
Abstract
Most children with functional constipation (FC) improve with conventional treatments. However, a proportion of children have poor treatment outcomes. Management of intractable FC may include botulinum toxin injections, transanal irrigation, antegrade enemas, colonic resections, and in some cases sacral nerve stimulation (SNS). SNS is surgically placed, not readily available and expensive. Posterior tibial nerve stimulation (PTNS) allows transmission of electronic impulses and retrograde stimulation to the sacral nerve plexus in a portable, simple and non-invasive fashion. To assess the efficacy and safety of transcutaneous PTNS for the treatment of FC in children. Single-center, prospective interventional study. Children 4–14 years with Rome IV diagnosis of FC received ten daily PTNS (30 min/day) sessions. Electrodes placed over skin of ankle. Strength of stimulus was below pain threshold. Outcomes were assessed during treatment and 7 days after. Twenty-three subjects enrolled. Two children excluded (acute gastroenteritis, COVID-19 contact). Twenty completed the study (4–14 years), (8.4 ± 3.2 years, 71.4% female). We found significant improvement in the consistency of bowel movements (BM) (p = 0.005), fecal incontinence (FI) (p = 0.005), abdominal pain presence (p = < 0.001) and intensity (p = 0.005), and a significant for improvement in blood in stools (p = 0.037). There was 86.3% improvement in abdominal pain. 96.7% reported treatment satisfaction. Only one child required rescue therapy.
Conclusion: We found significant improvement in stool consistency, FI, abdominal pain, and hematochezia. This suggests that transcutaneous PTNS could be a promising noninvasive treatment for FC in children. Large studies are needed.
What is Known: • Functional constipation is one of the most common disorders in children. • Current management of functional constipation consists of an integrative approach that includes medications, diet and behavioral strategies. | |
What is New: • Posterior tibial nerve stimulation is a novel noninvasive and easy to use therapy that can improve stool consistency, fecal incontinence and blood in stools. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Functional Constipation (FC) represents one of the most common disorders in children worldwide with a pooled prevalence of 9.5% [1]. FC is characterized by delayed or infrequent passage of dry, hardened and painful stools that may be accompanied by abdominal pain and/or fecal incontinence (FI) [2, 3]. Constipation is a major cause of school absenteeism, social isolation, and poor quality of life, particularly in cases associated with FI [4]. Current management of FC consists of an integrative approach that includes medications, diet and behavioral strategies. While the vast majority of patients with FC respond to conventional treatments [5], approximately 20% of children continue to suffer of long-term constipation. This group of patients are considered to have intractable constipation [6, 7]. Management of intractable constipation may include medications, antegrade enemas, transanal irrigations and in some cases sacral nerve stimulation (SNS) [8, 9]. SNS involves electric stimulation of the sacral nerve root (S2–S3) by a permanently implanted lead connected to a pulse generator battery. Although, the mechanism of action of SNS in the treatment of FC is not fully elucidated [10], it is thought to modulate the function of the bowel, bladder, and/or pelvic floor through direct modulation of sacral nerve activity. Several studies have shown that SNS can lead to improvement in symptoms and quality of life in children with constipation [6, 11]. However, SNS is only available in few centers, is expensive, surgically implanted and not devoid of complications [9, 12]. Therefore, it would be of importance to find an alternative therapeutic approach.
The posterior tibial nerve is a distal branch of the sciatic nerve (from sacral nerve plexus L4–S3). Similar to SNS, posterior tibial nerve stimulation (PTNS) can modulate anorectal neuromuscular function [13, 14] through depolarization and retrograde stimulation of the lumbar and sacral afferent somatic fibers. An advantage of PTNS is that it allows transcutaneous neuromodulation of the sacral nerve in a non-surgical fashion via adhesive electrodes placed over the skin of the ankle. Thus, PTNS is easy to apply, non-invasive, does not require anesthesia and is less costly than SNS. Transcutaneous PTNS has been used in children with refractory overactive bladder and in adults with chronic anal fissure and FI with a favorable response [14, 15]. However, there are no published studies to assess the efficacy of transcutaneous PTNS in children with FC.
The primary objective of this clinical trial is to assess the efficacy and safety of transcutaneous PTNS in children with FC. Secondary objectives are to evaluate treatment satisfaction. We hypothesized that the transcutaneous application of PTNS would be efficacious, safe, and well accepted.
Methods
Study design
We conducted a single-center prospective interventional study from January 7th to June 30th, 2020, in children that consulted the pediatric outpatient clinic of the Mario Correa Rengifo General Hospital of Cali, Colombia for FC.
Study population
Inclusion criteria
Children between 4 and 14 years with a diagnosis of FC per the Rome IV Criteria. Ability to complete daily diaries and PTNS sessions.
Exclusion criteria
Children that received treatment for FC 15 days prior to the study, had urinary incontinence, neurological problems (cerebral palsy, epilepsy, psychomotor retardation, language, or auditory cognitive impairment), documented neuropathies, congenital gastrointestinal or anorectal abnormalities, history of anorectal surgeries or skin allergic reactions.
We obtained written informed consent from participant’s parents and assent from children aged > 7 years. This study was approved by the Institutional Review Board of Mario Correa Rengifo General Hospital of Cali, Colombia (Resolution 8430 of the Colombian Ministry of Health, approval SDCI-2.0–11-02–183).
Measurements and procedures
At baseline, children underwent a medical visit which included data collection and physical exam. All children received 30-min daily sessions of transcutaneous PTNS for 10 days over a 2-week period resting weekends. Children who were not able to attend the clinic daily, were visited at home by a trained member of the research team that applied the treatment at home. For PTNS, negative electrodes were placed over the skin of the ankle posteriorly to the internal or medial malleolus and the positive electrodes above the negative electrodes. The exact placement and location of the electrodes was individually adjusted according to size. Confirmation of the correct placement of electrodes on the anatomic route of the posterior tibial nerve with visualization of rhythmic flexion of hallux during the initial stimulation was performed prior to each application. Children that had no BM for three consecutive days were considered treatment failures. These children received rescue therapy and had their PTNS treatment discontinued. They were included in the analysis as failures.
Transcutaneous PTNS
PTNS was conducted through the Biomedâ 2000 XL, a small (3.9″L × 2.75″W × 1″H) and portable transcutaneous electrical nerve stimulation (TENS) unit powered by a 9-V battery. The strength of the stimulus was set just below the pain threshold, enough to produce a tingling sensation without any muscle contraction. The frequency of the stimulation (pulses per second) was set at 10 Hz with the width (duration) of the pulse set at 200 µs. Settings were adjusted prior to each session.
Outcomes
Primary outcome–improvement in criteria of FC. Evaluation of safety.
Secondary outcome–satisfaction with treatment.
Data collection and instruments
Patients recorded the presence and characteristics of their bowel movements (BM) in a daily diary using the Bristol Stool Scale for the 10 days of transcutaneous PTNS and the following 7 days. Stool consistencies were categorized as per the Bristol Scale; Normal Stool were type 3 and type 4 and Hard stools type 1 and type 2. Satisfaction with treatment was assessed through a standardized questionnaire at day 17 (3-point scale: not-satisfied, neutral, and satisfied).
Statistical analysis
Mean, median, standard deviation, and interquartile ranges were calculated. The number of BMs and FC symptoms before and during treatment were compared with t-test analysis for independent samples. The statistical analysis was performed utilizing the STATA 15 program and the values were considered statistically significant when p value was < 0.05.
Results
We recruited twenty-three children with the diagnosis of FC according to the Rome IV criteria. Eleven children were treated outpatient and ten children in the home setting. All of them provided daily data throughout the trial and follow-up data on day seventeen. Two children were excluded: one child for COVID-19 exposure and another child for acute gastroenteritis. For the analysis of the results, we included the 21 patients that received treatment (Fig. 1), mean age of 8.4 ± 3.2 years. There were fifteen female (71.4%) and six males (28.6%). Children had mean duration of constipation of 5.3 ± 3.5 months.

Flow diagram of participants’ enrollment
One child failed treatment due to no depositions over a 3-day period on day six of PTNS and required rescue therapy. Out of the twenty remaining children all had clinical improvement in at least one of the presenting symptoms. No children worsened any of the presenting symptoms during the 10 days of the trial or at follow-up. At the end of the trial only two out of the twenty patients remained with FI that resolved by day seventeen and one patient remained with abdominal pain throughout the trial and follow-up. All other patients resolved their symptoms. There was no significant difference between children treated in the clinic and at home.
Stool characteristics
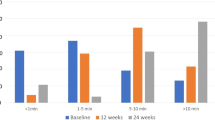
There were significantly more children with normal stools at the end of day ten and follow-up. There was a significant improvement in consistency of BMs at the end of the trial and at follow-up (Table 1 and Fig. 2). On day 1, 76.2% of patients had hard stools (Bristol Scale type 1, 2) while 30% of children had hard stools on day 10 and 25% had hard stools at 7-day follow-up. There was no significant improvement in frequency of BMs at the end of the trial or at follow-up. There was a significant improvement in blood in the stools. By the end of the trial, no children had blood in the stools (from 19% on day 1). This was sustained at 7-day follow-up.

Evolution from baseline in stool consistency (dotted line) abdominal pain (solid black line), FI (solid gray line) blood in stools (dashed line) in patients that received transcutaneous PTNS. Time course of comparison shown in days (X axis), number of patients (Y axis). Vertical dashed line represents day 10, completion of treatment and beginning of follow-up
Fecal incontinence
We found a trend for improvement in FI at the end of the 10 days of treatment and a significant improvement by day seventeen. Two out of seven children had episodes of FI on day ten and no children had FI on day 17 (Table 1).
Abdominal pain
There was a significant improvement in presence of abdominal pain. At day 1, 71.4% of children reported abdominal pain compared with 30% of children at day 10 and 4.7% at day 17 (Table 1 and Fig. 2). The intensity of abdominal pain (numeric rating scale of 1–10) was significantly reduced by day seventeen but the improvement was not statistically significant by day 10 (Table 1 and Fig. 3).

Changes from baseline of intensity in abdominal pain (measured in a scale from 1 to 10) in patients that received transcutaneous PTNS. Time course of comparison shown in days (Y axis), intensity of abdominal pain (X axis). Dashed line represents Day 10, completion of treatment and beginning of follow-up
Safety
Two children reported leg cramps that resolved by changing the side of PTNS application.
Satisfaction with treatment
There was 96.7% overall treatment satisfaction. All children reported that they would repeat the treatment if needed, 95% would recommend the therapy and 95% reported that the treatment fulfilled their expectations.
Follow up period
No child worsened any of the presenting features in the interval between day ten and day seventeen. FI continued to improve in the interval. There was a significant improvement in presence and intensity of abdominal pain between days 10 and 17. At day ten, none of the children had blood in the stools and continued with no blood in stools at 17. More children had normal stools on day seventeen than on day ten.
Discussion
This is the first study to assess the efficacy of transcutaneous PTNS for the treatment of FC in children. In this single-center prospective interventional study, we found that the application of PTNS was associated with clinical improvement in the great majority of children (20/21). There were no differences in outcomes between the application of the PTNS in the outpatient setting or at home. Our results showed a significant improvement in consistency of BMs, blood in the stools and abdominal pain. Twelve out of sixteen (75%) patients who had hard stools had normal stool consistency at the end of follow-up. None of the children reported blood in the stools at the completion of the study. The beneficial effect of treatment was also sustained for at least one week after treatment (Fig. 2) with some children continuing to improve and none of them worsening at follow-up once the intervention ended. Only two children had episodes of FI at the end of the study and no children had FI 1 week later.
FI is a debilitating problem that significantly affects children and families. Children with FI have worse quality of life compared to those who have intractable FC without FI [16]. FI is also very distressing for caregivers. Families are frequently distraught and seek consultation out of frustration with the child’s progress and the school system that in many cases is not prepared to manage and support children with FI [17, 18]. There are few proven efficacious treatments for the management of persistent FI. Some of them are invasive, expensive and require a very selected and skillful team. Novel pharmacological treatments that had proven success in the treatment of adult population with FC have failed in children. A common denominator of these clinical trials is that they all failed to resolve FI. Linaclotide failed to provide significant relief in symptoms of FC and FI and side effects were common [19]. The clinical trial of prucalopride trial was negative, mainly due to its inability to meet the FI endpoint [20]. The randomized clinical trial of lubiprostone is yet to be published, but the open label trial have shown that some children can have serious adverse events [21]. In our study, transcutaneous PTNS has shown persistent efficacy in treating FI. In the setting of the shortcomings of pharmacological and non-pharmacological treatments for the treatment of intractable FC and FI, it is refreshing and exciting to consider the possibility of novel treatments. Although, we should not overemphasize the results of a small and non-randomized study, the results are encouraging and merit further investigations. If the results of this investigation are confirmed in future studies, PTNS may become a suitable alternative for SNS and other therapies [9].
SNS has been shown to be effective in treating both urinary and FI in adults and children. A study by Lu et al. suggested that SNS is a promising and durable treatment that is particularly effective in decreasing FI in children with refractory constipation [11]. Dinning et al. has shown that SNS at a suprasensory threshold significantly increased the antegrade pan-colonic wave sequence in adult patients with slow transit constipation [22]. SNS may act at the spinal cord level by modulation of the enteric nervous system or reflex pathways to normalize transit [23]. However SNS is expensive, requires surgical implantation and can be associated with postoperative complications such as leg discomfort, infections, further surgeries, and device removal or replacement [11, 24]. The procedure is based on the electric stimulation of the sacral nerve root by an implanted lead wire connected to a pulse generator battery. By using, transcutaneous PTNS, we are seeking to achieve similar results as SNS in a noninvasive way. Posterior tibial nerve arises from nerve roots L4–S3, the same nerve roots that supply the pelvic floor and hindgut. Its mechanism of action remains incompletely understood, but it has been hypothesized that the stimulation of the PTNS could stimulate the pudendal nerve (S2–S4) via afferents fibers, leading to contraction of striated pelvic floor fibers, activation of detrusor inhibitory reflex, and improvement of transit time [25].
PTNS has been used in adults for the treatment of urinary incontinence, chronic pelvic pain, sexual dysfunction, and FI for approximately 40 years [26]. In the pediatric population, transcutaneous PTNS has been used for refractory overactive bladder with observed urodynamic improvement [15]. Although long-term outcomes of PTNS for adults with fecal and vesical disorders have been reported, information on long-term outcomes for children with defecation disorders remains limited [13, 26]. Our study suggests that transcutaneous PTNS has the potential to fill a vacuum in the treatment of FC in children. Transcutaneous PTNS is a noninvasive, easy to use treatment that as our study showed can be used in home setting. As reported by Iqbal et al., daily self-administered bilateral PTNS in adult patients with chronic constipation has been used as a safe and effective method [27]. Similarly, PTNS seems safe to be used in children. No children in our study reported important side effects and only two children had minor discomfort at the site of placement that resolved with change of the electrodes to the other leg.
The study has several limitations. The sample size of the cohort was small. Further studies with larger size sample are needed to address this limitation. Lack of a control group for comparison should be addressed in future studies. Our follow-up was limited to 7 days post-procedure. This limited our assessment to observe if the procedure maintains long-term effects. The study focused on children with FC exclusively, this precludes us from assessing the potential effect of PTNS on other gastrointestinal diseases.
In conclusion, we found improvement in stool consistency, FI and blood in stools at the end of the trial with sustained benefits in abdominal pain, blood in stools and FI at 7 days follow-up. The treatment was safe, easy to administer and well tolerated. PTNS may be a promising noninvasive at home non-pharmacological treatment for FC in children. Larger studies with long-term follow-up should confirm our findings. Controlled randomized clinical trials are recommended.
Data availability
N/A.
Abbreviations
- FC:
-
Functional constipation
- SNS:
-
Sacral nerve stimulation
- PTNS:
-
Posterior tibial nerve stimulation
- FI:
-
Fecal incontinence
- BM:
-
Bowel movement
References
Koppen IJN, Vriesman MH, Saps M et al (2018) Prevalence of functional defecation disorders in children: a systematic review and meta-analysis. J Pediatr 198:121-130.e6
of the Nourth CG (2006) Evaluation and treatment of constipation in infants and children: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr 43(3):e1–13
Koppen IJN, Di Lorenzo C, Saps M et al (2016) Childhood Constipation: finally, something is moving! Expert Rev Gastroenterol Hepatol 10(1):141–155
Liem O, Harman J, Benninga M et al (2009) Health utilization and cost impact of childhood constipation in the United States. J Pediatr 154(2):258–262
Madani S, Tsang L, Kamat D (2016) Constipation in children: a practical review. Pediatr Ann 1;45(5):e189–196
Tabbers MM, DiLorenzo C, Berger MY et al (2014) Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr 58(2):258–274
Ricard J, Quénéhervé L, Lefevre C et al (2019) Anterograde Colonic irrigations by percutaneous endoscopic caecostomy in refractory colorectal functional disorders. Int J Colorectal Dis 34(1):169–175
Vriesman MH, Wang L, Park C et al (2020) Comparison of antegrade continence enema treatment and sacral nerve stimulation for children with severe functional constipation and fecal incontinence. Neurogastroenterol Motil [Internet]. [cited 2020 Dec 6];32(8). Available from: https://onlinelibrary.wiley.com/doi/abs/, https://doi.org/10.1111/nmo.13809
Heemskerk SCM, Rotteveel AH, Benninga MA et al (2018) Sacral neuromodulation versus personalized conservative treatment in patients with idiopathic slow-transit constipation: study protocol of the No.2-trial, a multicenter open-label randomized controlled trial and cost-effectiveness analysis. Int J Colorectal Dis 33(4):493–501
Lu PL, Koppen IJN, Orsagh-Yentis DK et al (2018) Sacral nerve stimulation for constipation and fecal incontinence in children: long-term outcomes, patient benefit, and parent satisfaction. Neurogastroenterol Motil 30(2):e13184
Vriesman MH, Koppen IJN, Camilleri M et al (2020) Management of functional constipation in children and adults. Nat Rev Gastroenterol Hepatol 17(1):21–39
Sacco R, Braga A, Disanto G et al (2020) Effectiveness of percutaneous posterior tibial nerve stimulation for the management of bowel dysfunction in multiple sclerosis patients. Mult Scler J 12:135245852097226
Altunrende B, Sengul N, Arisoy O et al (2013) Transcutaneous electrical posterior tibial nerve stimulation for chronic anal fissure: a preliminary study. Int J Colorectal Dis 28(11):1583–1589
Boudaoud N, Binet A, Line A et al (2015) Management of refractory overactive bladder in children by transcutaneous posterior tibial nerve stimulation: a controlled study. J Pediatr Urol 11(3):138.e1-138.e10
Kovacic K, Sood MR, Mugie S et al (2015) A multicenter study on childhood constipation and fecal incontinence: effects on quality of life. J Pediatr 166(6):1482-1487.e1
Cushing CC, Martinez-Leo B, Bischoff A et al (2016) Health-Related quality of life and parental stress in children with fecal incontinence: a normative comparison. J Pediatr Gastroenterol Nutr 63(6):633–636
Bongers MEJ, van Dijk M, Benninga MA (2009) Health Related quality of life in children with constipation-associated fecal incontinence. J Pediatr 154(5):749-753.e1
Di Lorenzo C, Nurko S, Hyams JS et al (2019) 1151 Linaclotide safety and efficacy in children aged 6 to 17 years with functional constipation. Am J Gastroenterol 114(1):S645–S646
Mugie SM, Korczowski B, Bodi P et al (2014) Prucalopride is no more effective than placebo for children with functional constipation. Gastroenterology 147(6):1285-1295.e1
Hyman PE, Di Lorenzo C, Prestridge LL et al (2014) Lubiprostone for the treatment of functional constipation in children: J Pediatr Gastroenterol Nutr 58(3):283–291
Dinning PG, Hunt LM, Arkwright JW et al (2012) Pancolonic motor response to subsensory and suprasensory sacral nerve stimulation in patients with slow-transit constipation. Br J Surg 99(7):1002–1010
Thomas GP, Dudding TC, Rahbour G et al (2013) Sacral nerve stimulation for constipation. Br J Surg 100(2):174–181
Dudding TC, Meng Lee E, Faiz O et al (2008) Economic evaluation of sacral nerve stimulation for faecal incontinence. Br J Surg 95(9):115
Queralto M, Portier G, Cabarrot PH et al (2006) Preliminary results of peripheral transcutaneous neuromodulation in the treatment of idiopathic fecal incontinence. Int J Colorectal Dis 21(7):670–672
Biemans JMAE, van Balken MR (2013) Efficacy and effectiveness of percutaneous tibial nerve stimulation in the treatment of pelvic organ disorders: a systematic review: PTNS in the treatment of pelvic organ disorders. Neuromodulation Technol Neural Interface 16(1):25–34
Iqbal F, Collins B, Thomas GP et al (2016) Bilateral transcutaneous tibial nerve stimulation for chronic constipation. Colorectal Dis 18(2):173–178
Di Lorenzo C, de Jong JR, Benninga MA (2017) Surgical management of children with intractable functional constipation; experience of a single tertiary children’s hospital. Neurogastroenterol Motil 29(5):e13005
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Carlos Velasco-Benitez, Melissa Mendez, and Eder Villamarin. The first draft of the manuscript was written by Miguel Saps and Gregory Hungria and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Institutional Review Board of Mario Correa Rengifo General Hospital of Cali, Colombia under the Resolution 8430 of the Colombian Ministry of Health, with the following approval number SDCI-2.0–11-02–183.
Consent to participate
Informed consent was obtained from all individual participants included in the study. Written informed consent was obtained from the parents.
Consent for publication
N/A.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Velasco-Benitez, C., Villamarin, E., Mendez, M. et al. Efficacy of transcutaneous posterior tibial nerve stimulation in functional constipation. Eur J Pediatr 182, 1309–1315 (2023). https://doi.org/10.1007/s00431-022-04798-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-022-04798-w