
Abstract
Aims
The aim of this study was to determine prognostic factors in patients operated on for well-differentiated thyroid cancer (WDTC).
Patients and methods
A retrospective cohort study of patients with WDTC treated at our institution between 1989 and 1991 (n = 97; mean age 52.3 years, 78 females, follow-up 124.6 ± 75.1 months) was made. Multivariate analysis was performed including: age, gender, size of primary tumor, location and number of foci in thyroid tissue, clinical stage, thyroid capsule infiltration, tumor histological type, extent of surgery, prognosis based on the AGES and MACIS scores, and tumor proliferative activity based on determination of proliferating cell nuclear antigen (PCNA) and Ki-67 expression in tumor tissue and nodal metastases.
Results
The multivariate analysis showed increased relative risk (RR) of death for: age above 60 years (7.39; p < 0.001), pTm (2.94; p = 0.002), pT3 (11.83; p < 0.001), and pN1 (4.11; p < 0.001). Total thyroidectomy decreased RR of death (0.39; p = 0.023) when compared to more limited resections. Moderate and high PCNA index was associated with 48.3% and 87.5% mortality, respectively, while Ki-67 index was associated with the highest mortality rate (76%) in the group of medium values.
Conclusions
Despite good prognosis in WDTC, factors that most significantly affect overall survival rate include age, size of primary lesion and multifocal disease, presence of nodal metastases, and extent of primary surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Thyroid cancer accounts for only 1% of all malignancies, yet it is the most common endocrine tumor. Over the past two decades, the incidence of thyroid cancer has increased fourfold in females and threefold in males. Although well-differentiated thyroid cancer (WDTC) is associated with a good prognosis, in a certain group of patients it may have a fatal outcome. Early detection of lesions, selection of optimal surgical treatment in referral centers, target-oriented adjuvant therapy, and treatment monitoring significantly improve therapeutic results and quality of life in these patients [1, 2].
A group of WDTC patients with a poor prognosis may be selected following diagnosis establishment, what should affect further modification of treatment. The aim of this study was to determine prognostic factors in patients operated on for WDTC at a single institution in a 20-year follow-up.
Materials and methods
A retrospective cohort study of 97 patients treated surgically due to thyroid cancer in a single institution in the years 1989–1991 was made. The mean age of the patients was 52.3 years and the male to female ratio—4:1. Demographic characteristics of the investigated group are presented in Table 1.
Clinical stage was assessed using the seventh edition of the TNM staging system (2010) and histopathological results were classified based on reevaluation of detailed descriptions of examinations of materials stored in Hospital Records Department.
While analyzing the extent of primary surgical procedures, the authors adopted a simple division to total and subtotal thyroidectomies (total resection, subtotal resection, Dunhill’s procedure, and thyroid lobectomy with isthmectomy).
The analysis also included the extent of lymphatic system resection, determining the number of examined lymph nodes, number of involved lymph nodes, and the percentage of involved lymph nodes among examined lymph nodes. Assessment of death risk was based on two prognostic scales: AGES (age, histologic grade, extrathyroid invasion and distant metastasis, size of the primary lesion) and MACIS (metastasis, age, completeness of resection, invasion, size).
The presence and expression of proliferative antigens proliferating cell nuclear antigen (PCNA) and Ki-67 were investigated by immunocytochemical methods using monoclonal antibodies. To determine PCNA, monoclonal mouse anti-PCNA antibodies (DAKO M 879) were used. Ki-67 antigen was determined based on monoclonal antibodies (Monoclonal Mouse Anti Human Ki-67—DAKO).
Statistical analysis
The multivariate analysis was performed including: age, gender, size of primary tumor, location and number of foci in thyroid tissue, clinical stage, thyroid capsule infiltration, tumor histological type, extent of surgery, prognosis based on the AGES and MACIS scores, and tumor proliferative activity based on determination of PCNA and Ki-67 expression in tumor tissue and nodal metastases. For quantitative variables (age, mean thyroid volume, percentage of involved lymph nodes among investigated nodes, and comparison of mean follow-up), as the first step of the analysis, the conformity to normal distribution was assessed by the Shapiro–Wilk test. In variables with normal distribution, comparisons were made using the Student’s t test. In variables with oblique distribution, significance of differences was determined by the Mann–Whitney test.
The analysis also included the way particular clinical and demographic properties affected survival of thyroid cancer patients. Thus, the Kaplan–Meier curves were plotted to illustrate cumulative survival ratios in defined patient groups. To determine death risk in defined patient groups, the authors employed the Cox proportional regression model.
To determine independent death predictors in patients operated on for thyroid cancer, the stepwise Cox regression model was used. The criterion of a variable inclusion to the model was p < 0.05.
Results
The most common histological form was papillary carcinoma, accounting for slightly more than one half (51.6%) of patients operated on in the period 1989–1991 and followed by follicular cancer (28.9%) and other thyroid cancers (19.5%). The mean size of a single tumor was 35 mm, although in a large number of cases, lesions involved almost the entire thyroid lobe. Large numbers of patients demonstrated high clinical stages, with a relatively high percentage of stage III (25.8%) and stages IVa–IVc (14.4%). A larger percentage of patients had higher scores both according to MACIS (67.0%) and AGES (62.1%), what was associated with a potentially poorer prognosis.
In the years 1989–1991, subtotal thyroidectomies were predominant (81.4%). In 76.8% of cN0 patients, no lymphadenectomies were performed; the remaining 23.2% showed nodal metastases pN1. Only 3.2% were subjected to adjuvant radioiodine therapy.
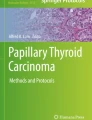
In the investigated group, the mortality rate was 52.1% (49/94 patients) over a mean follow-up of 124.6 ± 75.1 months. Mortality was found to increase with age. In the group <50 years, its value was only 12.1%, while among patients aged 60 and above—as much as 43.8% (Fig. 1). In the oldest age group, the death risk increased more than sevenfold as compared to patients below 50 years of age (p < 0.001). p value of the survival ratio at 7, 10, and 20-year time point in age groups were statistically significant: 7 years, p = 0.022; 10 years, p < 0.001; 20 years, p < 0.001.

Kaplan–Meier cumulative survival ratios in age groups
No significant risk was noted in association with gender and survival curves. However, patients with multiple lesions showed almost twofold mortality (approximately 43%) and death risk increased almost threefold.
The analysis included death risk depending on TNM cancer stage. At the time of surgery, the investigated group did not include patients with distant metastases (M0). With increasing size of primary tumors (T), mortality rates increased (from 4.8% for T1 to 52.5% for T3–T4). Patients staged as at least T3 showed an almost 11-fold increase of death risk as compared to T1 patients (p < 0.001). Death risk was significantly higher in all patients with tumors above 40 mm in size (p < 0.001). N1 patients showed a more than fourfold higher death risk (p < 0.001). In patients with 1–5 nodes involved, death risk increased more than twice (Fig. 2). No further effect of the number of involved lymph nodes on survival was seen. In patients with thyroid capsular infiltration, death risk increased more than twofold, while mortality increased from 16.9% (no capsular infiltration) to 30.6% (capsular infiltration) at a comparable follow-up. Death risk in stage II patients increased more than fourfold as compared to stage 1, and more than 50-fold in stage IV (p < 0.001; Fig. 3).

Kaplan–Meier cumulative survival ratios in TNM classification groups—N

Kaplan–Meier cumulative survival ratios in clinical stage groups
Total thyroidectomy decreased death risk by approximately 60% and intergroup differences were still marked 10 years postoperatively (Fig. 4). Local relapses were noted in 12.4%. No significant differences were noted in lymph node relapse development. Death risk based on MACIS and AGES scores pronouncedly increased, 25-fold and 20-fold, respectively (sevenfold to 25-fold) with increasing clinical stage (p < 0.001).

Kaplan–Meier cumulative survival ratios depending on extent of surgery
Analysis of survival as referred to PCNA and Ki-67 markers level showed the best prognosis in patients with low PCNA indices (72.7% survived); poorer results were seen in patients with medium PCNA indices—51.5%, and the poorest prognosis characterized patients with the highest indices (survival of only 12.5%; p < 0.001). The largest group consisted of patients with low Ki-67 indices (78%), and there, 40% of deaths were seen. The poorest prognosis and 100% mortality were observed in patients with high Ki-67 indices, yet the small number of subjects did not allow for drawing valid conclusions. However, in the investigated WDTC population, lymph node metastases were found not to be correlated with values of cell proliferation antigen indices.
Using the stepwise Cox regression model, where all the above variables were regarded as potential predictors, the authors noted that factors that significantly and irrespectively, of other variables, affected death risk were age and lymph node metastases. Having taken into consideration the confounding effect of age, metastases, clinical stage according to prognostic scales, and tumor grade measured by cell proliferation antigen indices, the authors found that total resections decreased death risk by 77%.
Discussion
The presented material includes patients treated in a single center within a defined time and analyzed over a 20-year follow-up period. Mortality was found to increase with age. All clinical observations to date confirm the above opinion, yet they do not explain the causes of the phenomenon. In adult population, death risk due to WDTC increases with age both in females and males. Elderly patients are commonly diagnosed with higher stage tumors, of more aggressive histology, often with WDTC dedifferentiation to poorly differentiated forms.
In keeping with multistage carcinogenesis theory, various phenotype variant of thyroid tumors may develop due to genetic defects of signaling cascade through oncogene activation and inactivation and consecutive mutations. Presently, the best understood form of such transformations is the theory of anaplastic carcinoma developing in a WDTC background [3, 4]. Moreover, poorer therapeutic results in elderly patients are associated with their deteriorated general state (concomitant diseases) and poorer treatment tolerance. Similar correlations have been demonstrated for prostate cancer and breast cancer [5]. Assessing the relation between age and cancer development, one must also take into consideration an increased average population age and thus, an increased time necessary for passing through particular carcinogenesis stages with molecular changes allowing for cell dedifferentiation, and carcinogenesis-favoring environmental changes combined with poor availability and quality of screening tests [6–8].
The effect of gender on the course of treatment in WDTC patients seems to be a somewhat controversial prognostic factor. Nevertheless, gender is present in all currently employed prognostic systems. A higher incidence of nodular lesions in female population is not identical with a percent increase of diagnosed malignancies. An almost twofold predominance of malignant thyroid lesions in a background of cold nodules was demonstrated in male population [9].
In the report of Sciuto et al., of more than 1,500 patients, approximately 80% were women. Of 37 mortalities, 19 deaths were noted in males [10]. Some authors suggest that a poorer prognosis in thyroid cancer in males as compared to females results from lack of a cytoprotective role played by estrogens, indicating that when menopausal disturbances develop, thyroid cancer morbidity in the population increases accompanied by an increase in the number of forms associated with poorer prognosis [11]. Nevertheless, there are also numerous reports that contradict the above observations and point to similar late therapeutic results in differentiated thyroid cancers, regardless of gender [12, 13]. Based on the present analysis, the authors did not observe a significant risk of statistically significant differences in survival curves plotted for males and females.
A thorough analysis of the relation between the primary focus size and increased death risk showed that risk values were significant for all patients with tumors sized above 40 mm. Survival curves showed that patients with tumors above 40 mm died markedly sooner and mortality rates were higher.
Primary tumors up to 1 cm in size are associated with a good prognosis, but they may have all the specific properties of malignant tumors, with nodal metastases, capsular infiltration, or multifocal growth in thyroid tissue. So et al. analyzed 551 patients with papillary thyroid carcinoma, including 203 patients with microcarcinomas. The latter showed as many as 31% of multifocal cancer with nodal metastases in approximately 24.6% and capsular infiltrations in 20.7% patients. We should thus assume that one fourth of patients, despite diagnosed thyroid papillary microcarcinomas, showed all the properties of fully symptomatic disease. The primary focus size was immaterial in patients with asymptomatic metastases to medial compartment lymph nodes [14–18].
Machens et al. observed that both multifocality (23.5%) and nodal metastases (40.2%) were markedly more common in females with papillary thyroid cancer in tumors up to 2 cm in diameter, while lesions above 20 mm more commonly gave distant metastases in patients with follicular thyroid carcinoma [19, 20]. The analysis of Bilimoria et al. showed in a very large population of thyroid papillary cancer patients in a 10-year follow-up that tumors above 1 cm in diameter were apt to relapse as much as five times more often as compared to smaller tumors [21].
In their retrospective analysis, Scheumann et al. found that routine resection of central compartment lymph nodes positively (p < 0.005) affected late survival and possibility of T1–T3 tumor relapses. According to the 2010 TNM classification, the above was true for tumors above 1 cm in diameter. The results could not have been unambiguously addressed due to lack of a control group without central compartment lymph nodes resection [22]. Thus, primary tumors above 1 cm in diameter, with a multifocal growth pattern in the form of intrathyroid lesions with numerous primary foci and capsular infiltration are associated with a poorer prognosis, especially in patients above 45 years of life, being associated with higher proneness to local relapses and distant metastases [23, 24].
Summing up the present analysis, it should be emphasized that factors that significantly and independently, of other variables, affected death risk were age and nodal metastases. Having taken into consideration the confounding effect of age, metastases, clinical stage according to prognostic scales, and tumor grade measured by cell proliferation antigen indices, the authors found that total resections decreased death risk by 77%.
References
Jarząb B, Słowińska-Klencka D (2010) Comment to recommendations: diagnostics and treatment of thyroid cancer. Endokrynol Pol 61:569–574
Ward E, Forman D (2011) Global Cancer Statistics. CA Cancer J Clin 61:69–90
Wynford TD, Jones CJ, Wyllie FS (1996) The tumour suppressor gene p53 as a regulator of proliferative life-span and tumour progression. Biol Signals 5:139–153
Fagin JA (1995) Tumor suppressor genes in human thyroid neoplasms: p53 mutations are associated undifferentiated thyroid cancers. J Endocrinol Invest 18:140–142
Allred DC, Harvey JM, Berardo M, Clark GM (1998) Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol 11:155–168
Akslen LA, Haldorsen T, Thoresen SO, Glattre E (1991) Survival and causes of death in thyroid cancer: a population-based study of 2479 cases from Norway. Cancer Res 51:1234–1241
Simpson WJ, McKinney SE, Carruthers JS, Gospodarowicz MK, Sutcliffe SB, Panzarella T (1987) Papillary and follicular thyroid cancer. Prognostic factors in 1,578 patients. Am J Med 83:479–488
DeGroot LJ, Kaplan EL, McCormick M, Straus FH (1990) Natural history, treatment, and course of papillary thyroid carcinoma. J Clin Endocrinol Metab 71:414–424
Belfiore A, La Rosa GL, La Porta GA, Giuffrida D, Milazzo G, Lupo DA et al (1992) Cancer risk in patients with cold thyroid nodules: relevance of iodine intake, sex, age, and multinodularity. Am J Med 93:363–369
Sciuto R, Romano L, Real S, Marandino F, Sperduti I, Maini CL (2009) Natural history and clinical outcome of differentiated thyroid carcinoma: a retrospective analysis of 1503 patients treated at a single institution. Ann Oncol 20:1728–1735
Cady B, Sedgwick CE, Meissner WA, Bookwalter JR, Romagosa V, Werber J (1976) Changing clinical, pathologic, therapeutic, and survival patterns in differentiated thyroid carcinoma. Ann Surg 184:541–553
Shaha AR, Shah JP, Loree TR (1996) Risk group stratification and prognostic factors in papillary carcinoma of thyroid. Ann Surg Oncol 3:534–538
Bhattacharyya N (2003) A population-based analysis of survival factors in differentiated and medullary thyroid carcinoma. Otolaryngol Head Neck Surg 128:115–123
So YK, Son YI, Hong SD, Seo MY, Baek CH, Jeong HS et al (2010) Subclinical lymph node metastasis in papillary thyroid microcarcinoma: a study of 551 resections. Surgery 148:526–531
Chow SM, Law SC, Chan JK, Au SK, Yau S, Lau WH (2003) Papillary microcarcinoma of the thyroid—prognostic significance of lymph node metastasis and multifocality. Cancer 98:31–40
Cappelli C, Castellano M, Braga M, Gandossi E, Pirola I, De Martino E et al (2007) Aggressiveness and outcome of papillary thyroid carcinoma (PTC) versus microcarcinoma (PMC): a mono-institutional experience. J Surg Oncol 95:555–560
Pellegriti G, Scollo C, Lumera G, Regalbuto C, Vigneri R, Belfiore A (2004) Clinical behavior and outcome of papillary thyroid cancers smaller than 1.5 cm in diameter: study of 299 cases. J Clin Endocrinol Metab 89:3713–3720
Gulben K, Berberoglu U, Celen O, Mersin HH (2008) Incidental papillary microcarcinoma of the thyroid—factors affecting lymph node metastasis. Langenbecks Arch Surg 393:25–29
Machens A, Holzhausen HJ, Dralle H (2005) The prognostic value of primary tumor size in papillary and follicular thyroid carcinoma. A comparative analysis. Cancer 103:2269–2273
Machens A, Holzhausen HJ, Lautenschläger C, Thanh PN, Dralle H (2003) Enhancement of lymph node metastasis and distant metastasis of thyroid carcinoma. A multivariate analysis of clinical risk factors. Cancer 98:712–719
Bilimoria KY, Bentrem DJ, Ko CY et al (2007) Extent of surgery affects survival for papillary thyroid cancer. Ann Surg 246:375–384
Scheumann GF, Gimm O, Wegener G et al (1994) Prognostic significance and surgical management of locoregional lymph node metastases in papillary thyroid cancer. World J Surg 18:559–568
Mazzaferri EL, Jhiang SM (1994) Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 97:418–428
Mazzaferri EL, Doherty GM, Steward DL (2009) The pros and cons of prophylactic central compartment lymph node dissection for papillary thyroid carcinoma. Thyroid 19:683–689
Conflicts of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was presented in the Langenbeck’s Archives of Surgery Award Session at the 15th Annual Meeting of the European Society of Surgery, November 17–19, 2011, Kraków, Poland.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Konturek, A., Barczyński, M., Nowak, W. et al. Prognostic factors in differentiated thyroid cancer—a 20-year surgical outcome study. Langenbecks Arch Surg 397, 809–815 (2012). https://doi.org/10.1007/s00423-011-0899-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-011-0899-z