
Abstract
Evidence-based practice (EBP) significantly improves the quality of healthcare, but its use in community pediatrics has not yet been proven. We aimed to assess how Dutch community pediatricians use scientific findings and apply evidence-based practice in everyday well-child care. We interviewed a purposive sample of 14 community pediatricians in the Netherlands regarding their professional activities in daily practice, focusing on instances in which their professional knowledge was insufficient to address the issue at hand. We transcribed the interviews verbatim, and coded them using ATLAS.ti software. We structured the information using template analysis. Community pediatricians relied largely on guidelines of their own profession. If these were not sufficient, they first consulted other medical specialists or colleagues, or used different sources that they considered reliable. They only rarely performed an EBP search, and if so, only for somatic problems. For psychosocial problems, they used a strategy of extensive interaction with clients and members of multidisciplinary teams. We identified five barriers to performing an EBP search: (1) a conviction that not every community pediatrician needs to be able to perform an EBP search; (2) a conviction that an EBP search is not suitable for psychosocial problems; (3) lack of confidence in one’s own abilities to perform an EBP search; (4) limited access to literature; (5) lack of time.
Conclusions: Community pediatricians rely on professional guidelines; this indicates a need to keep these up-to-date and user-friendly. Furthermore, pediatricians should be better trained in performing EBP searches, and in working in multidisciplinary teams, especially for psychosocial problems.
What is Known: |
• Conducting an evidence-based practice search is considered indispensable to determine the best management of the patient’s problem. |
• Conducting such a search is still considered challenging in many medical disciplines, including pediatrics. |
What is New: |
• There is a need to strengthen skills of community pediatricians to find evidence on psychosocial problems and to present this effectively in multidisciplinary teams. |
• The pediatricians’ broad use of other sources of evidence, like experts and online sources, shows the importance of critical evaluation skills. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Evidence-based medicine has a broadly supported role in improving the quality of healthcare [1, 2], but evidence is lacking regarding the extent of its use in community pediatrics. Kelly [1] has described the work of researchers like Sackett and Cochrane to establish the value of evidence-based medicine. Furthermore, Sackett et al. [3] have affirmed the need to combine evidence with clinical expertise and patients’ choices when making medical decisions. Finally, Dawes et al. [4] have proposed the broader concept known as evidence-based practice (EBP). Using this concept, we also define an EBP search as a process involving five steps: ask, access, assess, apply, and audit. Many medical disciplines have developed evidence-based guidelines, with state-of-the-art recommendations for common patient problems, to support EBP. When guidelines are inadequate or outdated, an EBP search is considered indispensable to determine the best management of the patient’s problem. However, conducting such a search is still considered challenging in many medical disciplines [5,6,7], including pediatrics [8].
Regarding pediatric practice, Draaisma et al. [8] have pointed out that, although for pediatricians in clinical care it was difficult to conduct an EBP search regularly, this could be promoted with the use of proper interventions. Whether that also holds for community pediatricians is unknown. The Dutch setting provides an excellent opportunity to assess this application of EBP in community pediatrics, as in the Netherlands well-child care is provided by community pediatricians who do not provide clinical care. Therefore, the aim of this study was to assess how Dutch community pediatricians use scientific evidence and how they apply EBP principles in everyday well-child care.
Methods
For this study, we used semi-structured interviews with community pediatricians.
Sample
We obtained a purposive sample of 14 participants from among 96 community pediatricians who graduated between January 2015 and January 2018 from the Netherlands School of Public and Occupational Health (NSPOH), one of the two Dutch postgraduate medical schools for community pediatricians. Roughly 60% of community pediatricians in the Netherlands are trained at the NSPOH. To maximize variability, we selected participants from different work situations (employed in a well-child clinic or a municipal public health service) and with varied education (two-years training as community pediatrician or 4-year training as community medicine specialist in pediatric care).
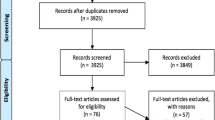
Participants were invited by e-mail and, in case of no reply, by telephone. They were eligible if they were actually working as a community pediatrician in daily practice, and not involved in further training as a general specialist in community medicine. Figure 1 shows the flow of participant selection. The Ethical Review Board of the Netherlands Association for Medical Education approved the study protocol (file 2018.7.6).

Flow diagram of participant selection
Procedure and measures
Each participant received a questionnaire (Supplementary File 1) on background characteristics, and was interviewed by the first author JJdS between February 2019 and August 2020. JJdS is an educational scientist, trained in interviewing techniques. He was responsible for organizing the training on EBP principles for the participants at the NSPOH. All participants received information about the study, including its aims and content; each signed an informed-consent form.
Interviews were conducted in a semi-structured way, using a topic-list; they lasted about one hour, and were audio-recorded. Five participants were interviewed face-to-face, the other nine by phone, in three cases because of COVID-related restraints. The topic-list was tested in a pilot interview, resulting in the following lead question in the final version: “If you have to make a medical decision or provide a client with advice, but your professional knowledge is not sufficient, how do you deal with that? Could you please provide some examples?” The interviewer subsequently focused on what the participant did to gain enough basis for a decision or an advice. If topics like use of evidence, clinical expertise, and patients’ choice, according to categories proposed by Sackett [3], or specifics regarding the steps of an EBP search [4] were not mentioned spontaneously, the interviewer asked specific questions about them. Follow-up questions focused on the attitude of colleagues and the organization [5] toward EBP. After the fourth interview we added a question about the obligatory peer-review sessions for community pediatricians, because in that interview these sessions appeared to be a useful context for an EBP search. The final version of the topic list is shown in Supplementary File 2.
Data analysis
All interviews were transcribed verbatim by a certified external office and coded in ATLAS.ti by JJdS. Data analysis was performed simultaneously with the interviews, in line with the principles of template analysis [9]. To improve information power, we continued to conduct interviews until no new codes appeared from the data. Four interviews were double coded, two by AJMH, a community medicine specialist in pediatric care, and two by FWN, a trainer in basics of research methodology. The code-tree was discussed repeatedly with all authors and adjusted cumulatively during the coding; its final version is shown in Supplementary File 3.
Results
Characteristics of the sample
Participants worked at twelve different organizations across the Netherlands. Their mean age was 48 years (SD 7.3; range 33–60). Thirteen were female and one male. They had completed their undergraduate medical education 10 to 22 years previous to the interview. Two participants had followed an extra course on EBP and two had contributed to a publication on community pediatrics. Ten had followed a 2 years’ basic specialist training, and four the 4 years’ specialist training.
How do community pediatricians in well-child care use scientific evidence?
Most participants considered it important to keep their professional knowledge up to date. If their knowledge appeared inadequate in a specific professional context with a client, they reported handling this first by consulting professional guidelines and other medical specialists. If that did not suffice, they used varied follow-up approaches for somatic and for psychosocial problems, as outlined further.
Keep professional knowledge up to date
As important reasons to keep their knowledge up to date, participants mentioned the ability to provide adequate care and to confer effectively with other disciplines. They kept track of new developments in their area of expertise by consulting a limited number of scientific journals, training programs, and newsletters, but often also social media: [29Footnote 1: “I read … a lot of professional information on all kinds of topics that are also shared via Twitter, for example, and … then I read the original research”].
Most participants considered indirect access to literature adequate for this purpose. However, lack of time often prevented them from keeping their knowledge up to date: reading professional literature was often a spare time activity.
In case of gaps in professional knowledge: consult professional guidelines, peers, or other specialists
When in doubt, participants first checked the guidelines of the Dutch national expertise center on well-child care, the NCJ [10]. These evidence-based professional guidelines provide guidance for a considerable number of somatic and psychosocial problems. They were broadly used and appreciated: [15: “Well, just look at all those guidelines, they really help us in our work. And how did they come about? By research!”]. Sometimes, no relevant guideline was available, or an existing guideline was outdated. In such cases, the participants conferred with colleagues or with other medical specialists, who could easily be reached for a telephone or digital consultation. Participants also used other sources considered to be reliable, like websites from pediatricians and dermatologists or relevant guidelines from other disciplines.
Different follow-up approaches for somatic or psychosocial problems
For somatic problems, the community pediatricians generally could decide independently on the course of action. The consultation stage mentioned above usually provided them with sufficient information. If not, some participants searched for specific studies or started a systematic EBP search. Such searches were performed sometimes individually, and sometimes with other colleagues, as part of peer-review sessions.
However, for psychosocial problems, the participants indicated that guidelines were not always available, and if so, they were often not sufficient to rely on for decisions or advice. The complexity of the clients’ problems usually led to a different consultation stage, characterized by extensive interaction with clients: [15: “…for a behavioral problem, it is more like practicing judo with parents … what is their concern, what is mine? … It becomes more practice-based”]. Also, not the individual community pediatrician, but members of multidisciplinary teams, consisting of nurses, social workers, and psychologists, decided on the course of action. Working in multidisciplinary teams was sometimes very effective, but could cause frustration as well: [26: “… They do not listen to evidence … We are all considered equal, a doctor with more than 20 years of experience and an advisor who has just started working … and then the person who submits the case … can choose which advice he wants to follow”]. For psychosocial problems, none of the participants considered starting an EBP search useful.
How do community pediatricians in well-child care apply EBP principles?
Regarding application of EBP principles, most participants indicated that in daily practice they never conducted a formal EBP search; the few examples mentioned are described below. Our study identified five barriers to performing an EBP search and these too are described below.
Examples of EBP searches performed
Some participants had performed partial EBP searches to find up-to-date answers on specific questions of clients: [43: “Sometimes parents … have a very clear opinion on weaning. …. Then I also look up … the latest studies on breastfeeding and supplementary feeding”]. Other EBP searches were aimed at developing organization-specific evidence-based guidelines for common practical questions. An interesting example was the use by one organization of peer-review sessions to perform EBP searches together: [25: “We … recently discussed … micro- and macrocephaly … so that we can make … better working agreements for colleagues; we … will, … look up articles about it … and make a summary and discuss it … during the peer-review session”].
Barriers mentioned
Participants mentioned the following five barriers to using an EBP search:
Barrier 1: Conviction that not every community pediatrician needs to be able to perform an EBP search
Some participants strongly indicated that being able to perform an EBP search is not necessary to perform well as a community pediatrician: [36: “I’m more for practice-based evidence than evidence-based practice. We can’t all be scientists…. Let me just examine the kids and give guidance to the parents—I’m good at that”]. Other participants stressed the opposite, namely that they considered it important for every community pediatrician to be able to derive substantiated advice from relevant literature.
Barrier 2: Conviction that an EBP search is not suitable for psychosocial problems
The participants considered it obvious that an EBP search is most appropriate in relation to somatic questions. They indicated that a search in PubMed was not likely to be successful for psychosocial problems: [15: “… breastfeeding and a certain medication is specific and small and medical; PubMed is suitable for this; … if you … start looking for social stuff in PubMed you will get bogged down very quickly”]. If they did mention using peer-review sessions to find answers to psychosocial problems, these sessions were aimed at discussing cases and not at performing an EBP search in order to support a decision or give advice.
Barrier 3: Lack of confidence in one’s own abilities to perform an EBP search
Some participants indicated feeling sufficiently confident to conduct an EBP search. However, most felt inadequate to do so, especially in comparison with colleagues who had much more recently completed their undergraduate medical education.
Barrier 4: Limited access to literature
Those participants who conducted EBP searches had access to full-text literature through a shared license. Of those who did not, some mentioned that they had to request specific literature from a library; as a result, this was a barrier to using literature: [36: “… if scientific literature would be much easier to access … one might be more inclined to look for it”].
Barrier 5: Lack of time
Most participants mentioned lack of time as a hindrance to gaining the experience needed to do a thorough EBP search: [16: “… If you don’t do that very often, it takes a lot more time and you don’t always allow yourself that time”].
Discussion
We found that community pediatricians first preferred to consult the national guidelines of their own profession when their knowledge was insufficient to give advice or make decisions. Subsequently, they preferred to consult other experts and sources they considered reliable. For somatic problems, they usually found this procedure to be sufficient as a base for their advice or decisions. They occasionally performed additional EBP searches. However, for psychosocial problems, it was necessary to have much more interaction with clients and within multidisciplinary teams, and they never conducted EBP searches.
We found five barriers that prevented community pediatricians from performing an EBP search: a conviction that not every community pediatrician needs to be able to perform an EBP search; a conviction that an EBP search is not suitable for psychosocial problems; lack of confidence in one’s own abilities to perform an EBP search; limited access to literature; and lack of time.
Interpretation of main findings
We found that the community pediatricians preferred national professional guidelines, and only subsequently applied a broader strategy to find evidence. This aligns with the finding that the 35 available guidelines provide adequate evidence and cover the routine offer of well-child care [11], which is important in professional situations when time is scarce. We found that for psychosocial problems, the community pediatricians moved quickly from the use of guidelines to a strategy of intensive interaction with clients and multidisciplinary teams; a possible explanation is that they considered these guidelines less applicable to the complex problems of their clients. We also found that working in multi-disciplinary teams posed an extra challenge — for instance, to reach consensus about the client’s problem and to acknowledge the contribution and value of each discipline involved. This finding aligns with that of Dopson et al. [12] that different professions can have different views about what constitutes credible evidence.
We found that the community pediatricians seldom performed an EBP search. This finding aligns with findings related to other disciplines [5,6,7], although we found some different barriers. The first barrier — the conviction that not every community pediatrician needs to be able to perform an EBP search — contrasts with the general support for EBP in all medical professions [1, 2], including AJN Jeugdartsen Nederland, the Dutch organization of community pediatricians [13]. The second barrier — the conviction that an EBP search is not considered suitable for psychosocial problems — is a remarkable finding. It contrasts with the fact that there is published evidence on the best handling of psychosocial problems (e.g. [14,15,16,17]). This incorrect assumption prevents pediatricians from making use of existing evidence. The third barrier — lack of confidence in one’s own abilities to perform an EBP search — is possibly caused by a lack of practice in using EBP. The participants graduated from their professional medical education 10 to 20 years ago, at a time when intensive training in using EBP principles was less common and the online EBP search possibilities were limited and more complicated. The fourth barrier — limited and incomplete access to literature — and the fifth barrier — lack of time — both align with findings in other studies [5, 18, 19].
In summary, the community pediatricians, like other medical specialists, reported that they valued professional guidelines as an important source of evidence, and they seldom performed EBP searches. For dealing with psychosocial problems, they considered it obvious that EBP searches would not be successful, a conclusion which contrasts with the availability of published evidence.
Strengths and limitations
A strength of this study is that it yielded a rich description of the results, with illustrative citations, in an area where evidence was not yet available. Another strength is the diversity of the research team, made up of both community pediatricians and educational scientists. This provided a multi-perspective interpretation of the data, thereby augmenting the credibility of the results.
A limitation of the study is that participants included graduates from only one of the two schools for community pediatricians in the Netherlands. However, the schools’ curriculums on EBP are broadly comparable, implying that our findings most likely apply to graduates from both schools. Another limitation may be that interviewer JJdS was also involved in the EBP training of the participants. However, that some answers were socially less desirable indicates that the interview setting was probably considered safe. A third possible limitation is that we interviewed a limited group, of only 14 participants. However, our sample of the study population was purposeful, resulting in a sufficiently heterogeneous group of participants. Also, the final three interviews which we used for verification of findings yielded no new information or codes. This suggests the presence of sufficient information power.
Implications and conclusion
Community pediatricians used national professional guidelines as their main source of scientific evidence; this indicates the value of these guidelines as well as the need for regular and frequent updates and extensions. Community pediatricians need more training and practice in skills to perform EBP searches and need sufficient time and unlimited access to literature. The pediatricians’ broad use of other sources of evidence, like experts and online sources, shows the importance of critical evaluation skills. Regarding the relatively new development of working in multi-disciplinary teams for psychosocial cases, our findings suggest a need for training in how to grade the quality of the evidence found in literature databases and other sources and how to communicate this information effectively within interdisciplinary settings. Our findings regarding barriers indicate a need to strengthen practitioners’ skills to find evidence on psychosocial problems. We identified the conducting of a systematic EBP search with colleagues in peer-review sessions as a best practice, and recommend that community pediatricians in more organizations begin to implement this practice. In conclusion, we found that in their everyday well-child care, most Dutch community pediatricians relied for evidence first on national guidelines and then on other sources, but they seldom performed an EBP search. Implications for practice are that excellent and up-to-date national guidelines are important and that several important skills should receive attention during postgraduate education, preferably combined with practice in the work setting: skills to perform EBP searches, critical evaluation skills, skills to work in multidisciplinary teams, and skills to find evidence on psychosocial problems. Our findings need confirmation in other countries with different systems of pediatric care.
Notes
Quotes of participants are given between brackets and in italics, and are preceded by a unique (Fig. 1) participant number.
Abbreviations
- EBP:
-
Evidence-based practice
- NCJ:
-
Dutch national expertise center on well-child care — Nederlands Centrum Jeugdgezondheid
- NSPOH:
-
Netherlands School of Public and Occupational Health
References
Kelly MP (2018) The need for a rationalist turn in evidence-based medicine. J Eval Clin Pract 24(5):1158–1165. https://doi.org/10.1111/jep.12974
McCartney M, Treadwell J, Maskrey N, Lehman R (2016) Making evidence based medicine work for individual patients. BMJ 353:i2452. Published 2016 May 16. https://doi.org/10.1136/bmj.i2452
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS (1996) Evidence based medicine: what it is and what it isn’t. BMJ 312(7023):71–72. https://doi.org/10.1136/bmj.312.7023.71
Dawes M, Summerskill W, Glasziou P, Cartabellotta A, Martin J, Hopayian K, Porzsolt F, Burls A, Osborne J (2005) Sicily statement on evidence-based practice. BMC Med Educ 5(1):1. Published 2005 Jan 5. https://doi.org/10.1186/1472-6920-5-1
Zwolsman S, te Pas E, Hooft L, Wieringa-de Waard M, Van Dijk N (2012) Barriers to GPs’ use of evidence-based medicine: a systematic review. Br J Gen Pract 62(600):e511–e521. https://doi.org/10.3399/bjgp12X652382
Swennen MH, van der Heijden GJ, Boeije HR, Van Rheenen N, Verheul FJM, Van der Graaf Y, Kalkman CJ (2013) Doctors’ perceptions and use of evidence-based medicine: a systematic review and thematic synthesis of qualitative studies. Acad Med 88(9):1384–1396. https://doi.org/10.1097/ACM.0b013e31829ed3cc
Ubbink DT, Vermeulen H, Knops AM, Legemate DA, Oude Rengerink K, Heineman MJ, Roos YB, Fijnvandraat CJ, Heymans HS, Simons R, Levi M (2011) Implementation of evidence-based practice: outside the box, throughout the hospital. Neth J Med 69(2):87–94
Draaisma E, Bekhof J, Langenhorst VJ, Brand PLP (2018) Implementing evidence-based medicine in a busy general hospital department: results and critical success factors. BMJ Evid Based Med 23(5):173–176. https://doi.org/10.1136/bmjebm-2018-110895
Brooks J, McCluskey S, Turley E, King N (2015) The utility of template analysis in qualitative psychology research. Qual Res Psychol 12(2):202–222. https://doi.org/10.1080/14780887.2014.955224
Nederlands Centrum Jeugdgezondheid (2021) Richtlijnen https://www.ncj.nl/richtlijnen/. Accessed 24 May 2021
Vanneste YTM, Lanting CI, Detmar SB (2022) The Preventive Child and Youth Healthcare Service in the Netherlands: the state of the art and challenges ahead. Int J Environ Res Public Health 19:8736. https://doi.org/10.3390/ijerph19148736
Dopson S, FitzGerald L, Ferlie E, Gabbay J, Locock L (2010) No magic targets! Changing clinical practice to become more evidence based. Health Care Manage Rev 35(1):2–12. https://doi.org/10.1097/HMR.0b013e3181c88e79
AJN (2021) Jeugdartsen Nederland https://ajnjeugdartsen.nl/. Accessed 24 May 2021
Bitto Urbanova L, Holubcikova J, Madarasova Geckova A, Van Dijk JP, Reijneveld SA (2020) Adolescents exposed to discrimination: are they more prone to excessive internet use? BMC Pediatr 20(1):402. Published 2020 Aug 25. https://doi.org/10.1186/s12887-020-02241-3
Den Haan PJ, de Kroon MLA, van Dokkum NH, Kerstjens JM, Reijneveld SA, Bos AF (2019) Risk factors for emotional and behavioral problems in moderately-late preterms. PLoS One 14(5):e0216468. Published 2019 May 2. https://doi.org/10.1371/journal.pone.0216468
Paclikova K, Dankulincova Veselska Z, Madarasova Geckova A, Van Dijk JP, Reijneveld SA (2020) Adolescent enrollment in psychosocial care: do parents make a difference? Int J Environ Res Public Health17(19):7066. Published 2020 Sep 27. https://doi.org/10.3390/ijerph17197066
Van der Zee-van den Berg AI, Boere-Boonekamp MM, Groothuis-Oudshoorn CGM, IJzerman MJ, Haasnoot-Smallegange RME, Reijneveld SA (2017) Post-up study: postpartum depression screening in well-child care and maternal outcomes. Pediatrics 140(4):e20170110. https://doi.org/10.1542/peds.2017-0110
Solomons NM, Spross JA (2011) Evidence-based practice barriers and facilitators from a continuous quality improvement perspective: an integrative review. J Nurs Manag 19(1):109–120. https://doi.org/10.1111/j.1365-2834.2010.01144.x
Van Dijk N, Hooft L, Wieringa-de WM (2010) What are the barriers to residents’ practicing evidence-based medicine? A systematic review Acad Med 85(7):1163–1170. https://doi.org/10.1097/ACM.0b013e3181d4152f
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by JJ De Schipper and the data were partially double coded by AJM Hermans and FW Noordik. All authors discussed the analysis and results. The draft of the manuscript was written by JJ De Schipper, and all authors commented and gave substantive suggestions, critical revisions, and additions to the manuscript. All authors read and approved the final manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval
The Ethical Review Board of the Netherlands Association for Medical Education approved the study protocol (file 2018.7.6).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Jaarsma ADC was affiliated to Department of Research and Innovation in Medical Education, University Medical Center, University of Groningen, Groningen, The Netherlands, until August 2021.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
De Schipper, J., Hermans, A., Jaarsma, A. et al. Evidence-based practice in well-child care. Eur J Pediatr 181, 4183–4189 (2022). https://doi.org/10.1007/s00431-022-04624-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-022-04624-3