children with first onset SSNS and in whom disease is in remission. Our findings are in line with those of Selewski et al. who reported that HRQoL – measured by PedsQL – in American children aged 8–17 years old with incident INS (i.e. first onset within 14 days of therapy) was worse than peers on physical, social, and total functioning [37]. To date, this had been the only HRQoL study in first onset SSNS. However, that study was conducted in children with active INS of 8 years or older only. In our study, children of all ages were studied using both proxy- and self-reported outcomes. Since SSNS predominantly affects children under the age of 6 years, our results fill this knowledge gap. Moreover, in our study, each child was in remission at PROM completion, but still receiving high doses of prednisolone. The poor scores on physical, social and total functioning could therefore be an effect of steroid treatment rather than of the disease itself.
Previous studies have found an association between the use and cumulative dose of steroids and HRQoL [38]. In children with relapsing SSNS, there is a wide variation in cumulative steroid dose and the use of steroid-sparing agents, which have been identified as independent predictors for negative outcome [39]. Disease duration [19, 37], the number of relapses [19], and disease severity [15, 16] have been identified as factors that negatively impact HRQoL in children with SSNS. As children in our study were at first onset having received similar doses of prednisolone, these factors could not be explored. Yet, as these children will be followed for two years after, systematically collected longitudinal HRQoL data will be available later. With this study, we provided a baseline score for children who are in remission.
At four weeks after onset, children are at their peak of steroid side-effects. While toxicity still continues after four weeks, study subjects were switched to alternate day prednisolone (60 mg/m2) at week 4 according to study protocol [2, 20], greatly relieving the steroid burden. We found that the presence of behavioral problems as reported by parents to the clinician were associated with more Hyperactivity-inattention and Externalizing problems. It is known that problematic externalizing behavior, such as aggression, violence, and restlessness, is more likely to be reported as it is visible behavior compared to internalizing behavior (anxiousness, depression, and refraining from social activities) which is an internal sense for the child. Surprisingly, binge eating was associated with fewer Emotional symptoms.
As Selewski et al. [37] demonstrated, HRQoL at first onset (incident INS) is worse than in the general population, but better than later in the disease course of SSNS (prevalent INS). Knowing more about the evolution of HRQoL and EBD over different courses of SSNS, could contribute to more patient-centered care. Monitoring and discussing HRQoL in daily clinical practice may aid clinicians with timely identifying lower HRQOL or more EBD and provide tailored interventions to prevent worsening of and/or improve symptoms. The KLIK PROM portal is a user-friendly and effective way to do so [40, 41].
This study was limited by small sample sizes per age group, which is secondary to the low incidence of SSNS. Due to a lack of power, differences that may be clinically relevant could have been missed. Therefore, we calculated effect sizes (Cohen’s d) which indeed showed moderate effects for the limited number of younger children. Also, a considerable number of variables have been tested for an association with outcome, increasing the chance of finding a false-positive result. Also, we acknowledge that HRQoL at 4 weeks after first onset may not be representative for the months following. For this reason, a long-term follow-up is currently ongoing. Last, HRQoL was only measured in children who participated in the LEARNS study, which may have biased the results and positively skewed the results.
On the other hand, this study is strengthened by the fact that this is the first study in children with first onset SSNS, adding new insights into the well-being of these children. The study consisted of a homogeneous population that spanned a wide age range (2–16 years), now including children in which SSNS is more incident. Furthermore, a high response rate was achieved (86%), which can be owed to the prospective study design, use of an online PROM portal, and a dedicated study team. Finally, recent Dutch reference data for both validated PedsQL and SDQ were available.
Conclusions
Impaired HRQoL was more profound in older children with first onset SSNS, in whom considerable proportions of impaired physical, emotional and total functioning were observed. Furthermore, this study showed that HRQoL and EBD are already affected in the first weeks after onset. Therefore, systematically monitoring of HRQoL and EBD by the use of PROMs should be encouraged to improve patient-centered care and timely identify signs of impaired HRQoL and EBD in children with first onset SSNS. Collection of longitudinal data of the first 2 years after onset is still ongoing and will provide additional insight into predictors of HRQoL outcomes eventually.
Data sharing statement
Deidentified individual participant data (including data dictionaries) will be made available, in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. Proposals should be submitted to the corresponding author.
Abbreviations
- CI:
-
Confidence interval
- EBD:
-
Emotional and behavioral difficulties
- FRNS:
-
Frequently-relapsing nephrotic syndrome
- HRQoL:
-
Health-related quality of life
- INS:
-
Idiopathic nephrotic syndrome
- PedsQL:
-
Pediatric Quality of Life Inventory 4.0
- PROM:
-
Patient-reported outcome measure
- SD:
-
Standard deviation
- SDNS:
-
Steroid-dependent nephrotic syndrome
- SDQ:
-
Strengths and Difficulties Questionnaire
- SSNS:
-
Steroid-sensitive nephrotic syndrome
- uPCR:
-
Urinary protein-creatinine ratio
References
Noone DG, Iijima K, Parekh R (2018) Idiopathic nephrotic syndrome in children. Lancet 392:61–74
Bérard É, Broyer M, Dehennault M, Dumas R, Eckart P, Fischbach M, Loirat C, Martinat L (2005) Syndrome néphrotique pur (ou néphrose) corticosensible de l’enfant: Protocole de traitement proposé par la Société de Néphrologie Pédiatrique. Nephrol Ther 1:150–156
Arbeitsgemeinschaft für Pädiatrische Nephrologie (1988) Short Versus Standard Prednisone Therapy for Initial Treatment of Idiopathic Nephrotic Syndrome in Children. Lancet 331:380–383
Tarshish P, Tobin JN, Bernstein J, Edelmann CM (1997) Prognostic significance of the early course of minimal change nephrotic syndrome: report of the International Study of Kidney Disease in Children. J Am Soc Nephrol 8:769–776
Rovin BH, Adler SG, Barratt J, Bridoux F, Burdge KA, Chan TM, Cook HT et al (2021) KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int 100:S1–S276
McDonough AK, Curtis JR, Saag KG (2008) The epidemiology of glucocorticoid-associated adverse events. Curr Opin Rheumatol 20:131–137
Teeninga N, Kist-van Holthe JE, van Rijswijk N, de Mos NI, Hop WCJ, Wetzels JFM, van der Heijden AJ, Nauta J (2013) Extending Prednisolone Treatment Does Not Reduce Relapses in Childhood Nephrotic Syndrome. J Am Soc Nephrol 24:149–159
Dossier C, Delbet JD, Boyer O, Daoud P, Mesples B, Pellegrino B, See H, Benoist G, Chace A, Larakeb A, Hogan J, Deschênes G (2019) Five-year outcome of children with idiopathic nephrotic syndrome: the NEPHROVIR population-based cohort study. Pediatr Nephrol 34:671–678
Webb NJA, Woolley RL, Lambe T, Frew E, Brettell EA, Barsoum EN, Trompeter RS, Cummins C, Wheatley K, Ives NJ (2019) Sixteen-week versus standard eight-week prednisolone therapy for childhood nephrotic syndrome: The PREDNOS RCT. Health Technol Assess 23:1–109
World Health Organization (1997) Division of Mental Health and Prevention of Substance Abuse WHOQOL: measuring quality of life. World Health Organization. https://apps.who.int/iris/handle/10665/63482
Haverman L, Limperg PF, Young NL, Grootenhuis MA, Klaassen RJ (2017) Paediatric health-related quality of life: what is it and why should we measure it? Arch Dis Child 102:393–400
Ro E, Clark LA (2009) Psychosocial functioning in the context of diagnosis: assessment and theoretical issues. Psychol Assess 21:313–324
Lam RW, Filteau MJ, Milev R (2011) Clinical effectiveness: the importance of psychosocial functioning outcomes. J Affect Disord 132(Suppl 1):S9–S13
Rahman M, Afroz S, Ali R, Hanif M (2016) Health Related Quality of Life in Children with Nephrotic Syndrome in Bangladesh. Mymensingh Med J 25:703–709
Rüth E-M, Landolt MA, Neuhaus TJ, Kemper MJ (2004) Health-related quality of life and psychosocial adjustment in steroid-sensitive nephrotic syndrome. J Pediatr 145:778–783
Roussel A, Delbet J-D, Micheland L, Deschênes G, Decramer S, Ulinski T (2019) Quality of life in children with severe forms of idiopathic nephrotic syndrome in stable remission - A cross-sectional study. Acta Paediatr 1–7(12):2267–2273
Selewski DT, Troost JP, Cummings D, Massengill SF, Gbadegesin RA, Greenbaum LA, Shatat IF, Cai Y, Kapur G, Hebert D, Somers MJ, Trachtman H, Pais P, Seifert ME, Goebel J, Sethna CB, Mahan JD, Gross HE, Herreshoff E, Liu Y, Carlozzi NE, Reeve BB, DeWalt DA, Gipson DS (2017) Responsiveness of the PROMIS® measures to changes in disease status among pediatric nephrotic syndrome patients: A Midwest pediatric nephrology consortium study. Health Qual Life Outcomes 15:166–166
Agrawal S, Krishnamurthy S, Naik B (2017) Assessment of quality of life in children with nephrotic syndrome at a teaching hospital in South India. Saudi J Kidney Dis Transplant 28:593–598
Eid R, Fathy AA, Hamdy N (2020) Health-related quality of life in Egyptian children with nephrotic syndrome. Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation 29:2185–2196
Veltkamp F, Khan DH, Reefman C, Veissi S, Van Oers HA, Levtchenko E, Mathôt RAA, Florquin S, Van Wijk JAE, Schreuder MF, Haverman L, Bouts AHM (2019) Prevention of relapses with levamisole as adjuvant therapy in children with a first episode of idiopathic nephrotic syndrome: Study protocol for a double blind, randomised placebo-controlled trial (the LEARNS study). BMJ Open 9:e027011–e027011
Haverman L, Engelen V, van Rossum MAJAJ, Heymans HSASA, Grootenhuis MA (2011) Monitoring health-related quality of life in paediatric practice: development of an innovative web-based application. BMC Pediatr 11:3–3
Varni JW, Seid M, Kurtin PS (2001) PedsQL™ 4.0: Reliability and Validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in Healthy and Patient Populations. Med Care 39:800–812
Engelen V, Haentjens MM, Detmar SB, Koopman HM, Grootenhuis MA (2009) Health related quality of life of Dutch children: psychometric properties of the PedsQL in the Netherlands. BMC Pediatr 9:68–68
Schepers SA, van Oers HA, Maurice-Stam H, Huisman J, Verhaak CM, Grootenhuis MA, Haverman L (2017) Health related quality of life in Dutch infants, toddlers, and young children. Health Qual Life Outcomes 15:1–8
Muilekom MMv, Luijten MAJ, Oers HAv, Conijn T, Maurice-Stam H, van Goudoever JB, Grootenhuis MA, Haverman L, Group obotKc (2021) Pediatric patients report lower Health-Related Quality of Life in daily clinical practice compared to new normative PedsQL data. Acta Paediatr 110:2267–2279
Goodman R (1997) The Strengths and Difficulties Questionnaire: A research note. J Child Psychol Psychiatry 38:581–586
Goodman R (2001) Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry 40:1337–1345
Van Widenfelt BM, Goedhart AW, Treffers PDA, Goodman R (2003) Dutch version of the Strengths and Difficulties Questionnaire (SDQ). Eur Child Adolesc Psychiatry 12:281–289
Maurice-Stam H, Haverman L, Splinter A, van Oers HA, Schepers SA, Grootenhuis MA (2018) Dutch norms for the Strengths and Difficulties Questionnaire (SDQ) - parent form for children aged 2–18 years. Health Qual Life Outcomes 16:1–11
Vugteveen J, de Bildt A, Timmerman ME (2022) Normative data for the self-reported and parent-reported Strengths and Difficulties Questionnaire (SDQ) for ages 12–17. Child Adolesc Psychiatry Ment Health 16:5
Cohen J (1992) A Power Primer Psychological Bulletin 112:155–159
IBM Corp (2021) IBM SPSS Statistics for Windows. IBM Corp., Armonk, New York
R Core Team (2020) R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria
Team R (2020) RStudio: Integrated Development for R. RStudio. RStudio, PBC, Boston, MA
Silva N, Pereira M, Otto C, Ravens-Sieberer U, Cristina Canavarro M, Bullinger M (2019) Do 8- to 18-year-old children/adolescents with chronic physical health conditions have worse health-related quality of life than their healthy peers? a meta-analysis of studies using the KIDSCREEN questionnaires. Qual Life Res 28:1725–1750
Pinquart M (2020) Health-related quality of life of young people with and without chronic conditions. J Pediatr Psychol 45:780–792
Selewski DT, Troost JP, Massengill SF, Gbadegesin RA, Greenbaum LA, Shatat IF, Cai Y, Kapur G, Hebert D, Somers MJ, Trachtman H, Pais P, Seifert ME, Goebel J, Sethna CB, Mahan JD, Gross HE, Herreshoff E, Liu Y, Song PX, Reeve BB, DeWalt DA, Gipson DS (2015) The impact of disease duration on quality of life in children with nephrotic syndrome: a Midwest Pediatric Nephrology Consortium study. Pediatr Nephrol 30:1467–1476
Khullar S, Banh T, Vasilevska-Ristovska J, Chanchlani R, Brooke J, Licht CPB, Reddon M, Radhakrishnan S, Piekut M, Langlois V, Aitken-Menezes K, Pearl RJ, Hebert D, Noone D, Parekh RS (2021) Impact of steroids and steroid-sparing agents on quality of life in children with nephrotic syndrome. Pediatr Nephrol 36:93–102
Troost JP, Gipson DS, Carlozzi NE, Reeve BB, Nachman PH, Gbadegesin R, Wang J, Modersitzki F, Massengill S, Mahan JD, Liu Y, Trachtman H, Herreshoff EG, DeWalt DA, Selewski DT (2019) Using PROMIS(R) to create clinically meaningful profiles of nephrotic syndrome patients. Health Psychol 38:410–421
Haverman L, Van Rossum MAJ, Van Veenendaal M, Van Den Berg JM, Dolman KM, Swart J, Kuijpers TW, Grootenhuis MA (2013) Effectiveness of a web-based application to monitor health-related quality of life. Pediatrics 131:e533–e543
Veltkamp F, Teela L, van Oers HA, Haverman L, Bouts AHM (2022) The Use of Patient-Reported Outcome Measures in Daily Clinical Practice of a Pediatric Nephrology Department. Int J Environ Res Public Health 19(9):5338
Acknowledgements
The authors like to thank all local investigators from the participating hospitals involved in the LEARNS study. The LEARNS study is an interuniversity collaboration in the Netherlands that is established to perform a double blind, placebo-controlled randomised clinical trial on the efficacy of levamisole on relapses in children with a first episode of steroid-sensitive nephrotic syndrome, and study basic mechanisms underlying the nephrotic syndrome and the mode of action of levamisole.
The LEARNS consortium study group
Principal investigators are (in alphabetical order): A.H.M. Bouts (Department of Pediatric Nephrology, Amsterdam UMC, location AMC, Amsterdam, the Netherlands), S. Florquin (Department of Pathology, Amsterdam UMC, location AMC, Amsterdam, the Netherlands), J.E. Guikema (Amsterdam UMC, location AMC, Amsterdam, the Netherlands), L. Haverman (Psychosocial Department, Amsterdam UMC, location AMC, Amsterdam, the Netherlands), L.P.W.J. van den Heuvel (Radboud Institute for Molecular Sciences, Radboud University Medical Center, Nijmegen, the Netherlands), E. Levtchenko (Department of Pediatric Nephrology, University Hospitals Leuven, Leuven, Belgium), R.A.A. Mathôt (Department of Hospital Pharmacy and Clinical Pharmacology, Amsterdam UMC, location AMC, Amsterdam, the Netherlands), M.F. Schreuder (Department of Pediatric Nephrology, Radboud University Medical Center, Nijmegen, the Netherlands), B. Smeets (Radboud Institute for Molecular Sciences, Radboud University Medical Center, Nijmegen, the Netherlands ), and J.A.E. van Wijk (Department of Pediatric Nephrology, Amsterdam UMC, location AMC, Amsterdam, the Netherlands).
Funding
The LEARNS study is funded by a consortium grant from the Dutch Kidney Foundation (CP16.03). Additional financial support was granted by Innovatiefonds Zorgverzekeraars and the Dr. C.J. Vaillant Fund.
Author information
Authors and Affiliations
Consortia
Contributions
In alphabetical order. Conceptualization: AB and LH. Study coordination: EM and FV. Patient selection: AB, EM, FV, and all local investigators affiliated to the LEARNS consortium. Data resource: LH, HvO, and LT. Data collection: EM and FV. Data analysis: ML, LT, and FV. Writing – original manuscript draft: FV. Writing – review and editing: AB, LH, ML, HvO, and LT. Supervision: AB and LH. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval
The LEARNS study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by an institutional review board (Netherlands: Amsterdam University Medical Centers, University of Amsterdam, 2017_301; Belgium: Onze Lieve Vrouwziekenhuis Aalst, 2019/042) and competent authorities of both countries.
Consent to participate
Written informed consent and/or assent (as appropriate) was obtained from the child (age ≥ 12 years) and legal representative(s).
Financial disclosure
All authors have no financial relationship relevant to this article to disclose.
Competing interest
The authors have no competing conflicts to disclose.
Additional information
Communicated by Peter de Winter
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Veltkamp, F., Teela, L., Luijten, M.A.J. et al. Health-related quality of life of children with first onset steroid-sensitive nephrotic syndrome. Eur J Pediatr 182, 4605–4614 (2023). https://doi.org/10.1007/s00431-023-05135-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-023-05135-5