
Abstract
Prescribing errors represent a safety risk for hospitalized patients, especially in pediatrics. Computerized physician order entry (CPOE) might reduce prescribing errors, although its effect has not yet been thoroughly studied on pediatric general wards. This study investigated the impact of a CPOE on prescribing errors in children on general wards at the University Children’s Hospital Zurich. We performed medication reviews on a total of 1000 patients before and after the implementation of a CPOE. The CPOE included limited clinical decision support (CDS) such as drug-drug interaction check and checks for duplicates. Prescribing errors, their type according to the PCNE classification, their severity (adapted NCC MERP index), as well as the interrater reliability (Cohen’s kappa), were analyzed. Potentially harmful errors were significantly reduced from 18 errors/100 prescriptions (95% CI: 17–20) to 11 errors/100 prescriptions (95% CI: 9–12) after CPOE implementation. A large number of errors with low potential for harm (e.g., “missing information”) was reduced after the introduction of the CPOE, and consequently, the overall severity of potential harm increased post-CPOE. Despite general error rate reduction, medication reconciliation problems (PCNE error 8), such as drugs prescribed on paper as well as electronically, significantly increased after the introduction of the CPOE. The most common pediatric prescribing errors, the dosing errors (PCNE errors 3), were not altered on a statistically significant level after the introduction of the CPOE. Interrater reliability showed moderate agreement (Κ = 0.48).
Conclusion: Patient safety increased by reducing the rate of prescribing errors after CPOE implementation. The reason for the observed increase in medication reconciliation problems might be the hybrid system with remaining paper prescriptions for special medication. The lacking effect on dosing errors could be explained by the fact that a web application CDS covering dosing recommendations (PEDeDose) was already in use before the implementation of the CPOE. Further investigations should focus on eliminating hybrid systems, interventions to increase the usability of the CPOE, and full integration of CDS tools such as automated dose checks into the CPOE.
What is Known: |
• Prescribing errors, especially dosing errors, are a common safety threat for pediatric inpatients. |
•The introduction of a CPOE may reduce prescribing errors, though pediatric general wards are poorly studied. |
What is New: |
•To our knowledge, this is the first study on prescribing errors in pediatric general wards in Switzerland investigating the impact of a CPOE. |
•We found that the overall error rate was significantly reduced after the implementation of the CPOE. The severity of potential harm was higher in the post-CPOE period, which implies that low-severity errors were substantially reduced after CPOE implementation. Dosing errors were not reduced, but missing information errors and drug selection errors were reduced. On the other hand, medication reconciliation problems increased. |
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Medication safety and the reduction of harm due to medication is an ongoing issue in health care. The WHO addresses this problem in the Third Global Patient Safety Challenge 2017, “Medication Without Harm.” [1] Pediatric patients are at particularly high risk of experiencing medication errors, notably prescribing errors [2,3,4,5]. A meta-analysis estimated a pooled rate of 17.5% of orders containing a prescribing error [6]. Neonatal intensive care units and pediatric intensive care units (PICU) have higher rates of prescribing errors [3]. A previous study by Glanzmann et al. [7] at the PICU in our hospital revealed an error rate of 14%. The situation in pediatric general wards is poorly studied [3].
Computerized physician order entry (CPOE) seems to reduce prescribing errors [8,9,10], and overall evidence suggests that mortality rates and preventable adverse drug events are reduced by electronic prescribing [10].
On pediatric general wards with CPOE prescribing, errors range from 14.8 to 47.0 errors/100 prescriptions, whereas paper charts show a range from 4.1 to 58.1 errors/100 prescriptions [3]. Dosing errors are common due to the great variability of weight and size among children [5, 10, 11]. In total, 2–6% of all orders for pediatric inpatients contain a dosing error [12].
In general, studies about medication errors show a great heterogeneity in definitions and methods [3, 8, 13]. To gain useful insights, clear definitions of the studied errors should be stated, validated error classifications applied, and—in addition to the prevalence of errors—severity of harm should be assessed [4, 9, 14, 15]. Chart review rather than voluntary reporting should be used as data source [3, 13], and interrater reliability should be calculated [13].
The aim of this study was to investigate the impact of the introduction of a CPOE on prescribing errors in children in pediatric general wards. We studied the prevalence, type, and severity of prescribing errors with retrospective chart review and validated our findings by calculating the interrater reliability.
Materials and methods
Setting and patients
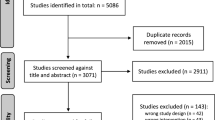
This retrospective observational study was conducted at the University Children’s Hospital Zurich, which is a tertiary care center and the largest pediatric hospital in Switzerland (220 beds). Eligible for the study were children up to 18 years who were hospitalized in 3 medical or 3 surgical wards. A total of 1000 patients, 500 from each study period, were randomly selected from 1688 (2018) and 1608 (2019) eligible patients, respectively, consisting of 250 medical and 250 surgical cases each. Patients with no prescribed medication (i.e., hospitalized for surveillance reasons) were not eligible. To control for seasonal effects, periods in identical months were included in the sampling frame: October until December 2018 (pre-CPOE) and October until December 2019 (post-CPOE).
CPOE
Until 2019 drugs were prescribed either manually on paper charts or electronically on semi-structured charts. CGM Clinical by CompuGroup Medical Inc. was used as a hospital information system. The pediatrics-specific CPOE tool by CompuGroup Medical Inc. was further developed from the preexisting CPOE tool for adults in cooperation with members of the University Children’s Hospital Zurich.
The drug master data were provided by HospINDEX (HCI Solutions Ltd.) and validated by the hospital pharmacy. Drugs from the hospital formulary were marked and provided with appropriate routes of administration so that only these routes of administration could be selected by the prescribing physician in the ordering process. In case of drug shortages, the appropriate substitute was proposed to the prescriber.
The CPOE contained some limited clinical decision support (CDS): an automated drug-drug interaction check and a duplication check based on the data of Pharmavista by HCI Solutions Ltd. [16], which was carried out every time a drug was prescribed.
In March 2019, the CPOE was implemented on all general wards. Implementation was accompanied by user education. Thereafter, most of the medication was prescribed electronically with the CPOE. There were some exceptions that could not be prescribed with the tool for technical reasons, such as patient-controlled analgesia and others, leading to hybrid drug prescription system to a small degree.
Information on drug dosing
Prescribers at the University Children’s Hospital Zurich had access to several guidelines and databases. They were requested to follow the dosing guidelines provided by the web application CDS by PEDeDose (PEDeus Ltd.), which was described by Higi et al. [17]. These dosing recommendations are based on the national harmonized dosing guidelines by Swisspeddose [18] and contain additional information. Aside from that, internal guidelines from different specialist fields with recommendations for certain disease patterns were available for all prescribers.
Prescriptions and medication review
A full medication review was conducted for all included patients, whereby the rater had access to all patient data. An adapted version of the medication appropriateness index [19] was used to guide the rater through the review process (Supplement 1).
All prescriptions within the first 24 h of admission to the ward were included. For patients who were hospitalized for elective surgery, prescriptions were included in the 24 h after surgery and return to the ward from PICU. Excluded medications were parenteral nutrition, lipids, any blood cell transfusions, insulin, solutions for dialysis, solutions for fluid management such as normal saline solution, dextrose 5%, dextrose 5% in normal saline solution, or acetated ringers. Electrolytes were included, even if they were added to parenteral nutrition.
Prescribing errors
As proposed by Dean et al. [20] the definition of a prescribing error was adopted as follows: “A clinically meaningful prescribing error occurs when, as a result of a prescribing decision or prescription writing process, there is an unintentional significant (1) reduction in the probability of treatment being timely and effective or (2) increase in the risk of harm when compared with generally accepted practice.”
Prescribing errors were classified into different types of errors according to the well-established PCNE Classification V 9.1, German Version [21, 22]. As pictured in Table 1, a subset of 7 primary domains from the PCNE Classification and 20 causes were used, which best matched the prescribing errors we found in our study. In the PCNE Classification, these causes are classified not only into the area of prescribing, but also into dispensing (PCNE 5), and patient transfer (PCNE 8). Nevertheless, we analyzed only drug prescriptions and no further steps in the medication process. A prescription could have more than one error, but a cause could only be recorded once per prescription. Supplement 2 displays how dosing errors were rated.
To increase the clinical relevance of our findings, we also included the severity of harm due to errors, even though the retrospective rating of the potential harm is likely to be more subjective than the rating of actual harm. [9, 15]. To determine the potential severity of the detected errors, we used the NCC MERP index as adapted by Forrey et al. [15, 23, 24] (see Table 2).
Interrater reliability
All patients were reviewed by the first rater (AS), and a random sample of 5% of all patients was additionally reviewed by a second rater (MP). Both raters were pharmacists with several years of experience in pediatric clinical pharmacy. A procedural manual was created to ensure that both raters approached the review in a similar way and that consistent data could be captured, as suggested by Vassar et al. [25]. Both raters decided on whether or not a prescription contained an error, which PCNE category the error belonged to, and what NCC MERP severity level it might have resulted in.
Database and statistical analysis
The study database was built with Microsoft SQL Server 2019 Master Data Services. The personal data from all included patients were automatically exported from the hospital information system into the database.
Statistical analyses were conducted with RStudio 2022.02.1 and IBM® SPSS® Statistics Version 27. The sample size of 1000 patients was estimated according to a previous study by Glanzmann et al. [7], with a reduction of prescribing errors from 14 to 9% based on a power of 0.8 and a one-sided test. Patient demographic data, rates of prescribing error, and severity of harm were compared by T-test, chi-square test, or Mann–Whitney test. Interrater reliability was calculated with Cohen’s kappa.
Results
Population
Pre-CPOE and post-CPOE patients did not differ in their demographic characteristics (Table 3), except for the length of stay. Post-CPOE patients stayed significantly longer on the ward (mean: 2.5 days) than pre-CPOE (mean: 2.1 days, p = 0.005, t-test).
Drug prescriptions
A total of 5022 drug prescriptions for 1000 patients were analyzed: 2299 drug prescriptions pre-CPOE and 2723 post-CPOE. Patients were prescribed more drugs post-CPOE than pre-CPOE (mean = 5.5 drugs vs. mean = 4.6 drugs, p < 0.001).
Handwritten prescriptions were significantly reduced by the CPOE (38.9% vs. 0.5%, p < 0.001).
Number of errors overall
A total of 2485 errors for all prescriptions was found, of which 1802 errors occurred pre-CPOE and 683 errors post-CPOE. Consequently, 78.4 errors per 100 prescriptions (95% CI: 76.2–80.6) were found before the introduction of the CPOE vs. 25.1 errors per 100 prescriptions (95% CI: 23.0–27.1) after introduction of the CPOE (p < 0.001, t-test). This means that 69.2% (95% CI: 67.4–71.0) of all prescriptions pre-CPOE contained at least one error vs. only 22.8% (95% CI: 21.2–24.5) of all prescriptions post-CPOE, which implies a significant reduction of errors (p < 0.001). In 100 admissions, 360 errors could be found pre-CPOE vs. 137 in post-CPOE (p < 0.001).
The most frequent type of error (80.6% of all errors pre-CPOE and 44.7% of all errors post-CPOE) was in PCNE primary domain 5 (dispensing) (Table 4). More precisely, 79.5% of all errors pre-CPOE and 44.1% of all errors post-CPOE were type 5.2 errors: “Necessary information not provided or incorrect advice provided.” Examples of this type of error pre-CPOE are: “Missing or incorrect information about the route of administration,” “active ingredient missing,” (only product name prescribed) or “drug form missing.” Post-CPOE, the most frequent error 5.2 was due to the additional selection of a mode of administration, like buccal or lingual, where it was not appropriate. Most of these errors 5.2 were of minor severity (NCC MERP severity grades A–D). Some of the 5.2 errors, though were rated as “temporary harm possible,” such as analgesic prescriptions in reserve with a frequency but no maximum number of doses prescribed.
Severity of harm due to errors
The overall severity of harm increased significantly after the introduction of the CPOE. Mean rank pre-CPOE was 1175 vs. 1423 post-CPOE (p = 0.000, Mann–Whitney test).
Overall, the majority of the documented errors were of minor severity (NCC MERP A–D): 76.4% pre-CPOE and 58% post-CPOE (Table 5). These errors with minor severity are unlikely to result in any harm for the patient (see the “Prescribing errors” section [20]). Therefore, we decided to focus on errors with severity E–I that might have resulted in potential harm.
Numbers of errors causing potential harm (NCC MERP E-I)
After exclusion of errors with severity A–D, we counted a remaining total of 711 errors with potential severity of harm, E–I, which were 424 errors pre-CPOE and 287 errors post-CPOE. The overall error rate of 18.4 errors/100 prescriptions (95% CI: 16.8–19.9) before CPOE was reduced to 10.5 errors/100 prescriptions (95% CI: 9.1–12.0) after introduction of the CPOE, which was a significant reduction of the error rate (p < 0.001). Therefore, 16.8% of all prescriptions before CPOE contained at least one error (95% CI: 15.5–18.2), whereas the error rate after CPOE was only 9.8% (95% CI: 8.6–11.1) (p < 0.001). The rate of errors per 100 admissions was significantly reduced from 84 errors/100 admissions pre-CPOE to 57 errors/100 admissions post-CPOE (p = 0.001).
Type of errors causing potential harm (NCC MERP E-I)
As Table 6 shows, the most frequent primary domain of errors causing potential harm pre-CPOE was domain 5 (dispensing), while post-CPOE the most frequent was domain 3 (dosing errors). Type 5 errors decreased significantly from 8.7 errors/100 prescriptions to 1.9 errors/100 prescriptions (p < 0.001), and type 1 errors (drug selection) decreased from 3.0 to 2.0 errors/100 prescriptions (p = 0.031).
The third domain that showed a significant change from pre- to post-CPOE was PCNE 8 “patient transfer related.” These errors increased significantly from 0.2 errors/100 prescriptions to 0.6 errors/100 prescriptions (p = 0.010). Type 8 errors were coded when two valid prescriptions for the same patient and time were found in different media, e.g., one CPOE prescription and one prescription on a paper chart. The doubled prescriptions contained, in some cases, the same information but sometimes slightly different dosages or instructions.
There were no statistically significant differences from pre- to post-CPOE in the other primary domains. In particular, dosing errors (type 3) showed no significant change (pre-CPOE: 5.6 errors/100 prescriptions, post-CPOE: 5.2 errors/100 prescriptions, p = 0.555). The PCNE causes are also displayed in Table 6.
Handwritten vs. electronically written prescriptions causing potential harm
Pre-CPOE, we compared the error rates in handwritten and electronically written prescriptions. Handwritten prescriptions showed a significantly higher rate of errors (22.6 errors/100 prescriptions) than electronically written prescriptions (15.7 errors/100 prescriptions) (p < 0.001). A total of 20.9% of handwritten prescriptions contained at least one error, while only 14.2% of electronically written orders contained an error.
Interrater reliability
Cohen’s Kappa for the agreement on whether or not an error occurred in a prescription was 0.476. This implies a moderate interrater agreement [26]. The agreement on primary domains and causes showed perfect agreement with k = 1.000, but for severity of harm, a kappa of only 0.158 (slight agreement) was calculated.
Discussion
After the implementation of the CPOE, patients were prescribed more drugs than before (5.5 vs. 4.6). The fact that many adjustments to a CPOE prescription, such as an adaption of the dose, resulted in a new prescription line may have influenced this finding.
The overall error rate decreased significantly after implementation of the CPOE. This finding complies with the results of a recent systematic review in pediatrics by Koeck et al. [9], indicating that CPOE reduces prescribing errors.
The rate of potentially harmful errors (NCC MERP E-I) of 18.4% (95% CI 16.8–19.9) before introduction of the CPOE was higher than the error rate of 14%. Glanzmann et al. [7] found 9 years ago in our PICU, where a semi-structured order sheet was in use. Usually, error rates in PICUs are higher than those in general wards. One explanation for the higher error rate in our study might be that the PICU had a clinical pharmacist on rounds once or twice per week for years, while the general wards were not visited by a clinical pharmacist, except for one medical ward with irregular visits once per week at maximum. Besides that, the study of Glanzmann et al. was prospective, where uncertainties about the prescription could be clarified by direct discussion with the prescriber, whereas we conducted a retrospective study.
The CPOE especially improves the quality of prescriptions, which can be seen in the largest reduction of potentially harmful errors (NCC MERP E-I) in PCNE errors 5.2 (“lacking or wrong information”) from 8.7 to 1.9 errors/100 prescriptions (p < 0.001). This is consistent with the findings of Jungreithmayr et al. [27], who showed that a CPOE increased the quality of the prescription documentation.
Drug selection errors (PCNE 1) and especially cause 1.4 “inappropriate duplication of therapeutic group or active ingredient” were significantly reduced post-CPOE. This could be contributed to the duplication-check CDS.
Interestingly, cause 1.3 concerning drug-drug interactions did not decrease, even though one CDS tool (Pharmavista) offered an automatic drug-drug interaction check. This could be attributed to either alert fatigue [29] or poor usability of the integrated tool [30].
Nevertheless, a new hybrid-systems-related error did occur, as medication reconciliation problems (PCNE 8) increased significantly with remaining paper prescriptions for special medication. This type of error might be prevented through the integration of all prescriptions into the CPOE and the complete elimination of prescriptions on paper.
The CPOE had no effect on dosing errors. This finding might be explained by the fact that the web application CDS covering dosing recommendations (PEDeDose) was already in use before implementation of the CPOE, and there was no automated dose check to validate the prescriptions. The lacking effect of CPOE on dosing errors was also seen by Roumeliotis et al. [28]. Dosing errors could be prevented more effectively by a fully integrated CDS that offers dosing support and automated dose check [31].
The fact that handwritten prescriptions contained more errors than electronic prescriptions is a plausible finding, as CPOE leads to standardized, legible, and complete prescriptions [32].
The errors that occurred post-CPOE were more severe than pre-CPOE. This implies that a large number of minor-severity errors like “missing information” (PNCE 5.2) and others no longer occurred after the introduction of the CPOE. It also indicates that the introduction of the CPOE was not able to reduce the severity of harm but only the rate of errors.
Limitations
Due to the retrospective nature of our study, we had to interpret previously recorded data on patients’ history and their prescriptions. This could have led to the conclusion that an error had occurred, although there was a plausible reason for the deviation from the norm, which was however not recorded in the patient’s charts. For this reason, the retrospective nature of our study imposes a limitation not only on the rate of errors but especially on the interpretation of the severity of harm.
Furthermore, not optimal interrater reliability imposes another limitation to our study. Even though a procedure manual existed, there was only limited training and coordination between the two raters. One rater might have tried to capture errors comprehensively, whereas the other had a more pragmatic way of assessment of the prescriptions. Rater 1 reviewed all 1000 patients and therefore had more routine in the procedure, while rater 2 only reviewed 50 patients.
Conclusion
In conclusion, our findings imply a positive impact of the CPOE on patient safety by reducing the prevalence of prescribing errors. Especially the high number of errors with low harming potential (NCC MERP A–D) was reduced, but also potentially harmful errors were significantly reduced.
Hybrid systems of CPOE and paper charts carry a risk for errors and should therefore be eliminated. Future research might focus on interventions to increase the usability of the CPOE and on the full integration of CDS tools, for example, dosing support and notably automated dose check into the CPOE.
Data Availability
The datasets generated and analysed during the current study are not publicly available due to sensitivity.
Abbreviations
- CDS:
-
Clinical decision support
- CI:
-
Confidence interval
- CPOE:
-
Computerized physician order entry
- PCNE:
-
Pharmaceutical Care Network Europe
- PICU:
-
Pediatric intensive care unit
References
Donaldson LJ, Kelley ET, Dhingra-Kumar N, Kieny M-P, Sheikh A (2017) Medication without harm: WHO’s third global patient safety challenge. Lancet 389:1680–1681. https://doi.org/10.1016/S0140-6736(17)31047-4
Kaushal R, Bates DW, Landrigan C, McKenna KJ, Clapp MD, Federico F, Goldmann DA (2001) Medication errors and adverse drug events in pediatric inpatients. JAMA 285:2114–2120
Gates PJ, Baysari MT, Gazarian M, Raban MZ, Meyerson S, Westbrook JI (2019) Prevalence of medication errors among paediatric inpatients: systematic review and meta-analysis. Drug Saf 42:1329–1342. https://doi.org/10.1007/s40264-019-00850-1
Ghaleb MA, Barber N, Franklin BD, Wong ICK (2010) The incidence and nature of prescribing and medication administration errors in paediatric inpatients. Arch Dis Child 95:113–118. https://doi.org/10.1136/adc.2009.158485
Conn RL, Kearney O, Tully M, Shields M, Dornan T (2019) What causes prescribing errors in children? Scoping review. BMJ Open 9
Koumpagioti D, Varounis C, Kletsiou E, Nteli C, Matziou V (2014) Evaluation of the medication process in pediatric patients: a meta-analysis. J Pediatr (Rio J) 90:344–355. https://doi.org/10.1016/j.jped.2014.01.008
Glanzmann C, Frey B, Meier CR, Vonbach P (2015) Analysis of medication prescribing errors in critically ill children. Eur J Pediatr. https://doi.org/10.1007/s00431-015-2542-4
Gates PJ, Hardie RA, Raban MZ, Li L, Westbrook JI (2021) How effective are electronic medication systems in reducing medication error rates and associated harm among hospital inpatients? A systematic review and meta-analysis. J Am Med Inform Assoc 28:167–176. https://doi.org/10.1093/jamia/ocaa230
Koeck JA, Young NJ, Kontny U, Orlikowsky T, Bassler D, Eisert A (2021) Interventions to reduce pediatric prescribing errors in professional healthcare settings: a systematic review of the last decade. Paediatr Drugs 23:223–240. https://doi.org/10.1007/s40272-021-00450-6
Sutcliffe K, Stokes G, O Mara A, Caird J, Hinds K, Bangpan M, Kavanagh J, Dickson K, Stansfield C, Hargreaves K, Thomas J (2014) Paediatric medication error: a systematic review of the extent and nature of the problem in the UK and international interventions to address it
Lehmann CU (2015) Pediatric aspects of inpatient health information technology systems. Pediatrics 135:e756-768. https://doi.org/10.1542/peds.2014-4148
Gates PJ, Meyerson SA, Baysari MT, Westbrook JI (2019) The prevalence of dose errors among paediatric patients in hospital wards with and without health information technology: a systematic review and meta-analysis. Drug Saf 42:13–25. https://doi.org/10.1007/s40264-018-0715-6
Maaskant JM, Vermeulen H, Apampa B, Fernando B, Ghaleb MA, Neubert A, Thayyil S, Soe A (2015) Interventions for reducing medication errors in children in hospital. Cochrane Database Syst Rev Cd006208. https://doi.org/10.1002/14651858.CD006208.pub3
Gates PJ, Meyerson SA, Baysari MT, Lehmann CU, Westbrook JI (2018) Preventable adverse drug events among inpatients: a systematic review. Pediatrics 142 https://doi.org/10.1542/peds.2018-0805
Garfield S, Reynolds M, Dermont L, Franklin BD (2013) Measuring the severity of prescribing errors: a systematic review. Drug Saf 36:1151–1157. https://doi.org/10.1007/s40264-013-0092-0
Solutions H (2022) www.pharmavista.ch
Higi L, Käser K, Wälti M, Grotzer M, Vonbach P (2021) Description of a clinical decision support tool with integrated dose calculator for paediatrics. Eur J Pediatr. https://doi.org/10.1007/s00431-021-04261-2
Tilen R, Panis D, Aeschbacher S, Sabine T, Schwabedissen MZ, HE, Berger C (2022) Development of the Swiss Database for dosing medicinal products in pediatrics. Eur J Pediatr 181:1221–1231. https://doi.org/10.1007/s00431-021-04304-8
Hanlon JT, Schmader KE, Samsa GP, Weinberger M, Uttech KM, Lewis IK, Cohen HJ, Feussner JR (1992) A method for assessing drug therapy appropriateness. J Clin Epidemiol 45:1045–1051. https://doi.org/10.1016/0895-4356(92)90144-c
Dean B, Barber N, Schachter M (2000) What is a prescribing error? Qual Health Care 9:232–237
Schindler E, Richling I, Rose O (2021) Pharmaceutical Care Network Europe (PCNE) drug-related problem classification version 9.00: German translation and validation. Int J Clin Pharm 43:726–730. https://doi.org/10.1007/s11096-020-01150-w
Association PCNE (2020) The PCNE classification V 9.1. Pharmaceutical Care Network Europe, p Classification for Drug related problems
Forrey RA, Pedersen CA, Schneider PJ (2007) Interrater agreement with a standard scheme for classifying medication errors. Am J Health Syst Pharm 64:8. https://doi.org/10.2146/ajhp060109
Prevention NCCfMERa (2001) NCC MERP index for categorizing medication errors
Vassar M, Holzmann M (2013) The retrospective chart review: important methodological considerations. J Educ Eval Health Prof 10:12. https://doi.org/10.3352/jeehp.2013.10.12
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Jungreithmayr V, Meid AD, Haefeli WE, Seidling HM (2021) The impact of a computerized physician order entry system implementation on 20 different criteria of medication documentation-a before-and-after study. BMC Med Inform Decis Mak 21:279. https://doi.org/10.1186/s12911-021-01607-6
Roumeliotis N, Sniderman J, Adams-Webber T, Addo N, Anand V, Rochon P, Taddio A, Parshuram C (2019) Effect of electronic prescribing strategies on medication error and harm in hospital: a systematic review and meta-analysis. J Gen Intern Med 34:2210–2223. https://doi.org/10.1007/s11606-019-05236-8
Carli D, Fahrni G, Bonnabry P, Lovis C (2018) Quality of decision support in computerized provider order entry: systematic literature review. JMIR Med Inform 6:e3. https://doi.org/10.2196/medinform.7170
Sutton RT, Pincock D, Baumgart DC, Sadowski DC, Fedorak RN, Kroeker KI (2020) An overview of clinical decision support systems: benefits, risks, and strategies for success. NPJ Digit Med 3:17. https://doi.org/10.1038/s41746-020-0221-y
Hashemi F, van Gelder TG, Bollen CW, Liem YTB, Egberts TCG (2022) The effect of a decision support system on the incidence of prescription errors in a PICU. J Clin Pharm Ther 47:330–344. https://doi.org/10.1111/jcpt.13562
Maat B, Au YS, Bollen CW, van Vught AJ, Egberts TC, Rademaker CM (2013) Clinical pharmacy interventions in paediatric electronic prescriptions. Arch Dis Child 98:222–227. https://doi.org/10.1136/archdischild-2012-302817
Acknowledgements
This work would not have been possible without the financial support of the GSASA and the University Children’s Hospital Zurich. We would like to express our sincere gratitude to Priska Vonbach from PEDeus Ltd. for the first concept of the study and for acquiring the GSASA grant. Furthermore, we thank Beat Bangerter from the University Children’s Hospital Zurich for his tireless technical support in the creation and use of the database.
Funding
Open access funding provided by University of Zurich. This work was funded by the grant for the scientific project of national reach 2014 of the Swiss Association of Public Health Administration and Hospital Pharmacists (GSASA).
Author information
Authors and Affiliations
Contributions
Principal investigator and supervision of the thesis of AS: AC; conception, design, and methods: AC and AS; data collection: AS; medication review: AS and MP; data analysis and initial manuscript: AS; review, editing, and final approval of the manuscript: AC, AS, MP, and CM.
Corresponding author
Ethics declarations
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Zurich (PB_2019-00030, project related to subsequent use of non-genetic personal health data). All included patients gave informed consent for further use of their health-related data.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Satir, A.N., Pfiffner, M., Meier, C.R. et al. Prescribing errors in children: what is the impact of a computerized physician order entry?. Eur J Pediatr 182, 2567–2575 (2023). https://doi.org/10.1007/s00431-023-04894-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-023-04894-5