
Abstract
The present paper reviews the diagnosis of imported malaria in children. Malaria is caused by a parasite called Plasmodium and occurs in over 100 countries worldwide. Children account for 10–15% of all patients with imported malaria and are at risk to develop severe and life-threatening complications especially when infected with Plasmodium falciparum. Case–fatality ratios vary between 0.2% and 0.4%. Children visiting friends and relatives in malaria endemic areas and immigrants and refugees account for the vast majority of cases. Symptoms are non-specific and delayed infections (more than 3 months after return from an endemic country) may occur. Microscopic analysis of the thick blood film is the cornerstone of laboratory diagnosis. For pragmatic reasons, EDTA-anticoagulated blood is accepted, provided that slides are prepared within 1 h after collection. Information about the Plasmodium species (in particular P. falciparum versus the non-falciparum species) and the parasite density is essential for patient management. Molecular methods in reference settings are an adjunct for species differentiation. Signals generated by automated hematology analyzers may trigger the diagnosis of malaria in non-suspected cases. Malaria rapid diagnostic tests are reliable in the diagnosis of P. falciparum but not for the detection of the non-falciparum species. They do not provide information about parasite density and should be used as an adjunct (and not a substitute) to microscopy. In case of persistent suspicion and negative microscopy results, repeat testing every 8–12 h for at least three consecutive samplings is recommended. A high index of suspicion and a close interaction with the laboratory may assure timely diagnosis of imported malaria.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Malaria is endemic in over 100 countries worldwide [62]. In endemic regions, it is a serious health problem with an estimated 863,000 people dying each year of which 85% are children under the age of 5 years [59]. Imported malaria, i.e., malaria contracted in an endemic region but diagnosed in a non-endemic country [33], is a rare event but may have a fatal outcome. Due to its rare occurrence, physicians and laboratory staff are not familiar with its diagnosis. Prompt and accurate diagnosis is, however, critical for the effective management of malaria [44].
The present paper gives an overview of the clinically relevant features of the cycle of the Plasmodium parasite and a short reminder of the clinical presentation of malaria in children. Next, it focuses on the laboratory diagnosis of imported malaria in a non-endemic setting and gives an update on the diagnostic value and place of malaria rapid diagnostic tests.
The Plasmodium species
The parasite
Malaria is caused by a parasite called Plasmodium, which is transmitted through the bites of the infected Anopheles mosquito. There are four human Plasmodium species: Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae. Recently, human infections with a fifth species, Plasmodium knowlesi, which is usually found in monkeys, have been reported [48]. Figure 1 depicts the life cycle of malaria parasites in humans. A detailed description of the Plasmodium life cycle can be found in reference [35].

Plasmodium life cycle. Retrieved from Centers for Disease Control and Prevention (CDC). Available at http://www.cdc.gov/malaria/about/biology/
The cycle in the human host: from liver to blood, hypnozoites, relapse, and recrudescence
Plasmodium has a sexual cycle inside the mosquito and an asexual cycle inside man. During the bite of an infected female mosquito, Plasmodium sporozoites are injected in the blood and move to liver cells where they develop into liver schizonts. After the rupture of the schizonts (approximately 1 week after infection), merozoites are released into the bloodstream and each of them will invade a RBC. There they develop into ring forms (trophozoites) which mature into schizonts that divide into merozoites which invade new RBCs. The rupture of the schizont and release of merozoites give rise to the so-called malaria paroxysms with spiking fever and rigors. The time required to complete the RBC cycle (from invading merozoites over trophozoites to rupturing schizont) depends on the species: for P. falciparum, P. ovale, P. vivax, and P. ovale, the cycle takes 48 h; for P. malariae and P. knowlesi, it takes 72 h and 24 h, respectively. In non-immune patients, however, particularly when infected with P. falciparum, parasites tend to mature asynchronously, resulting in irregular fever patterns [67].
After 1 or 2 weeks, gametocytes, the sexual form of Plasmodium, will be produced. These gametocytes continue the sexual cycle when taken up by a mosquito during a next blood meal. The sexual cycle will be completed over a period of 2 weeks, where after the mosquito can infect another human host.
In case of P. vivax and P. ovale infections, dormant liver stages (hypnozoites) may cause infections (so-called relapses) weeks to months after adequate prophylaxis or effective blood-stage therapy of a primary infection. P. malariae may persist in the blood at undetectable levels without causing symptoms for many years and may subsequently develop into clinical illness in patients under immunosuppressive drugs or after splenectomy (these infections are referred to as recrudescence) [67].
The red blood cell: differences in parasite densities among the Plasmodium species
P. vivax and P. ovale only infect young RBCs and P. malariae only infects old RBCs; hence, the percentages of infected RBCs (designated as “parasite density” or “parasitemia”) are usually lower than 2% and 1%, respectively. By contrast, P. falciparum infection has not such a preference and there is no intrinsic limit to the parasite density. In addition, RBCs infected by P. falciparum stick to the capillary endothelium and occlude the microvascular circulation in the deep organs (a process called sequestration), leading to the manifestations of what is defined as severe malaria: metabolic acidosis, cerebral malaria (coma), renal insufficiency, and acute respiratory distress. In addition, hypoglycemia can occur. By consequence, P. falciparum is the most dangerous species, and infection may become fatal when treatment is delayed for more than 24 h after presentation of symptoms [62]. The other species are thought to be less severe though organ involvement and case fatalities have been described for P. vivax as well [41].
Geographic distribution of Plasmodium species
P. falciparum is the predominant species in Africa, where P. vivax is virtually absent (because most Africans lack the Duffy blood group antigen which enables P. vivax to enter the RBC), except for some areas in Eastern Africa. P. ovale is mainly restricted to Africa; rare cases have been observed in Haiti and Oceania. P. malariae is the second common species in Africa and also distributed in other geographic areas. Latin America is predominated by P. vivax though P. falciparum is present as well. The same goes for the Indian sub-continent and South-East Asia where P. malariae is also prevalent.
Imported malaria in children
Children at risk: few tourist travelers, mostly visiting friends and relatives or immigrants
Yearly, more than 125 million international travelers visit malaria endemic countries and over 10,000 people are reported to fall ill upon return to their home country, though this number might even be as high as 30,000 [62]. However, in most European countries, imported malaria has been declining during the past 10 years [53]; possible explanations are the increased use of prophylaxis or a decreased transmission intensity in the visited malaria endemic areas, though this remains to be confirmed [53].
Children account for 10–15% of all patients with imported malaria [11, 23, 39] and share with pregnant women the highest risk to develop severe and life-threatening complications [62]. Children of the so-called visiting friends and relatives category (further referred to as VFR children) are the main group at risk [47]. VFR children are born in non-endemic countries to parents originating from malaria endemic areas and contract malaria upon visits to malaria endemic regions. Immigrated children and refugees are another risk group [47]. In an Italian and a Spanish study, imported malaria in children was exclusively observed among VFR children and immigrants [1, 39]. These findings were confirmed in other studies, with VFR children accounting for most of the cases versus tourist travelers representing only a minor part [11, 33, 34]. Among 194 children with imported malaria in the USA for the year 2004, more than half (54.6%) were visiting friends and relatives, and more than a quarter (28.3%) of them were refugees and immigrants. Reasons for this phenomenon are that VFR children hardly comply with preventive measures and have a poor adherence to prophylactic drugs [1, 11, 33, 34, 39]. Their parents have difficult access to travel advice due to language and cultural barriers, and may also believe their children have immunity against malaria because of their ethnic origin, making prophylaxis unnecessary [33]. Semi-immunity does exist in children, but only when born and grown in endemic countries. This semi-immunity wanes after a variable period (usually estimated at 6 months) of not being exposed to malaria (as in the case of migrants and refugees) [39, 49].
A particular group—strictly speaking not to be classified as "import malaria"—are autochthonous malaria cases caused by inadvertently imported Anopheles mosquitoes, either by airplane, ship, or baggage. Although members of airport staff are the primary victims, anecdotal cases of "airport" or "baggage" malaria have been described in children too [28–30]. As Anopheles mosquitoes survive transports in aircrafts, WHO recommends insecticide spraying in flights leaving endemic countries [57].
Non-specific symptoms but serious complications
A 2.5-year-based study in a district hospital in Birmingham, UK assessed 153 children presenting with fever and having traveled to the tropics or subtropics during the previous year and revealed that 14% of them had malaria [54]. Although fever was reported as the major presenting symptom in up to 97.6% of children with imported malaria [24], other studies revealed that 10–17% of children with malaria had no fever upon admission [1, 11]. Other symptoms are non-specific and may mimic diseases like gastrointestinal infections or pneumonia [8].
In the UK, a total of 997 children with imported malaria were reported between 2004 and 2008, of which one third fulfilled the WHO criteria for severe malaria [16]. Other studies from the UK, the Netherlands, and Canada revealed similar proportions [11, 32, 34]. The proportions of children requiring intensive care support ranged from 3% to 40% [11, 16, 34]; most of them survived without sequelae though cerebellar infarction was observed in one out of 10 patients with cerebral malaria [16]. The case–fatality ratio of all imported malaria cases in children varied between 0.2% and 0.4% [3, 16].
How long after return from an endemic country can children develop malaria?
The time between returning home after travel and onset of symptoms depends on the infecting Plasmodium species. In a study including 245 children positive for malaria, the median delay of P. falciparum infection was 5 days (range 0–330 days); for P. vivax, P. ovale, and P. malariae, the recorded delays were 62 (0–330), 25 (0–120), and 37 days (0–188), respectively [65]. It should be reminded, however, that as a consequence of relapse (P. ovale and P. vivax) and recrudescence (P. malariae), clinical malaria can occur even at a later onset. Of interest, P. falciparum, which apparently lacks both features, has been reported with a delayed onset of infection in adults for up to 9 years after acquisition [9, 20, 21, 50].
Malaria diagnosis: patient delay, doctor delay, laboratory delay
Diagnosis is delayed in one third of children with imported malaria [4, 12, 65]. The median time between onset of symptoms and diagnosis of malaria was recorded as 3–4 days [4, 65] but can extend up to 32 days [65]. Importantly with regard to pre-travel advice was that most delay was at the patient’s side, with parents waiting several days before consulting, resulting in a median patient delay of 3 days (range 0–11 days) [4]. The median doctor delay in that study was 0 days (which means that in most cases malaria was considered at the first presentation) but ranged up to 19 days [4]. Other data about doctor delay are variable, with 2% [1] to 60% [32] of doctors failing to consider malaria at first presentation. Finally, there may be a considerable laboratory delay, due to the lack of a competent microbiologist on duty [1] or the lack of microscopic expertise [1, 4]. Indeed, in non-endemic settings, since it is difficult to maintain adequate performance and expertise of the laboratory staff due to the low exposure to malaria-positive samples and especially at low parasite densities, diagnosis may easily be missed [18, 26, 40].
Plasmodium species involved
The Plasmodium species involved reflect the travel destination or the country of origin of the child or his/her migrated parents. Overall, the most encountered species was P. falciparum, accounting for up to 90% of cases, with the majority of infections acquired in Sub-Saharan Africa [11, 23, 34, 65]. P. vivax infections were mostly acquired in the Indian sub-continent by VFR children whose parents were originating from these regions [33]. Table 1 gives an overview of the species distribution and geographic origin of 147 children ≤14 years old diagnosed with malaria in our setting (Institute of Tropical Medicine, Antwerp, Belgium).
The diagnosis of imported malaria in children
Essential information needed in the laboratory diagnosis of malaria
All essential information for diagnosis and patient management can be obtained by microscopy. Plasmodium parasites are looked for in a thick blood film, which consists of a superposition of several layers of blood cells. The RBCs are lysed during the staining process, in preference by Giemsa stain. Thin blood films—as regularly used in the hematological laboratory—represent a monolayer of blood, and are used for Plasmodium species identification, which is based on morphological characteristics of the RBCs (shape and inclusions) and the Plasmodium parasites (Fig. 2).

Giemsa-stained thin blood film of a patient with P. falciparum malaria: the patient was sick for 2 weeks before diagnosis. Numerous red blood cells are infected with small trophozoites (ring forms); some red blood cells contain multiple trophozoites. Three banana-shaped gametocytes (visible only after 1 or 2 weeks of clinical infection) are present and the white blood cell (center) contains black-brown hemozoin pigment
Apart from not missing the diagnosis of malaria, differentiation of P. falciparum from the non-falciparum species is important because of the life-threatening potential of this species. Accurate identification of parasite density appears to be difficult in non-endemic settings [31], but high parasite densities exceeding 2% of RBCs infected should be recognized, as this criterion constitutes an alert sign [61]. Expert microscopists in reference laboratories will recognize P. falciparum stages and hemozoin pigment in white blood cells (WBCs): in the case of P. falciparum infection, schizonts and hemozoin-containing WBCs are indicators of a serious infection, whereas the exclusive presence of gametocytes after treatment is a normal finding [60].
Capillary or venous blood?
Some authors recommend capillary rather than venous blood as the sample of choice for malaria diagnosis because of a presumed higher parasite density in the former [40, 43]. However, this assumption has never been confirmed [25] and for pragmatic reasons, i.e., to assure preparation of (enough) samples of good quality and to allow antigen testing and confirmatory analysis, we advice in our setting to submit a tube of EDTA blood rather than capillary blood specimens.
Details for sampling can be found in reference [36]. For capillary blood, a non-cotton alcohol pad should be used for cleaning as cotton may leave loose fibers resulting in confusing artifacts [43]. Thick and thin blood films should be prepared instantly: for the thick film, a blood spot is applied on a slide and stirred in a circular motion with the corner of the slide, taking care not to make the preparation too thick. The slide is allowed to dry without fixative. For venous blood, EDTA is the anticoagulant of choice. Slides should preferable be prepared within 1 h after collection in order to preserve RBC alterations and parasite morphology [43].
Automated hematology analyzers may trigger the possibility of malaria
Some automated hematology analyzers display an alert (flag) in case of malaria suspicion based on the presence of (1) activated monocytes (Coulter Counter), (2) hemozoin-containing white blood cells (Cell-Dyn series), and (3) an additional peak in the reticulocyte fraction (Cell-Dyn series) [2, 27, 45, 55]. Although diagnostic accuracy of these features is too low to exclusively rely on these flags for malaria diagnosis, the merit of these analyzers is triggering the diagnosis of malaria in patients for whom malaria diagnosis was not requested. As an example, based on flags generated by Cell-Dyn 3200 apparatus used in our laboratory, we retrieved Plasmodium parasites in the blood of seven patients over a 3-year period (2008–2010), for whom malaria diagnosis was not considered upon clinical presentation (including an 11-year-old boy with P. falciparum infection).
Molecular methods can refine the diagnosis
Molecular techniques such as polymerase chain reaction (PCR) are powerful tools with detection limits below that of expert microscopy. For the time being, they do not generate information about parasite density and their turnaround time is too long to be practicable in clinical diagnosis. In our setting, we developed a real-time four-primer Plasmodium-specific PCR as a back-up method for species confirmation and diagnosis of mixed Plasmodium infections [6]. We also converted this method to Giemsa-stained slides and malaria rapid diagnostic tests as the source of DNA, which makes it possible to confirm or refine the diagnosis even when whole blood samples are not available [5, 7].
Malaria rapid diagnostic tests (MRDTs): simple and accurate
Malaria rapid diagnostic tests (MRDTs) detect Plasmodium antigen by an antibody–antigen reaction on a nitrocellulose strip, which is embedded in a plastic cassette or occasionally in a cardboard format (Fig. 3). Malaria-positive samples will present cherry-red test lines which are read by the naked eye. Two-band MRDTs are mostly designed to detect P. falciparum; they display a control line and a test line which targets either histidine-rich protein-2 (HRP-2) or P. falciparum-specific parasite lactate dehydrogenase (Pf-pLDH). Three- and four-band malaria MRDTs display a control line and two or three test lines, one targeting a P. falciparum-specific antigen, another line targeting an antigen common to the four species [either pan-Plasmodium-specific lactate parasite dehydrogenase (pan-pLDH) or aldolase], and, in case of the four-band malaria RDTs, a third line which targets P. vivax-specific pLDH (Pv-pLDH).

Two- and three-band (below) malaria rapid diagnostic tests (MRDTs) with blood transfer devices (pipette and loop). Control and test lines are cherry-red colored. The two-band MRDT (upper) displays a control line and a test line which targets P. falciparum-specific histidine-rich protein-2 (HRP-2) The three-band MRDT (below) displays a control line and two test lines, one targeting HRP-2 and another line targeting pan-parasite lactate dehydrogenase
Figure 4 displays the different components of a MRDT strip and the sequence of reactions on a two-band MRDT strip. Before interpreting test results, the presence of the control line should be confirmed and when absent the test should be repeated. In case of three-band MRDTs, the presence of a single P. falciparum-specific test line indicates an infection with P. falciparum and the presence of a single pan-Plasmodium test line indicates an infection with one of the non-falciparum species. When both test lines are present, this indicates an infection with either P. falciparum or a mixed infection of P. falciparum and one or more of the non-falciparum species.

Schematic drawing of the malaria rapid diagnostic test. Sequence of events when performing a MRDT: blood and buffer are applied, respectively, to the sample and buffer pad. They are attracted by the capillary action of the absorption pad and start to migrate. First, they pass the conjugate pad, which contains a detection antibody targeting a Plasmodium antigen, such as HRP-2, Pf-pLDH, Pv-pLDH, pan-pLDH, or aldolase (for abbreviations see text). This detection antibody is a mouse antibody that is conjugated to a signal, mostly colloidal gold. If present in the sample, the Plasmodium antigen is bound to this detection antibody–conjugate. Next, the antigen–antibody–conjugate complex migrates further until it is bound to the capture antibody, which binds to another site of the Plasmodium target antigen. As the capture antibody is applied on a narrow section of the strip, the complex with the conjugated signal will be concentrated and by virtue of the colloidal gold will become visible as a cherry-red line. The excess of detection antibody–conjugate that was not bound by the antigen and the capture antibody moves further until it is bound to a goat-raised anti-mouse antibody, thereby generating a control line
Malaria rapid diagnostic tests: different accuracies for the four Plasmodium species
Nowadays more than 80 MRDT brands are marketed worldwide [10] and their diagnostic performances may vary. WHO has published two series of diagnostic evaluations [58, 63] and we have evaluated a set of MRDTs available on the European market [36, 37, 51, 52]. No studies about diagnostic accuracies of MRDTs in the setting of imported childhood malaria are available, though MRDT performances are assumed not to be different in children compared to adults [42].
For the diagnosis of P. falciparum, MRDTs approach a sensitivity of 100% but they perform less well below parasite densities of 100/μl (corresponding to 0.002% of RBCs). This detection limit generally is above the threshold of expert microscopy (50/μl) but below that of routine microscopy in non-endemic settings, which has been shown to be close to 500/μl [40]. Of note, however, non-immune travelers can present with symptoms below a parasite density of 100/μl parasite density [42].
Concerns have risen about rare but persistent reports of false-negative MRDT results at higher parasite densities. One of the explanations is the hrp gene deletions that have been found in P. falciparum samples in the Peruvian Amazon [15]. These parasites do not secrete HRP-2, thereby impeding diagnosis by HRP-2-based MRDTs. Further, MRDTs may generate false-negative results in cases of high parasite densities (>5% of RBCs infected). This is the so-called prozone effect, caused by an excess of antigen blocking the binding sites of both detection and capture antibodies [17].
For the non-falciparum species, reported diagnostic sensitivities vary more and are lower than for P. falciparum [38]. Several MRDT brands have been evaluated at our institute on stored whole blood samples. Reported sensitivities for P. vivax ranged from 66.0% to 92.9% with false-negative results especially occurring at low parasite densities [36, 37, 51, 52]. For P. ovale and P. malariae, sensitivities were 5.5–80.0% and 21.4–45.2%, respectively [36, 37, 51, 52]. The lower diagnostic sensitivities for P. ovale and P. malariae are well known and might be explained by the lower affinity of some monoclonal antibodies to these species [22]. Though MRDTs can be of help in the diagnosis of malaria, they cannot be used to reliably exclude the non-falciparum species, especially P. ovale and P. malariae.
Malaria rapid diagnostic tests are not fail-proof and have inherent weaknesses
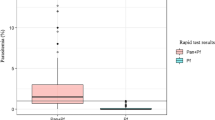
Although useful in the diagnosis of malaria and for the species identification of P. falciparum, MRDTs do not provide a reliable indication about parasite density. In addition, the HRP-2 antigen may persist for weeks after treatment and clearing of the parasites [38, 40, 42, 66], giving rise to apparent false-positive results. Limitations may also arise in performance and interpretation. For instance, problems can occur with the blood transfer device supplied with the MRDT kit (a loop, pipette or a straw—Fig. 3) which may be too small to manipulate accurately [64], reason why we advice a transfer pipette. Disregarding faint test lines as negative results is a frequent error among end users [46], and this is of concern as faint test lines (which are barely visible to the naked eye) may occur in 17.8% of all positive test lines [37]. Further, reading beyond the recommended reading time must be avoided as this may cause false-positive results [56]. Finally, inadequacies in MRDT package, labeling, and test instructions have been reported also among CE-labeled kits [18, 19], which might limit accurate performance and/or test interpretation by end users.
The diagnostic strategy, some comments
There is a tendency among clinical laboratories in non-endemic settings to rely on MRDTs as the single tool for the diagnosis of malaria (especially outside office hours), but for reasons of their limitations, MRDTs should only be used as an adjunct to microscopy. The clinician, who in some cases decides about which laboratory analyses is going to be performed for the diagnosis of malaria, should request both microscopy and MRDTs when filling in the laboratory request form [18].
Non-immune children may present with symptoms at parasite densities below the detection thresholds of both microscopy and MRDTs. Therefore, laboratory testing after unexpected negative results should be repeated. Repeat testing has been advised every 8–12 h for at least three consecutive samplings [13, 14, 67]. Of note, there is no need to await a next peak of fever to repeat microscopy or MRDT testing [42].
Conclusion
From the above, it is clear that a high index of clinical suspicion and close communication with the laboratory are clues to the timely diagnosis of malaria. VFR children, immigrants, and refugees belong to the highest risk group. Malaria may present months after leaving an endemic area, also in case of P. falciparum. Microscopy remains the cornerstone of diagnosis and provides information about parasite density and Plasmodium species. It can be complemented by MRDTs which are accurate for the diagnosis and distinction of P. falciparum but lack sensitivity for the diagnosis of the non-falciparum species. Repeat testing is recommended in case of negative laboratory tests and persistent suspicion of malaria.
References
Arnaez J, Roa MA, Albert L, Cogollos R, Rubio JM, Villares R, Alarabe A, Cervera A, Lopez-Velez R (2010) Imported malaria in children: a comparative study between recent immigrants and immigrant travelers (VFRs). J Travel Med 17:221–227
Briggs C, Da Costa A, Freeman L, Aucamp I, Ngubeni B, Machin SJ (2006) Development of an automated malaria discriminant factor using VCS technology. Am J Clin Pathol 126:691–698
Castela F, Legros F, Lagardere B (2003) Imported malaria in children in France. Arch Pediatr 10:758–765
Chalumeau M, Holvoet L, Cheron G, Minodier P, Foix-L'Helias L, Ovetchkine P, Moulin F, Nouyrigat V, Breart G, Gendrel D (2006) Delay in diagnosis of imported Plasmodium falciparum malaria in children. Eur J Clin Microbiol Infect Dis 25:186–189
Cnops L, Boderie M, Gillet P, Van Esbroeck M, Jacobs J (2011) Rapid diagnostic tests as a source of DNA for Plasmodium species-specific real-time PCR. Malar J 10:67
Cnops L, Jacobs J, Van Esbroeck M (2010) Validation of a four-primer real-time PCR as a diagnostic tool for single and mixed Plasmodium infections. Clin Microbiol Infect doi:10.1111/j.1469-0691.2010.03344.x
Cnops L, Van Esbroeck M, Bottieau E, Jacobs J (2010) Giemsa-stained thick blood films as a source of DNA for Plasmodium species-specific real-time PCR. Malar J 9:370
Crawley J, Chu C, Mtove G, Nosten F (2010) Malaria in children. Lancet 375:1468–1481
D'Ortenzio E, Godineau N, Fontanet A, Houze S, Bouchaud O, Matheron S, Le Bras J (2008) Prolonged Plasmodium falciparum infection in immigrants, Paris. Emerg Infect Dis 14:323–326
Drakeley C, Reyburn H (2009) Out with the old, in with the new: the utility of rapid diagnostic tests for malaria diagnosis in Africa. Trans R Soc Trop Med Hyg 103:333–337
Driessen GJ, Pereira RR, Brabin BJ, Hartwig NG (2008) Imported malaria in children: a national surveillance in the Netherlands and a review of European studies. Eur J Public Health 18:184–188
Dubos F, Dauriac A, El Mansouf L, Courouble C, Aurel M, Martinot A, Hospital Network for Evaluating the Management of Common Childhood Diseases (2010) Imported malaria in children: incidence and risk factors for severity. Diagn Microbiol Infect Dis 66:169–174
Farcas GA, Zhong KJ, Lovegrove FE, Graham CM, Kain KC (2003) Evaluation of the Binax NOW ICT test versus polymerase chain reaction and microscopy for the detection of malaria in returned travelers. Am J Trop Med Hyg 69:589–592
Forney JR, Wongsrichanalai C, Magill AJ, Craig LG, Sirichaisinthop J, Bautista CT, Miller RS, Ockenhouse CF, Kester KE, Aronson NE, Andersen EM, Quino-Ascurra HA, Vidal C, Moran KA, Murray CK, DeWitt CC, Heppner DG, Kain KC, Ballou WR, Gasser RA Jr (2003) Devices for rapid diagnosis of malaria: evaluation of prototype assays that detect Plasmodium falciparum histidine-rich protein 2 and a Plasmodium vivax-specific antigen. J Clin Microbiol 41:2358–2366
Gamboa D, Ho MF, Bendezu J, Torres K, Chiodini PL, Barnwell JW, Incardona S, Perkins M, Bell D, McCarthy J, Cheng Q (2010) A large proportion of P. falciparum isolates in the Amazon region of Peru lack pfhrp2 and pfhrp3: implications for malaria rapid diagnostic tests. PLoS ONE 5:e8091
Garbash M, Round J, Whitty CJ, Chiodini PL, Riordan FA, Shingadia D, Ladhani S (2010) Intensive care admissions for children with imported malaria in the United Kingdom. Pediatr Infect Dis J 29:1140–1142
Gillet P, Mori M, Van Esbroeck M, Van den Ende J, Jacobs J (2009) Assessment of the prozone effect in malaria rapid diagnostic tests. Malar J 8:271
Gillet P, Mukadi P, Vernelen K, Van Esbroeck M, Muyembe JJ, Bruggeman C, Jacobs J (2010) External quality assessment on the use of malaria rapid diagnostic tests in a non-endemic setting. Malar J 9:359
Gillet P, Maltha J, Hermans V, Ravinetto R, Bruggeman C, Jacobs J (2011) Malaria rapid diagnostic kits: quality of packaging, design and labeling of boxes and components and readability and accuracy of information inserts. Malar J 10:39
Giobbia M, Tonon E, Zanatta A, Cesaris L, Vaglia A, Bisoffi Z (2005) Late recrudescence of Plasmodium falciparum malaria in a pregnant woman: a case report. Int J Infect Dis 9:234–235
Greenwood T, Vikerfors T, Sjoberg M, Skeppner G, Farnert A (2008) Febrile Plasmodium falciparum malaria 4 years after exposure in a man with sickle cell disease. Clin Infect Dis 47:e39–e41
Grobusch MP, Hanscheid T, Zoller T, Jelinek T, Burchard GD (2002) Rapid immunochromatographic malarial antigen detection unreliable for detecting Plasmodium malariae and Plasmodium ovale. Eur J Clin Microbiol Infect Dis 21:818–820
Guedes S, Siikamaki H, Kantele A, Lyytikainen O (2010) Imported malaria in Finland 1995 to 2008: an overview of surveillance, travel trends, and antimalarial drug sales. J Travel Med 17:400–404
Gutman J, Guarner J (2010) Pediatric malaria: 8-year case series in Atlanta, Georgia, and review of the literature. J Travel Med 17:334–338
Haditsch M (2004) Quality and reliability of current malaria diagnostic methods. Travel Med Infect Dis 2:149–160
Hanscheid T (1999) Diagnosis of malaria: a review of alternatives to conventional microscopy. Clin Lab Haematol 21:235–245
Hanscheid T (2003) Current strategies to avoid misdiagnosis of malaria. Clin Microbiol Infect 9:497–504
Hay F, Treluyer JM, Orbach D, Jouvet P, Hubert P (2000) Severe malaria in children in intensive care. National survey 1990–1995. Arch Pediatr 7:1163–1170
Hennequin C, May F, Treluyer J, Druilhe P, Valensi F, Pays J (1996) Les difficultés diagnostiques du paludisme d’aéroport. Hématologie 2:329–333
Isaacson M (1989) Airport malaria: a review. Bull World Health Organ 67:737–743
Kettelhut MM, Chiodini PL, Edwards H, Moody A (2003) External quality assessment schemes raise standards: evidence from the UKNEQAS parasitology subschemes. J Clin Pathol 56:927–932
Kuhn SM, McCarthy AE (2006) Paediatric malaria: what do paediatricians need to know? Paediatr Child Health 11:349–354
Ladhani S, Aibara RJ, Riordan FA, Shingadia D (2007) Imported malaria in children: a review of clinical studies. Lancet Infect Dis 7:349–357
Ladhani S, Garbash M, Whitty CJ, Chiodini PL, Aibara RJ, Riordan FA, Shingadia D (2010) Prospective, national clinical and epidemiologic study on imported childhood malaria in the United Kingdom and the Republic of Ireland. Pediatr Infect Dis J 29:434–438
Malaria Plasmodium life-cycle and natural history of malaria. Available at http://www.malariajournal.com/graphics/videos/plasmodium_cycle.asp
Maltha J, Gillet P, Bottieau E, Cnops L, van Esbroeck M, Jacobs J (2010) Evaluation of a rapid diagnostic test (CareStart Malaria HRP-2/pLDH (Pf/pan) Combo Test) for the diagnosis of malaria in a reference setting. Malar J 9:171
Maltha J, Gillet P, Cnops L, Bottieau E, Van Esbroeck M, Bruggeman C, Jacobs J (2011) Evaluation of the rapid diagnostic test SDFK40 (Pf-pLDH/pan-pLDH) for the diagnosis of malaria in a non-endemic setting. Malar J 10:7
Marx A, Pewsner D, Egger M, Nuesch R, Bucher HC, Genton B, Hatz C, Juni P (2005) Meta-analysis: accuracy of rapid tests for malaria in travelers returning from endemic areas. Ann Intern Med 142:836–846
Mascarello M, Allegranzi B, Angheben A, Anselmi M, Concia E, Lagana S, Manzoli L, Marocco S, Monteiro G, Bisoffi Z (2008) Imported malaria in adults and children: epidemiological and clinical characteristics of 380 consecutive cases observed in Verona, Italy. J Travel Med 15:229–236
Moody A (2002) Rapid diagnostic tests for malaria parasites. Clin Microbiol Rev 15:66–78
Mueller I, Galinski MR, Baird JK, Carlton JM, Kochar DK, Alonso PL, del Portillo HA (2009) Key gaps in the knowledge of Plasmodium vivax, a neglected human malaria parasite. Lancet Infect Dis 9:555–566
Murray CK, Gasser RA Jr, Magill AJ, Miller RS (2008) Update on rapid diagnostic testing for malaria. Clin Microbiol Rev 21:97–110
NCCLS (2008) Laboratory diagnosis of blood-borne parasitic disease; approved guideline. NCCLS document M15-A
Newman RD, Parise ME, Barber AM, Steketee RW (2004) Malaria-related deaths among U.S. travelers, 1963–2001. Ann Intern Med 141:547–555
Padial MM, Subirats M, Puente S, Lago M, Crespo S, Palacios G, Baquero M (2005) Sensitivity of laser light depolarization analysis for detection of malaria in blood samples. J Med Microbiol 54:449–452
Rennie W, Phetsouvanh R, Lupisan S, Vanisaveth V, Hongvanthong B, Phompida S, Alday P, Fulache M, Lumagui R, Jorgensen P, Bell D, Harvey S (2007) Minimising human error in malaria rapid diagnosis: clarity of written instructions and health worker performance. Trans R Soc Trop Med Hyg 101:9–18
Schlagenhauf P, Steffen R, Loutan L (2003) Migrants as a major risk group for imported malaria in European countries. J Travel Med 10:106–107
Singh B, Kim Sung L, Matusop A, Radhakrishnan A, Shamsul SS, Cox-Singh J, Thomas A, Conway DJ (2004) A large focus of naturally acquired Plasmodium knowlesi infections in human beings. Lancet 363:1017–1024
Stager K, Legros F, Krause G, Low N, Bradley D, Desai M, Graf S, D'Amato S, Mizuno Y, Janzon R, Petersen E, Kester J, Steffen R, Schlagenhauf P (2009) Imported malaria in children in industrialized countries, 1992–2002. Emerg Infect Dis 15:185–191
Theunissen C, Janssens P, Demulder A, Nouboussie D, Van-Esbroeck M, Van-Gompel A, Van-Denende J (2009) Falciparum malaria in patient 9 years after leaving malaria-endemic area. Emerg Infect Dis 15:115–116
Van der Palen M, Gillet P, Bottieau E, Cnops L, Van Esbroeck M, Jacobs J (2009) Test characteristics of two rapid antigen detection tests (SD FK50 and SD FK60) for the diagnosis of malaria in returned travellers. Malar J 8:90
van Dijk DP, Gillet P, Vlieghe E, Cnops L, van Esbroeck M, Jacobs J (2009) Evaluation of the Palutop+4 malaria rapid diagnostic test in a non-endemic setting. Malar J 8:293
van Rijckevorsel GG, Sonder GJ, Geskus RB, Wetsteyn JC, Ligthelm RJ, Visser LG, Keuter M, van Genderen PJ, van den Hoek A (2010) Declining incidence of imported malaria in the Netherlands, 2000–2007. Malar J 9:300
West NS, Riordan FA (2003) Fever in returned travellers: a prospective review of hospital admissions for a 2(1/2) year period. Arch Dis Child 88:432–434
Wever PC, Henskens YM, Kager PA, Dankert J, van Gool T (2002) Detection of imported malaria with the Cell-Dyn 4000 hematology analyzer. J Clin Microbiol 40:4729–4731
WHO (2003) Malaria rapid diagnosis, making it work
WHO (2005) International health regulations. Available at http://www.who.int/ihr
WHO (2009) Malaria rapid diagnostic test performance. Results of WHO product testing of malaria RDTs: round 1 (2008)
WHO (2009) World malaria report 2009
WHO (2010) Basic malaria microscopy—part I. Learner's guide, 2nd edn
WHO (2010) Guidelines for the treatment of malaria, 2nd edn
WHO (2010) International travel and health
WHO (2010) Malaria rapid diagnostic test performance. Results of WHO product testing of malaria RDTs: round 2 (2009)
Wiese L, Bruun B, Baek L, Friis-Moller A, Gahrn-Hansen B, Hansen J, Heltberg O, Hojbjerg T, Hornstrup MK, Kvinesdal B, Gomme G, Kurtzhals JA (2006) Bedside diagnosis of imported malaria using the Binax Now malaria antigen detection test. Scand J Infect Dis 38:1063–1068
Williams JP, Chitre M, Sharland M (2002) Increasing Plasmodium falciparum malaria in southwest London: a 25 year observational study. Arch Dis Child 86:428–430
Wongsrichanalai C, Barcus MJ, Muth S, Sutamihardja A, Wernsdorfer WH (2007) A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT). Am J Trop Med Hyg 77:119–127
Wyler DJ (1993) Malaria: overview and update. Clin Infect Dis 16:449–456
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.