
Abstract
Purpose
Textbook outcome (TO) is a composite measure of outcome and provides superior assessment of quality of care after surgery. TO after major living donor hepatectomy (MLDH) has not been assessed. The objective of this study was to determine the rate of TO and its associated factors, after MLDH.
Methods
This was a single center retrospective review of living liver donors who underwent MLDH between 2012 and 2021 (n = 1022). The rate of TO and its associated factors was determined.
Results
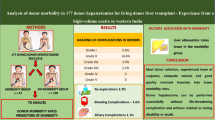
Among 1022 living donors (of whom 693 [67.8%] were males, median age 26 [range, 18–54] years), TO was achieved in 714 (69.9%) with no donor mortality. Majority of donors met the cutoffs for individual outcome measures: 908 (88.8%) for no major complications, 904 (88.5%) for ICU stay ≤ 2 days, 900 (88.1%) for hospital stay ≤ 10 days, 990 (96.9%) for no perioperative blood transfusion, 1004 (98.2%) for no 30-day re-admission, and 1014 (99.2%) for no post-hepatectomy liver failure. Early donation era (before streamlining of donor operative pathways) was associated with failure to achieve TO [OR 1.4, CI 1.1–1.9, P = 0.006]. TO was achieved in 506/755 (67%) donors in the early donation era versus 208/267 (77.9%) in the later period (P = 0.001).
Conclusion
Despite zero mortality and low complication rate, TO was achieved in approximately 70% donors. TO was modifiable and improved with changes in donor operative pathway.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Post-operative outcomes are an important determinant of healthcare quality. Traditionally, individual measures like morbidity, mortality, hospital stay, and re-admission have been used to assess hospital performance [1]. These individual measures might not capture the multidimensional recovery process in surgical patients. Hospitals might perform well in some while do poorly in other individual metrics. As a result, surgical procedures with low morbidity and mortality might be considered absolutely safe, despite considerable rates of patient dissatisfaction [2].
It has been suggested that composite measures of quality might be superior to individual outcome measures [3, 4]. A desirable outcome is achieved when all these parameters are met in an individual patient. This “all or none approach” to patient care substantially raises the bar, and forms the basis for the newly proposed term text book outcomes (TO) in surgery [5]. The term was first described in 2013 by a group of colorectal surgeons in Netherlands [6]. Recent reports suggest that TO is achieved in 25.5 to 62.3% patients undergoing liver resections. Various patient-, procedural-, and tumor-related factors contribute towards achieving TO in these patients [1] [7,8,9].
In living liver donation (LLD), complex liver surgery is performed with a very low anticipated morbidity and negligible mortality. LLD is based upon the principle of double equipoise which states that the benefit to the recipient must be balanced against the risk to the donor [10, 11]. Worldwide living donor liver transplant (LDLT) programs use stringent criteria for donor selection. This mitigates many patient and procedural factors that might negatively impact outcomes after LLD. For example, donors are young (18–55 years) and healthy, have normal liver function, and retain a minimum acceptable future liver remnant (≥ 30%) to be eligible for donation [12]. Nevertheless, serious morbidity and mortality are reported in 15–20% and 0.5% donors undergoing major hepatectomy respectively [13, 14]. LLD is a major surgical intervention with the sole purpose of saving a loved one’s life. With existing barriers to LLD and ongoing organ shortage, it is important to identify gaps that might negatively impact donor’s experience during the donation process. To this end, assessment of TO can improve quality of care in liver donors, thereby promoting the spirit of donation in other members of the community.
So far, TO have not been reported after major living donor hepatectomy (MLDH). The objective of the current study was to assess TO after MLDH and identify factors associated with TO.
Materials and methods
Study population and data collection
Between April 2012 and July 2021, 1037 living donor hepatectomies (LDH) were performed at our center. These included right hepatectomy (n = 971), left hepatectomy (n = 51), and left lateral hepatectomy (n = 15). Donors were healthy, 18–55 years of age, blood group compatible, and related to the recipient (legal or blood relation).The stepwise donor workup has been discussed elsewhere [15]. The decision to proceed with donation was made by the hospital ethics committee and human organ transplant authority. A donor was considered to have undergone MLDH when the procured graft included ≥ 3 Couinaud segments i.e. right (segments 5, 6, 7, 8) or left (segments 2, 3, 4) hepatectomy [16]. For this study, we reviewed our donor database and all consecutive donors who underwent MLDH (n = 1022) were included.
Textbook outcome
The TO for this study was based on six outcome variables: ICU stay (≤ 2 days), hospital stay (HS) (≤ 10 days), no 30-day major complications, no post-hepatectomy liver failure (PHLF), no perioperative blood transfusion, and no 30-day re-admission. Since there was no post-operative mortality in our cohort, we did not include this as an outcome measure. We used Clavien-Dindo classification for complications and grade 3 and above complications were considered as major complications [17]. Major complications, re-admissions, blood transfusions, and HS have been used previously to determine TO [1, 2] [7, 8]. We included PHLF as an additional outcome measure since it is important for donor wellbeing to have predictable and re-assuring liver functions in the early post-donation period. We used 50–50 criteria to define PHLF since it was simple, liver specific, and easier to calculate when working on a retrospective cohort [18]. We used ICU stay ≤ 2 days and hospital stay ≤ 10 days to define TO as per our institutional policy. With an uneventful postoperative course, donors who underwent a MLDH were shifted from ICU in ≤ 2 days and were discharged in ≤ 10 days of hospital admission. More specifically, once a donor was vitally stable, on room air, mobilizing out of bed, with re-assuring laboratory investigations, a discharge from ICU was considered. Discharge from the hospital was considered once the donor was on regular diet, pain free, had normal or down trending liver functions, and no signs of active infection or any other complications.
We included ICU stay as an additional measure besides hospital stay since prolonged ICU stay is independently associated with poor outcomes after surgery [19, 20]. When all six desired outcomes were met, the donor was considered to have achieved a TO.
Statistical analysis
Categorical variables were presented as frequencies. Based on normal distribution, continuous variables were presented as median and interquartile ranges (IQR) or mean and standard deviation (SD). Demographics (age, sex, BMI) and liver related variables (liver attenuation index (LAI), FLR, hepatitis B core antibody positivity, and graft type) were compared between donors who achieved a TO outcome (TO +) or did not (TO −). The LAI was calculated as the hepatic-to-splenic attenuation ratio, which is obtained by dividing the value of hepatic attenuation by the value of splenic attenuation on noncontract CT scan. LAI is reduced when there is significant liver steatosis. When LAI is 0 or less, it represents significant steatosis and donors with LAI < 1 are not accepted for donation. From January 2019 onwards, certain modifications were introduced in the donor operative pathway (Fig. 1). In order to assess the impact of these modifications, TO was compared in the early (April 2012–December 2018) and late donation era (January 2019-June 2021) of LLD. For categorical variables, Pearson X2 test and Fischer test were used while for continuous variables, t test or Mann–Whitney U test was used. Factors like FLR, graft type, variant portal and biliary anatomy, and MHV inclusion with the graft have been associated with donor outcomes [12] [21,22,23,24,25,26]. A univariate analysis was performed using these variables and those with a P value < 0.1 were included in multivariate analysis. A P value < 0.05 was considered statistically significant for all other comparisons. The hospital ethics committee approved the study (IRB # 338–21).

Modifications in donor operative pathway implemented in January 2019
Results
Patient characteristics
Among 1022 donors (of whom 693 [67.8%] were males, median age 26 [range, 18–54] years), TO was experienced in 714 (69.9%) after MLDH. Each individual outcome measure was achieved in > 85% donors (Fig. 2). Outcome measures such as ICU stay ≤ 2 days (88.5%), HS ≤ 10 days (88.1%), and no major complications (88.8%) were achieved in < 90% of donors undergoing surgery. Abdominal collections 73/1022 (7.1%) and pleural effusions 47/1022 (4.5%) needing aspiration under image guidance, were the most frequent postoperative complications (Fig. 3). Biliary complications were seen in 20/1022 (1.9%) donors. There was a significant difference in TO with regards to FLR (P = 0.043), biliary anatomy (P = 0.04), and donation era (P = 0.001) (Table 1).

Distribution of textbook outcome by its definition. Values are 714 (69.9%) for TO, 904 (88.5%) for ICU ≤ 2 days, 900 (88.1%) for hospital stay ≤ 10 days, 1014 (99.2%) for no liver failure, 908 (88.8%) for no 30-day major complications, 1004 (98.2%) for no 30-day re-admission, 990 (96.9%) for no peri-operative blood transfusion

Post-donation 30-day complications (grade 3 and above), others (n = 4) included (re-exploration = 2, tube thoracostomy for pneumothrorax = 1, re-intubation for adult respiratory distress syndrome = 1)
Multivariate analysis
Table 2 summarizes factors associated with failure to achieve TO after MLDH on multivariate analysis. On univariate analysis, FLR (P = 0.09), donation era (P = 0.006), and biliary anatomy (P = 0.086) were associated with TO. On multivariate analysis, donors who underwent hepatectomy in the early donation era (before program modifications) had 40% increase in the risk of not experiencing TO [OR 1.4, CI 1.1–1.9, P = 0.006]. TO was achieved in 506/755 (67%) and 208/267 (77.9%) donors in the early and late donation era respectively (P = 0.001). Table 3 shows the comparison of complications and individual outcome measures in the two donation periods.
ICU stay as an outcome measure
Major complication rate (P = 0.07), perioperative blood transfusion (P = 0.003), and HS > 10 days (P < 0.001) were significantly lower in donors with shorter (≤ 2 days) ICU stay (Table 4). With exclusion of ICU stay as an outcome measure, TO would have been achieved in 77.2% (789/1022) donors.
Discussion
Major liver resections are associated with significant morbidity and TO might be achieved in less than half of the patients undergoing hepatectomy [9, 27]. To the best of our knowledge, this is the first study to look at TO as a composite measure of outcome after MLDH. Although each individual parameter was achieved in majority (> 85%) of donors after MLRH, TO was experienced only in 69.9%. We noted that with streamlining of operative pathways, a substantial increase in TO was possible.
There are no established criteria to define prolonged HS and various cutoffs on median length of stay after surgery have been used [1, 2][7,8,9]. We used HS > 10 days as a cutoff for TO since it was our hospital policy to provide extended inpatient care to living donors. Donors were discharged when they were on regular diet and free of complications with reassuring laboratory investigations. On the other hand, ICU stay has not been previously used to determine TO in hepato-pancreatic surgery. Prolonged ICU stay is associated with poor outcomes after surgery [19, 20]. ICU stay (11.5%) was the second most frequent individual outcome measure after hospital stay (11.9%) that was not met in the current study. The importance of ICU stay as an outcome measure was reflected as a substantial increase in hospital stay, blood transfusion rate, and major complications (Table 4). Therefore, ICU stay appears to be a useful early indicator of failure to achieve TO when compared with other outcome measures like hospital stay or readmission.
Various patient related (age, sex, underlying liver function) and procedural factors (extent of hepatectomy, bile duct resection) influence the probability of achieving a TO after liver surgery [7,8,9][27]. These factors are less important in LLD due to strict selection criteria. Donors are young (18–55 years), healthy, and thoroughly worked up for underlying liver disorders. Instead, factors such as low FLR, variant biliary anatomy, hepatic steatosis, and inclusion of MHV with the graft might impact donor outcomes [12] [21,22,23,24,25,26]. The minimum acceptable FLR for LLD is considered to be 30%. To improve safety of LLD, more experienced LDLT centers use an FLR cutoff of 35% with relatively older donors (> 35 years) and with mild hepatic steatosis [12]. We noted that FLR > 35% had little impact on TO. In fact, streamlining of donor operative pathways appeared to be the only predictor of TO (Table 2). From January 2019 onwards, certain changes were implemented in the operative care of our donors. There was increased sharing of operative responsibilities and instead of one surgeon supervising both donor and recipient operations, we moved to designated surgeons responsible for the entire length of the donor or the recipient operation (Fig. 1). Each supervising donor surgeon had prior operative experience of more than 150 donor hepatectomies. Traditionally, two cholangiograms were performed during the donor operation, a pre-hilar dissection cholangiogram and a completion cholangiogram (after liver transection and bile duct division). A routine third precut cholangiogram (before bile duct division) was introduced allowing more precise division of hepatic duct (Fig. 4a–b). The completion cholangiogram was assessed by two surgeons for potential leaks or narrowing. Both the donor and the recipient surgeon had to be scrubbed together at the time of graft procurement. We also adopted the policy of performing transection with MHV exposure (Fig. 4c). This technique has been proposed to reduce postoperative infections and damage to portal pedicles, preserve venous drainage and functional liver tissue [28]. In addition, modified right lobe grafts were preferred over extended grafts due to recent evidence indicating improved FLR regeneration with modified grafts [24]. We assume all these factors led to improvement in TO in the later period. In addition, cumulative experience of anesthesiology and critical care teams also played an important role in improving rate of TO. For example, more judicious use of intravenous fluids keeping central venous pressure around 5 cm of water during the perioperative period, introduction of erector spinae block alongside epidural analgesia particularly for donors who were not candidates for epidural analgesia contributed to early mobility, reduced pleural effusions, and oxygen requirements.

a Precut cholangiogram (after liver transection) with bulldog clamp applied near the confluence (yellow arrow) to identify point of division of RHD. b Completion cholangiogram with RHD stump (yellow arrow) after graft procurement to prevent biliary complications in the donor. c A modified right lobe graft with MHV exposure, segment 5 (V5) and segment 8 (V8) veins will be ligated and used for reconstruction
A significant difference was observed between the two eras for ICU and hospital stay, abdominal collections, and wound infections (Table 3). The rates of biliary complications (2.1% to 1.5%), pleural effusions (4.5% to 3.7%), and blood transfusions (3.4% to 1.9%) also reduced in the later era, but the difference was not significant due to smaller number of these events. Contrary to this, there was an increase in re-admission rate in the later era. This can be attributed to the impact of COVID-19. Access to hospitals, healthcare professionals, and transportation was difficult during this time [29]. As a result, we kept a lower threshold for re-admission after LLD. Donors who presented with fever, any respiratory symptoms, or other signs of infection were more likely to be re-admitted when compared with pre COVID era.
Despite zero mortality, we noted that certain deviations from the normal postoperative course including prolonged ICU stay, hospital stay, interventions for biliary complications, and blood transfusions were associated with increased anxiety among donors and their respective families. Considering that LDLT is the only mode of donation in certain regions of the world, it is important that living donors play their role in promoting donation in the community. For this to happen, there is a need to reduce deviation from the ideal postoperative course in healthy voluntary donors. We believe that LDLT centers should strive to achieve a TO in all donors.
There are certain limitations of the current study. The study reports TO from an exclusively LDLT center and the results should be judiciously applied to centers with simultaneous deceased and living donor liver transplant activity. Although streamlining of donor operation significantly improved outcomes, it is not clear which single factor out of all modifications was most crucial. During the later period, there was more rigorous implementation of certain steps pertaining to operative pathway; however, these were not completely new and were partially practiced before streamlining as well. For example, while factors such as designated donor surgeon, 2 surgeon graft procurement, precut cholangiogram, and MHV exposure were only introduced in the later period, modified right lobe grafts were used previously although MHV exposure was not necessary. It is also difficult to ascertain how the increasing experience of the surgical and non-surgical teams contributed to TO. In addition, the cutoff on ICU and hospital stay is center-specific and cannot be generalized. In fact, some donors might be discharged as early as POD 4 after donation but are kept in hospital in view of increased donor safety. As such, the ideal cutoffs are difficult to establish in LDLT. Moreover, it is also important to assess the impact of TO in donors on recipients in future research. This single center analysis merits validation in multicenter studies, yet enables in depth assessment of changing practices and how they impact outcomes in an LDLT program.
Conclusion
Despite achieving individual outcome measures in majority of donors, the overall rate of TO is only acceptable. TO is a simple composite measure of patient care that allows identification of gaps in delivered quality of surgical care. It can be used as a shared decision making tool enabling clinicians and potential donors to have realistic expectations and identify ways to improve the overall surgical experience. More importantly, TO is modifiable, and larger multicenter studies are needed to identify factors that increase rate of TO after LLD.
Data availability
The data was analyzed anonymously.
References
Merath K, Chen Q, Bagante F, Alexandrescu S, Marques HP, Aldrighetti L et al (2019) A multi-institutional international analysis of textbook outcomes among patients undergoing curative-intent resection of intrahepatic cholangiocarcinoma. JAMA Surg 154(6):e190571. https://doi.org/10.1001/jamasurg.2019.0571
Merath K, Chen Q, Bagante F, Beal E, Akgul O, Dillhoff M et al (2020) Textbook outcomes among medicare patients undergoing hepatopancreatic surgery. Ann Surg 271(6):1116–1123. https://doi.org/10.1097/SLA.0000000000003105
Dimick JB, Staiger DO, Baser O, Birkmeyer JD (2009) Composite measures for predicting surgical mortality in the hospital. Health Aff (Millwood) 28(4):1189–1198. https://doi.org/10.1377/hlthaff.28.4.1189
Dimick JB, Birkmeyer NJ, Finks JF, Share DA, English WJ, Carlin AM, Birkmeyer JD (2014) Composite measures for profiling hospitals on bariatric surgery performance. JAMA Surg 149(1):10–16. https://doi.org/10.1001/jamasurg.2013.4109
Nolan T, Berwick DM (2006) All-or-none measurement raises the bar on performance. JAMA 295(10):1168–70. https://doi.org/10.1001/jama.295.10.1168
Kolfschoten NE, Kievit J, Gooiker GA, van Leersum NJ, Snijders HS, Eddes EH et al (2013) Focusing on desired outcomes of care after colon cancer resections; hospital variations in ‘textbook outcome.’ Eur J Surg Oncol 39(2):156–163. https://doi.org/10.1016/j.ejso.2012.10.007
Tsilimigras DI, Sahara K, Moris D, Mehta R, Paredes AZ, Ratti F et al (2020) Assessing textbook outcomes following liver surgery for primary liver cancer over a 12-year time period at major hepatobiliary centers. Ann Surg Oncol 27(9):3318–3327. https://doi.org/10.1245/s10434-020-08548-w
Tsilimigras DI, Mehta R, Merath K, Bagante F, Paredes AZ, Farooq A et al (2020) Hospital variation in textbook outcomes following curative-intent resection of hepatocellular carcinoma: an international multi-institutional analysis. HPB (Oxford) 22(9):1305–1313. https://doi.org/10.1016/j.hpb.2019.12.005
Tsilimigras DI, Pawlik TM, Moris D (2021) Textbook outcomes in hepatobiliary and pancreatic surgery. World J Gastroenterol 27(15):1524–1530. https://doi.org/10.3748/wjg.v27.i15.1524
Fisher RA (2021) Living donor liver transplantation: eliminating the wait for death in end-stage liver disease? Nat Rev Gastroenterol Hepatol 14(6):373–382. https://doi.org/10.1038/nrgastro.2017.2
Pomfret EA, Lodge JP, Villamil FG, Siegler M (2011) Should we use living donor grafts for patients with hepatocellular carcinoma? Ethical considerations. Liver Transpl 17(Suppl 2):S128–S132. https://doi.org/10.1002/lt.22356
Lee SG (2015) A complete treatment of adult living donor liver transplantation: a review of surgical technique and current challenges to expand indication of patients. Am J Transplant 15(1):17–38. https://doi.org/10.1111/ajt.12907
Lauterio A, Di Sandro S, Gruttadauria S, Spada M, Di Benedetto F, Baccarani U et al (2017) Donor safety in living donor liver donation: an Italian multicenter survey. Liver Transpl 23(2):184–193. https://doi.org/10.1002/lt.24651
Middleton PF, Duffield M, Lynch SV, Padbury RT, House T, Stanton P et al (2006) Living donor liver transplantation–adult donor outcomes: a systematic review. Liver Transpl 12(1):24–30. https://doi.org/10.1002/lt.20663
Dar FS, Zia H, Hafeez Bhatti AB, Rana A, Nazer R, Kazmi R et al (2016) Short term donor outcomes after hepatectomy in living donor liver transplantation. J Coll Physicians Surg Pak 26(4):272–276
Strasberg SM (2005) Nomenclature of hepatic anatomy and resections: a review of the Brisbane 2000 system. J Hepatobiliary Pancreat Surg 12(5):351–355. https://doi.org/10.1007/s00534-005-0999-7
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD et al (2009) The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 250(2):187–196. https://doi.org/10.1097/SLA.0b013e3181b13ca2
Balzan S, Belghiti J, Farges O, Ogata S, Sauvanet A, Delefosse D, Durand F (2005) The “50–50 criteria” on postoperative day 5: an accurate predictor of liver failure and death after hepatectomy. Ann Surg 242(6):824–8, discussion 828–9. https://doi.org/10.1097/01.sla.0000189131.90876.9e.
Cornellà N, Sancho J, Sitges-Serra A (2017) Short and long-term outcomes after surgical procedures lasting for more than six hours. Sci Rep 7(1):9221. https://doi.org/10.1038/s41598-017-09833-7
Mahesh B, Choong CK, Goldsmith K, Gerrard C, Nashef SA, Vuylsteke A (2012) Prolonged stay in intensive care unit is a powerful predictor of adverse outcomes after cardiac operations. Ann Thorac Surg 94(1):109–116. https://doi.org/10.1016/j.athoracsur.2012.02.010
Yuan Y, Gotoh M (2010) Biliary complications in living liver donors. Surg Today 40:411–417. https://doi.org/10.1007/s00595-009-4143-1
Kadohisa M, Inomata Y, Uto K, Hayashida S, Ohya Y, Yamamoto H et al (2021) Impact of donor age on the outcome of living-donor liver transplantation: special consideration to the feasibility of using elderly donors. Transplantation 105(2):328–337. https://doi.org/10.1097/TP.0000000000003246
Reichman TW, Sandroussi C, Azouz SM, Adcock L, Cattral MS, McGilvray ID et al (2011) Living donor hepatectomy: the importance of the residual liver volume. Liver Transpl 17(12):1404–1411. https://doi.org/10.1002/lt.22420
Varghese CT, Bharathan VK, Gopalakrishnan U, Balakrishnan D, Menon RN, Sudheer OV et al (2018) Randomized trial on extended versus modified right lobe grafts in living donor liver transplantation. Liver Transpl 24(7):888–896. https://doi.org/10.1002/lt.25014
Tan CHN, Hwang S, Bonney GK, Ganpathi IS, Madhavan K, Kow WCA (2019) The influence of the middle hepatic vein and its impact on outcomes in right lobe living donor liver transplantation. HPB (Oxford) 21(5):547–556. https://doi.org/10.1016/j.hpb.2018.09.003
Zhang S, Dong Z, Zhang M, Xia Q, Liu D, Zhang JJ (2011) Right lobe living-donor liver transplantation with or without middle hepatic vein: a meta-analysis. Transplant Proc 43(10):3773–3779. https://doi.org/10.1016/j.transproceed.2011.08.100
Virani S, Michaelson JS, Hutter MM, Lancaster RT, Warshaw AL, Henderson WG et al (2007) Morbidity and mortality after liver resection: results of the patient safety in surgery study. J Am Coll Surg 204(6):1284–1292. https://doi.org/10.1016/j.jamcollsurg.2007.02.067
Fan ST (2007) Precise hepatectomy guided by the middle hepatic vein. Hepatobiliary Pancreat Dis Int 6(4):430–434
Bhatti ABH, Nazish M, Khan NY, Manan F, Zia HH, Ilyas A et al (2021) Living donor liver transplantation during the COVID-19 pandemic: an evolving challenge. J Gastrointest Surg 25(12):3092–3098. https://doi.org/10.1007/s11605-021-05057-3
Author information
Authors and Affiliations
Contributions
Bhatti AB: study conception and design, acquisition of data, analysis and interpretation of data, drafting of manuscript, critical revision of manuscript; Naqvi W: study conception and design, acquisition of data, analysis; Ali N: study conception and design, acquisition of data, analysis; Khan NY: drafting of manuscript, critical revision of manuscript; Zia HH: drafting of manuscript, critical revision of manuscript; Faiz BY: acquisition of data, analysis and interpretation of data; Ilyas A: study conception and design, acquisition of data; Rana A: acquisition of data, drafting of manuscript, critical revision of manuscript; Khan NA: drafting of manuscript, critical revision of manuscript.
Corresponding author
Ethics declarations
Ethics approval
The hospital ethics committee of Shifa International Hospital Islamabad approved the study (IRB # 338–21).
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bhatti, A.B.H., Naqvi, W., Ali, N. et al. Textbook outcome among voluntary donors undergoing major living donor hepatectomy. Langenbecks Arch Surg 407, 2905–2913 (2022). https://doi.org/10.1007/s00423-022-02578-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-022-02578-6